
Abstract

Introduction
Missed or chronic ruptures of the Achilles tendon present a unique treatment challenge for the treating physician and, if left untreated, can cause significant dysfunction for the patient.
What constitutes a delayed or missed diagnosis rupture is not well defined. Different terminology has been used to describe this condition and its treatment, including chronic rupture, neglected rupture, late or old repair, and delayed reconstruction. Dalton 6 suggested acute injuries should be defined as being diagnosed and treated at less than 48 hours. Gabel and Manoli 10 and Porter et al. 20 stated that 4 weeks is the interval cited most often between rupture and repair for the condition to be considered “late.” Myerson 19 stated that if treatment is delayed for 6 weeks after rupture, the expected outcome could not parallel the results had the repair been performed more expeditiously, though he thought this depended on the extent of the gap between the tendon ends and the potential for muscle recovery.
While there is no definite consensus on when an Achilles tear becomes late or chronic, the end result is a gap between the tendon ends that cannot be apposed by simple plantar flexion of the foot. Filling of this gap requires some form of tissue reconstruction.
The most common reason for delayed treatment is delayed diagnosis. However, long-standing tendinosis with micro rupture has been cited as secondary cause for progressive elongation of the tendon resulting in dysfunction. 6 Much of the treatment's success or failure depends on reestablishing the functional length of the muscle tendon unit. An over-lengthened triceps surae results in diminished strength and inadequate plantar flexion power reduces the stability of the ankle and impairs the resultant gait pattern. 1
The patient may not recall a specific injury and a lack of continued pain or swelling can lead to an ignoring of symptoms, thus delayed diagnosis. Patients may complain of an unsteady gait, difficulty with step climbing, a limp with ambulation, and difficulty with heel rise. Pain is an uncommon complaint.
On physical exam, a palpable gap may be present (Figure 1) and the normal tendon contour of the posterior ankle may be absent (Figure 2). Also, increased dorsiflexion excursion compared to the contralateral ankle, diminished plantarflexion strength, and weak or absent heel rise are common findings. The Thompson or Simmonds test is performed with the patient prone and the feet dangling off the edge of the exam table. The calves are squeezed and an intact Achilles will passively plantarflex the foot. The Matles “no touch” passive dorsiflexion test 16 is performed with the patient prone with the knees flexed to 90 degrees. The involved leg is notably more dorsiflexed than the normal side (Figure 3). There are two unique considerations when evaluating and treating the patient with delayed diagnosis or neglected ruptures:

Contracture of the skin over the segmental defect in a 10 week old Achilles rupture.

Visible lack of continuity of the left Achilles tendon.

Passive increase in dorsiflexion of the involved leg in the “no touch” test described by Matles with the patient placed prone and the knees flexed to 90 degrees, indicating loss of continuity of the Achilles tendon.
Skin Contracture
Contracture of the skin overlying the Achilles defect can cause difficulties with wound closure after the Achilles is reconstructed (Figure 1). Excessive tension of the soft tissue envelope over the reconstructed tendon decreases the blood flow to the tissues and increases the risk of infection and wound breakdown. There may be a role for tissue expansion prior to reconstruction if the contracture is severe. Mohammed et al. 18 reported using a tissue expander for 8 to 10 weeks in 4 patients with late presentation of an Achilles rupture to expand the skin prior to reconstruction to allow tension-free wound closure. They reported only one minor skin problem and suggested that an experienced plastic surgeon perform the first-stage procedure.
Irreducible Gap
Almost invariably, there is a gap greater than two centimeters that cannot be closed without excessive plantarflexion of the foot and ankle. What treatment or combination of treatment options available to the surgeon depends on the size of the tendon gap.14,19 Table 1 outlines the treatment options available to fill the gap and reestablish normal tension of the gastrocsoleus complex.
