
Abstract

INTRODUCTION
Adult acquired flatfoot deformity usually develops as a consequence of posterior tibial tendon dysfunction. 1–3 The posterior tibialis muscle is the strongest inverter to the hindfoot which actively inverts the heel during the heel rise phase of gait. Its antagonist, the strongest evertor of the foot, is the peroneus brevis. The unopposed pull of the peroneus brevis in patients with posterior tibial tendon dysfunction has been felt to be the primary deforming force in patients who develop adult acquired flatfoot deformity. 3 Mizel et al. 4 supported this argument by reporting on a series of patients who underwent posterior tibial tendon transfers to the dorsum of the foot to correct a foot drop gait abnormality following common peroneal nerve palsy. In their series, since none of the patients had a functioning peroneus brevis and none developed a flatfoot deformity, they postulated that the lack of this unopposed antagonist prevented the development of a flatfoot deformity. In contrast to this, in one previous report by Vertullo and Nunley, 7 a flatfoot deformity developed after a posterior tibial to dorsum transfer following common peroneal nerve injury in one patient. In this report, we present a case where a patient developed a planovalgus foot deformity following a posterior tibial dorsum transfer in a patient with Guillain-Barre syndrome residuals with nonfunctioning dorsiflexors and evertors of the foot.
CASE REPORT
A 51-year-old female presented complaining of bilateral leg weakness and right foot pain and deformity. She developed Guillain-Barre syndrome in 1970 and lost dorsiflexion and eversion strength to both sides. Two years later, due to dissatisfaction with her AFO's, she underwent a bilateral posterior tibial tendon to middle cuneiform transfer. She did not have any previous Achilles lengthening procedure. She wore the AFO's for another six years postoperatively, but since she was able to dorsiflex to neutral and was no longer stumbling, she discontinued AFO use at that time. At that time, she was able to walk up to 3 miles a day, but noted gradually increasing pain and deformity of the right foot and ankle more than 30 years after her posterior tibial tendon transfer.
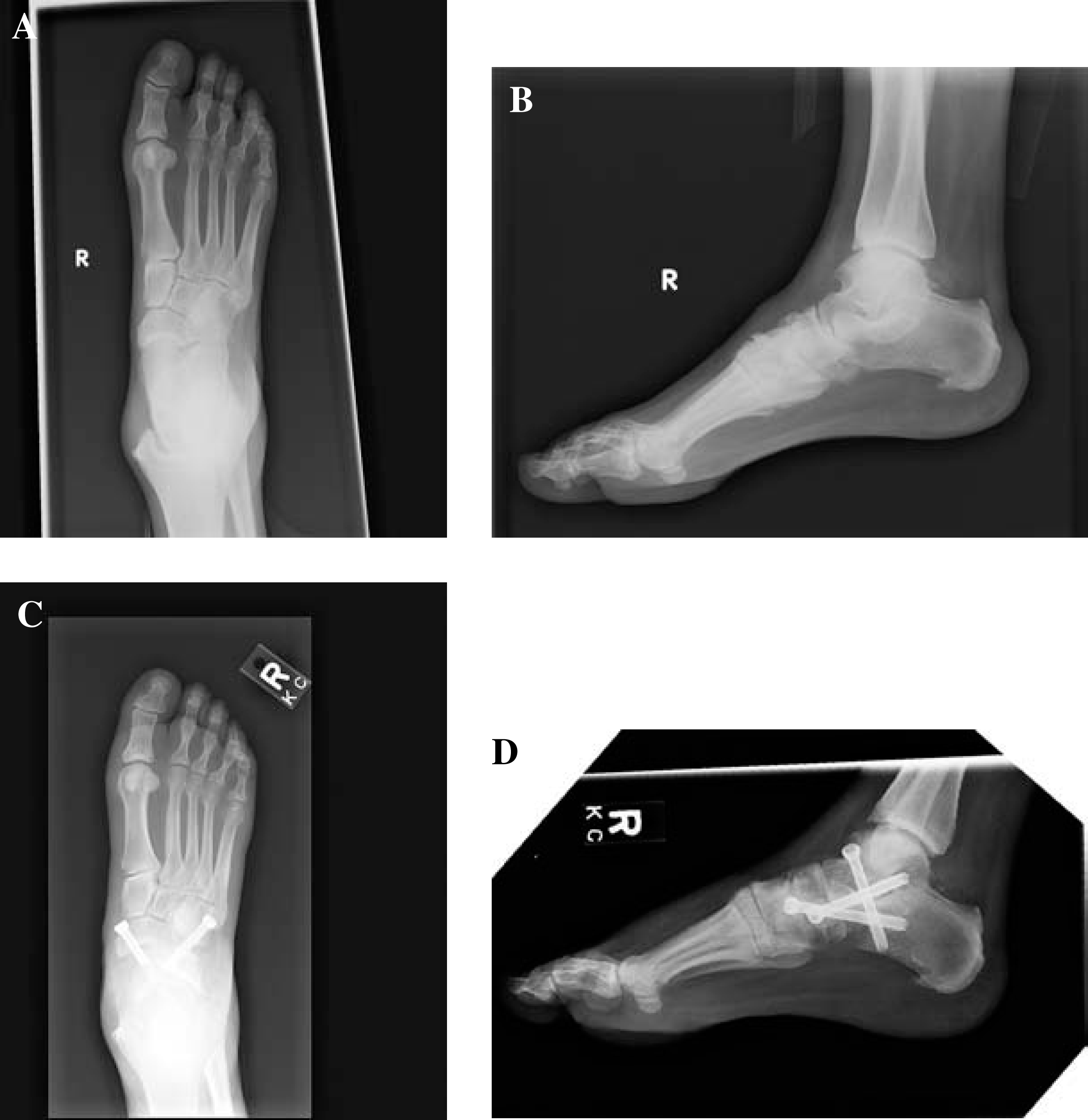
On examination, the patient was noted to have right-sided hindfoot valgus deformity of 12 degrees versus 7 degrees on the left with marked tenderness over the lateral hindfoot area. With the hindfoot held in neutral, she had a mild midfoot supination deformity but no visible abduction deformity. She had a normal, symmetric valgus alignment of both knees when standing. She had 3+/5 dorsiflexion strength. Her gait revealed no visible foot drop with mild slapping of the foot on both sides. She had no active eversion on either side. With active dorsiflexion of the right foot, her ankle dorsiflexed into neutral without significant inversion or eversion. She was unable to single-heel rise on the affected side complaining of pain and was able to heel rise on the contralateral side. With the hindfoot held in subtalar neutral position, her ankle dorsiflexed passively to 5 degrees with the knee fully extended and to 10 degrees with the knee flexed. Her left ankle dorsiflexed to 10 degrees with the knee extended and 15 degrees with the knee flexed. Despite a course of casting and camboot immobilization, the patient had persistent pain. She underwent an uncomplicated triple arthrodesis as she had a relatively rigid planovalgus deformity with no transferable tendons (Figure 1). Postoperatively, she became fully ambulatory and could single-heel rise on the affected side without pain.
