
Abstract
Background: Screws placed in the distal fibula may not have satisfactory purchase during internal fixation of an osteoporotic ankle fracture. Tibia-pro-fibula screws that extend from the fibula into the distal tibial metaphysis provide additional purchase. The purpose of this study was to investigate if purchase of these screws can be enhanced further by injecting calcium sulfate and calcium phosphate composite graft into the drill holes prior to insertion of the screws. Materials and Methods: Bone density was quantified using a DEXA scan in paired cadaver legs. One leg from each pair was randomly selected for injection of composite graft into the screw holes before insertion of the screws. Two screws were inserted through the fibula into the distal tibial metaphysis in each leg, at the level of the syndesmosis under fluoroscopy in a standardized fashion in an MTS machine. Results: After testing 4 pairs of cadaver legs, a statistically significant difference was noted in displacement (p = 0.018 distal, p = 0.0093 proximal), failure load, (p = 0.0185 distal, p = 0.0238 proximal), and failure energy (p = 0.0071 distal, p = 0.0115 proximal) between augmented and non-augmented screws, with the augmented screws being considerably stronger. Conclusion: Screws augmented with composite graft provide significantly greater purchase in an osteoporotic fibular fracture model. Clinical relevance: Composite graft augmented screws inserted into the distal tibia from the fibula may enhance the stability of internal fixation of an osteoporotic ankle fracture. This may enable earlier weightbearing and return to function which is important in elderly patients.
INTRODUCTION
Globally, approximately 200 million people are at risk for sustaining an osteoporotic fracture each year. 8 By 2012, 25% of the European population will be over the age of 65 years, and by 2020, 52 million people will be over this age in the United States. 35 Lack of bone strength together with excessive skeletal loading and reduced control and coordination in elderly patients leads to a higher incidence of fractures that can require fixation to allow early mobilization despite osteoporotic bone. 30 Fractures in elderly patients' require treatment that quickly re-establishes function to avoid prolonged bedrest. 30 Accurate fracture reduction with secure fixation to allow early mobilization and weightbearing can be achieved only by surgical means. Frequently, it is difficult to accomplish this goal due to poor bone quality in elderly patients. 20,29,30,38
The major technical problem is obtaining secure fixation in osteoporotic bone. In fact, unsatisfactory results are seen in 42% of elderly patients with ankle fractures. 38 Eighty-four percent of patients with ankle fractures remained non-weightbearing for 6 to 8 weeks with an increased average length of hospital stay. 38 Strong fixation is achieved most reliably when the screws are placed in dense trabecular bone. In elderly patients with osteoporosis, there is less cortical and cancellous bone for the screws to gain purchase, so the screw-bone interface can be stripped easily during screw insertion. As a result, there is an increased risk of screw loosening and pull-out after surgery. 25 The holding power of screws is linearly correlated with bone mineral density. 5,31
Clinically, although delay in fracture healing is not always obvious, the decreased healing capacity in osteoporosis is reflected in a dramatic increase in the rate of implant failure. 2,12 The common mode of failure of internal fixation in osteoporotic bone is implant failure secondary to bone failure rather than implant breakage. 12 Nonunion and implant failure occur in 2% to 10% of fractures, malunion in 5% to 16%, and re-operation or early removal of implants in 1% to 16%. 4,20,1,19 Usually, the strength of screw purchase determines the ultimate strength of fixation. 30,40 Failure of fixation due to screws pulling out can occur even when tibia-pro-fibula screws are used (Figure 1).

Failure of fixation due to tibia-pro-fibular screws backing out.
A variety of methods and techniques have been used to reduce the rate of implant failure in osteoporotic bone. The use of tibia-pro-fibula screws to obtain better screw purchase into the tibial metaphysis in combination with a hook-plate has been described previously. 28,29 Another method is to use intramedullary Kirschner wires with a fibular plate which is augmented by proximal fixation of the fibula to the tibia with screws above the fracture. 9 A variety of substances also have been used to enhance the screw purchase in bone including bone autograft or allograft, bone cement, or bone substitutes such as calcium sulphate. 6,10,14,18,23,24,26,32,33,41,43 The major advantages of the calcium sulphate/calcium phosphate composite graft are that it is osteoconductive, resorbs during fracture healing, and has the ability to remodel into bone. Furthermore, it is injectable and has demonstrated bone regenerative properties. 22,44 When compared with conventional calcium sulfate pellets, triphasic calcium sulfate cement produces an increased amount and strength of restored bone. 22,44
The purpose of this study was to investigate whether purchase of tibia-pro-fibula screws in the distal tibial metaphysis can be enhanced by injecting this composite graft into the drill holes prior to insertion of the screws.