Options for bridging Achilles tendon gap
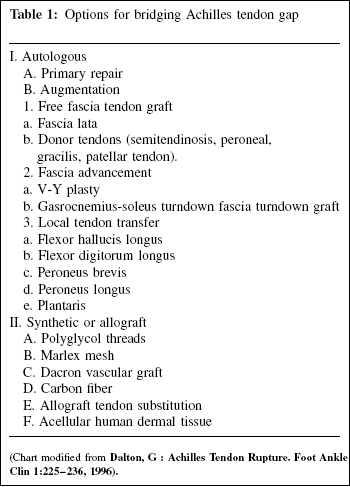
(Chart modified from
Indications
Surgical indications include persistent weakness or dysfunction. Contraindications are poor skin, uncontrolled diabetes, scarring from previous surgery, smoking, or patient desire to avoid surgery. The decision to implement treatment depends on the time elapsed since the rupture, the magnitude of the disability, the desire of the patient for improved function and risk factors associated with surgery. Nonoperative treatment, such as bracing, may be acceptable if the risks of skin or deep tissue compromise are deemed too high.
When surgery is indicated, the author prefers a combination of a fascial advancement and tendon transfer to bridge large gaps in the Achilles. A review of the literature reveals a number of level IV evidence studies reporting results of the more common techniques used to reestablish tendon continuity.
FHL Transfer Alone
Wapner et al. 23 reported 7 patients who underwent FHL transfer harvested from the midfoot and passed through the calcaneus and sutured to the ruptured ends of the Achilles tendon. All patients but one had a good or excellent result with an average of a 29.5% reduction in plantar flexion strength on Cybex testing compared to the contralateral side.
More recent studies by Den Hartog,6,7 Wilcox et al., 25 and Coull et al. 5 reported good or excellent results with an FHL transfer with proximal harvest, for tendinosis after extensive debridement. Den Hartog described a technique of harvesting the FHL tendon near the tip of the medial malleolus for chronic tendinosis. Good to excellent results were reported in 23 of 26 patients without any deficit in first toe function. A recent biomechanical study by Coull et al. 5 revealed little pressure change under the first or second MTP joint and no clinical functional deficit after FHL harvesting.
Fascial Advancement Alone
Takao et al. 21 using Cybex isokinetic testing, reported up to strength deficits up to 23% on 10 patients with neglected Achilles ruptures treated with gastrocnemius fascial flaps. Us et al. 23 reported up to 22% deficiency in peak torque in patients treated with V-Y advancement alone. Kissel et al. 13 reported up to 30% deficiencies to patients who underwent repair for smaller defects.
Porter 20 reported good results in 11 patients with gastrocnemius release with imbrication of the scar tissue without excision. No tendon transfer was performed.
Tendon Transfer and Fascial Advancement
Mann et al. 15 reported use of the FDL tendon, harvested from the midfoot, for augmentation transfer for large gaps between the proximal and distal stumps of the Achilles tendon in seven patients with neglected rupture. All seven also had a fascial turndown flap. With 39 months average followup, all patients but one had good or excellent result with no pain or limitation of activities
Elias et al. 9 reported results of 15 patients treated with FHL transfer and V-Y lengthening for neglected Achilles ruptures with gaps of 5 to 8 cm. They found a 22% loss of plantarflexion strength and a 5-degree loss of AROM, but scored an average of 94/100 for the total AOFAS hindfoot score.
Author's Prefered Technique
The goal of surgery is to restore strength and continuity of the triceps surae unit. To accomplish this, one must bridge the tendon gap and restore normal muscle tension. Currently the FHL, FDL, and peroneus brevis are the transfers most often used either to augment primary repairs or to reconstruct a neglected rupture with a gap greater than 2 to 3 cm. The importance of the peroneus brevis to lateral ankle stability and eversion of the foot makes this transfer less desirable than other tendon transfers. I use an FHL transfer for all defects over 2 cm because of its benefit of adding plantarflexion strength, which is almost always compromised with just fascial advancement alone.9,13,23
I prefer the FHL tendon over other transfers for the following reasons:
relative strength compared to other tendon transfer options,
fires in phase with the Achilles,
ease of access for transfer through the proximal harvest technique, 12
little or no functional morbidity associated with harvest, 5 and
maintenance of normal muscle balance of the ankle (i.e., plantar flexor to plantar flexor).