DISCUSSION
The most common cause of adult acquired flatfoot deformity is posterior tibial tendon dysfunction. One potential etiology for this flatfoot deformity is the unopposed pull of the peroneus brevis, the antagonist to the posterior tibialis. 3,4 Two additional factors likely contribute to the development of a flatfoot deformity in most patients with posterior tibial tendon dysfunction. The posterior tibialis normally inverts the hindfoot during the heel rise phase of gait. Due to the lack of inversion with the dysfunctional posterior tibialis, the foot remains in an unstable, supple valgus position during heel rise allowing the gastrocnemius soleus complex to strongly evert the hindfoot. Sarafian has concluded that in a normal foot with the heel in inversion at heel rise, the Achilles tendon exerts a 48-N/m supination force on the hindfoot. This is in contrast to the tibialis posterior exerting only an 18 N/m force. With the heel in valgus such as a patient with a nonfunctional posterior tibialis, this supinating force becomes a pronating force, thus exacerbating the flatfoot deformity. 5 Another minor contribution to the flatfoot deformity is the loss of the direct arch supporting function of the posterior tibialis. A previous study by us has revealed a modest direct arch supporting effect when the posterior tibialis is tensioned in a static, neutrally aligned cadaveric ankle model. 6
In cases of common peroneal nerve palsy, both the anterior and lateral compartment musculature is nonfunctional, which leads to inability to dorsiflex the ankle or evert the hindfoot. In their report, Mizel et al. showed that in 10 patients, no one developed a flatfoot deformity following posterior tibial tendon transfer, and they postulated that it was only the unopposed pull of the peroneus brevis which led to the flatfoot deformity in patients with posterior tibial tendon dysfunction. 4 In that study, they only had a 74.9 (range, 18 to 351)-month average followup. The patient in the present study developed her deformity greater than 30 years after her tendon transfer. However, this case demonstrates that there is more than just the unopposed pull of the peroneus brevis contributing to the development of the flatfoot deformity. Our case is in agreement with the report of Vertullo and Nunley 7 where a patient with a common peroneal nerve palsy developed a flatfoot deformity after posterior tibial to dorsum transfer. We believe that the unopposed pull of the peroneus brevis exacerbates any dynamic valgus malalignment of the foot which then leads to a greater eversion stress on the hindfoot especially with contraction of the gastrocnemius soleus. However, in the absence of the peroneus brevis pull, the flatfoot deformity can still develop gradually as seen in this case and the case of Vertullo and Nunley.
CONCLUSION
We have demonstrated that a patient with a nonfunctional peroneus brevis who undergoes posterior tibial tendon to dorsum transfer can eventually develop a planovalgus foot deformity even in the absence of peroneus brevis function. Thus, the unopposed pull of the peroneus brevis is not the sole cause of a flatfoot deformity in patients with posterior tibial tendon dysfunction. However, in the absence of the peroneus brevis tension, the flatfoot deformity may develop over a much longer period of time. We agree with Vertullo and Nunley 7 that patients should be warned there is a slight risk of developing a flatfoot deformity after this tendon transfer. Likewise, it would be prudent in these patients to recommend an arch support postoperatively.