A number of fascial advancement options exist, the most common being gastrocnemius recession, V-Y advancement, and turndown flap. Tendon gaps 2 to 5 cm usually close adequately with gastrocnemius recession or V-Y gastroplasty (Figure 3, A and B). For gaps greater than 5 cm, I tend to use a turndown flap as it allows for greater tissue length for bridging the larger gaps. For gaps greater than 10 cm, I consider an Achilles allograft.
Surgical Technique
The technique described most closely follows that described by Gerdes 11 and the proximal harvest technique described by Hanson. 12
The anesthetized patient is placed prone on the operative table and the involved extremity prepped and draped in the usual fashion. Both extremities are draped if the surgeon chooses to use the contralateral limb for comparison in proper tensioning of the reconstructed Achilles.
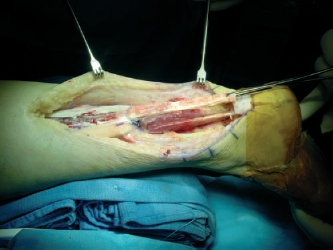
The incision is made posteromedial to the Achilles, which allows ease of access to the flexor hallucis longus tendon (FHL) for harvest. A horizontal extension of the incision in an “L” or hockey stick shape can be made if extensive debridement of the distal tendon or calcaneal tuberosity is anticipated (Figure 4). A straight posterior, tendon splitting incision has also been used effectively. 17
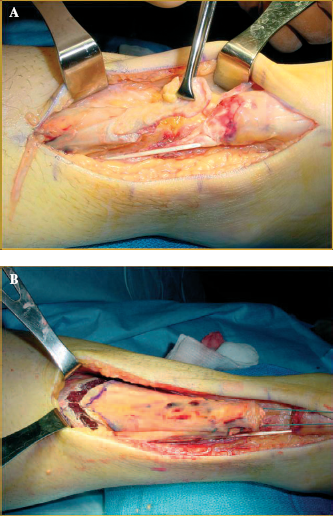
(A) 12 week old Achilles rupture with interposed scar tissue. (B) Continuity of the Achilles restored with end to end repair after gastrocnemius recession alone.
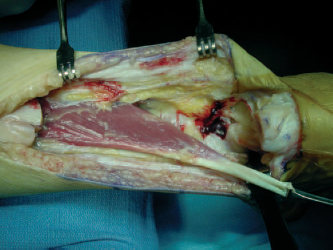
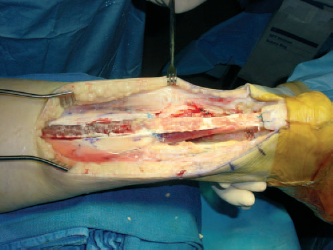
The full thickness incision should include the paratenon. Undermining of the incision should be avoided. Once the tendon gap is exposed (Figure 5) and the interposing scar tissue excised to expose more normal collagen fibers in the remaining tendon, the size of the gap is measured (Figure 6). The decision of what tissue to use for reconstruction is determined based on the defect size. Gaps greater than 3 cm or more will likely require tendon transfer in addition to the fascial advancement from the gastrocnemius tendon.

Posteromedial incision with a horizontal “L” extension for improved exposure.
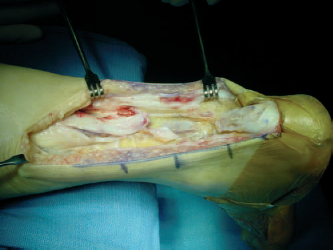
The ruptured Achilles is exposed with a full thickness incision, which includes the paratenon.
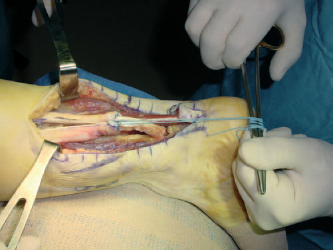
The FHL tendon and muscle are exposed by incising the deep fascia anterior to the Achilles. The tendon is followed distally along the fibrosseous tunnel where it courses along the tuberosity of the calcaneus and transected as far distal as possible with the great toe and ankle plantar flexed maximally. Care is taken to protect the neurovascular bundle by placing a blunt retractor between the neurovascular bundle and the FHL. The FHL is transected medial to lateral with a No. 15 blade to avoid inadvertent injury to the contents of the tarsal tunnel (Figure 7, A and B). The FHL is mobilized for transfer into the calcaneus (Figure 8).
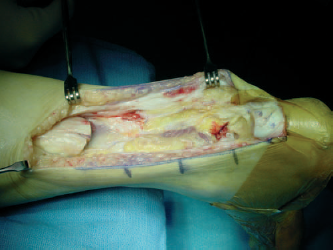
The scar tissue is debrided and the defect measured.
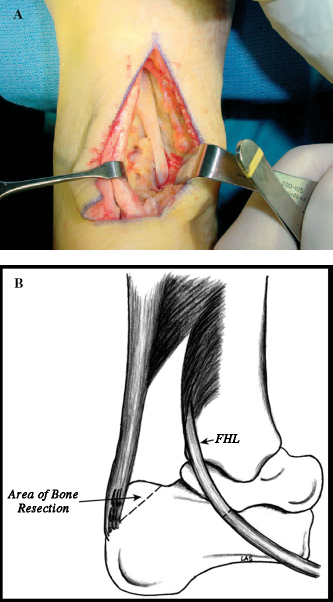
(A) Protection of the neurovascular bundle during harvest of the FHL inferior to the medial malleolus. (B) Artist drawing of level of transection of the FHL below the medial malleolus and area of calcaneal resection to make room for the tendon transfer.
The superior aspect of the calcaneal tuberosity is removed with an osteotome to make room for the FHL transfer and remove any boney impingement from the reconstructed tendon (Figure 9).
The FHL is detached from below the medial malleolus and mobilized for transfer.
A Krackow locking stitch is placed at the end of the transfered FHL. A Steinman pin with an eyelet at the proximal end is used to pass the suture ends down through a 7- to 8-mm bone tunnel drilled in the calcaneal tuberosity and out the heel. The FHL is tensioned with the ankle in about 20 degrees of plantarflexion or, if the surgeon prefers, placed in the same resting foot position as the draped contralateral limb. An interference screw (usually 7 × 23 mm) is used for fixation of the tendon in the bone tunnel. In most cases, adequate FHL tendon length is obtained using the proximal harvest technique to allow passage of the tendon far enough into the bone tunnel to allow adequate interference screw fixation (Figure 10). If there is not enough length of the FHL, a 5.0-mm cork screw double strand suture anchor can be used to secure the transfer (Figure 11).

The superior calcaneal tuberosity is removed with an osteotome.
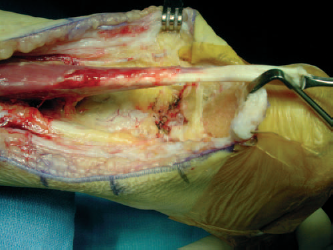
Assess for adequate length of the transferred FHL for bone tunnel interference fixation.
The gastrocnemius tendon is then exposed and the gap measured. The length of turndown needed is usually 2 cm more than the measured gap, as some length will be taken distally where the sutures are placed at the turndown point. A 10- to 12-mm wide central slip of fascia is outlined with a marking pen. All but the last 10 to 15 mm is incised and the fascia elevated from the underlying muscle in a proximal-to-distal direction using sharp dissection. A braided, nonabsorbable No. 2 suture is used on each side of the distal end of the flap to keep the turndown from pulling completely away from the main gastrocnemius fascia and muscle. The suture knots are buried to avoid irritation to the overlying soft tissue (Figure 12).
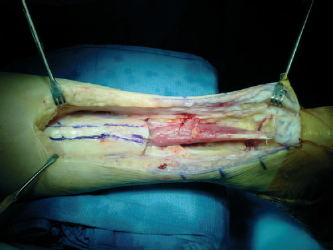
The transferred FHL is in place and the gastrocnemius fascia is marked for flap development.
It is important to assess excursion of triceps surae. If the triceps has limited excursion, I apply several minutes of longitudinal tension through the sutures applied in the distal tendon (Figure 13). I prefer draping both limbs to assess normal resting tension of the unaffected limb. The fascial flap is attached to the calcaneus anterior to the Achilles stump with suture anchors or sutured directly to the stump of the Achilles with the same tension as the transferred FHL. The turndown flap is the attached to the calcaneus with a 5.0 cork screw suture anchor and/or sutured directly to the distal remnant of the Achilles. The FHL tendon and the gastroc-turndown flap are sutured side-to-side with nonabsorbable braided suture with care to bury the knots to avoid impingement on the overlying soft tissue (Figure 14).
The fascial flap is turned downward after sutures are placed to prevent pullout.
Tension is applied for several minutes through braided nonabsorbable sutures in the distal gastrocnemius tendon to stretch the triceps surae muscle.
Careful layered closure of the soft tissues is done with interrupted fashion, with special care to cover the reconstruction with the paratenon.
Postoperative Treatment
A bulky Jones splint is applied in the operating room and removed 2 weeks post-op. The patient is then placed in a nonweightbearing cast for 4 weeks. A CAM-soled walker is applied and weight bearing as tolerated allowed. The CAM boot is weaned as swelling and pain decrease and as strength improves. Physical therapy for range of motion and strengthening is usually begun at 8 to 10 weeks.
Results of Treatment
Though the combination of FHL transfer and gastrocnemius turndown technique has been described, 4 no outcomes have been reported. My experience with this treatment combination involves 6 patients with 9- to 20-months followup for large (greater than 7 cm) segmental defects of the Achilles. All but one has had return to normal daily activity without pain. Three of the 6 patients can single-heel rise on the operated side. One obese patient avulsed the FHL transfer which had been attached to the calcaneus with a corkscrew anchor. Since that time, I have used interference screw fixation through a calcaneal bone tunnel for my heavier patients. I have had a followup MRI scan on two of the patients (at 9- and 12-months followup). Both scans revealed hypertrophy of the collagen fibers of the turned down gastrocnemius tendon (Figure 15).
The completed FHL and gastrocnemius turndown reconstruction.
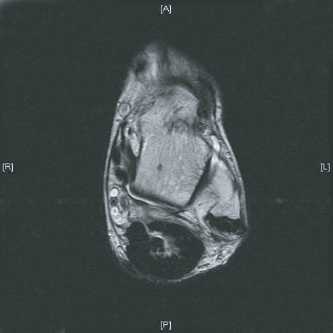
MRI showing hypertrophy of the collagen fibers of the turndown flap around the transferred FHL 9 months post-op.
Conclusion
The decision to proceed with surgical treatment depends on the magnitude of disability, the desire of the patient for improved function, and potential risk factors associated with surgery. Bracing may be an acceptable alternative if the risks of poor wound healing necessitating a free tissue transfer are too high. If the surgical risks are acceptable, the clinical results of delayed repair may be as successful as acute repair. 3 Higher level of evidence studies are needed to determine which combination of treatments will give the best chance for improved function and maximum return of strength in patients with large segmental defects of the Achilles. In general, patients can expect reasonably good function after delayed or late surgical reconstruction after neglected, late, or chronic rupture of the Achilles tendon.
Summary Points
For Achilles defects 2 to 3 cm or greater, consider using a tendon transfer along with the fascial advancement to reconstruct continuity and restore normal tension to the gastrocnemius-soleus complex.
Use a full thickness incision with care to elevate the paratenon with the skin and subcutaneous tissues.
Tendon gap size will determine options for treatment.
Harvest the FHL through the same incision and anchor it to the calcaneus through a bone tunnel using an interference screw.
Tensioning of the transferred tendon is critical and facilitated by comparison to the resting tension of the draped contralateral limb.
For larger tendon gaps, use a central slip of fascia from gastrocnemius tendon rotated 180 degrees on distal sutures to prevent pullout of the fascia. The distal part of the flap is anchored to the calcaneus anterior to the remnant of the Achilles and sutured side-to-side to the Achilles stump at maximum tension of the triceps surae.
Careful closure of the remaining paratenon is done over the reconstruction and subcutaneous and skin closure performed in layered fashion.