MATERIALS AND METHODS
Specimens and Fixation
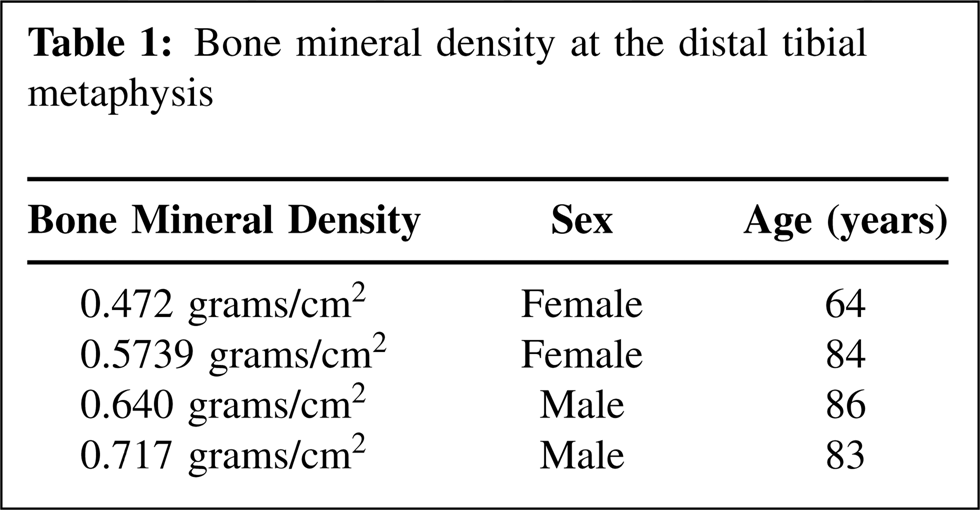
Four fresh frozen pairs of elderly cadaver legs free of disease or deformity were obtained and stored at a constant temperature of −10 degrees Celsius. The cadaver legs were thawed for 24 hours until they reached a core temperature of 21 degrees Celsius. The core temperature of each bone was checked in the drill holes made for placement of the screws. Bone mineral density (BMD) was determined for all specimens using Dual Energy X—Ray Absorptiometry (DEXA) scan (Hologic Discovery, MA; model QDR 4500). The actual BMD values were provided as no standard Z scores are available for the distal tibial metaphysis. Three cadavers were above 80 years old and one cadaver was from a 64-year-old but had the lowest BMD value (Table 1).
Bone mineral density at the distal tibial metaphysis
The lateral malleolus was exposed through a 4 cm incision over the distal fibula. Each leg was secured in a customized gutter shaped jig made of a radiolucent material. This jig had holes to direct the drill bit in an identical direction and location in both legs of a pair. A 3.5-mm drill was used to make the holes across both cortices of the fibula and the tibia; the hole in medial cortex of the tibia serving to relieve pressure and ease flow of composite graft. The holes were made 1.5 cm apart in a coronal plane, with the distal hole located 1.5 cm above the joint line.
One specimen from each pair of cadaver legs was randomly assigned to serve as a control. In the legs assigned to the study group, the composite graft [calcium sulfate and calcium phosphate (PRO-DENSE™ Wright Medical Technology Inc, Arlington, TN] was injected into the drill holes. The composite graft was prepared according to the manufacturer's instructions. The paste was loaded into the syringe with a spatula and 2 to 3 cc was injected into the drill holes across the fibula and tibia. Fully threaded 4.0-mm diameter cancellous screws (Synthes, West Chester, PA) were inserted in the holes made in the distal tibial metaphysic, engaging three cortices in both the study and control groups. The screws were inserted immediately after injection of the composite graft in the study group. After 30 minutes, the legs were stored in a cool room at 2 degrees Celsius for 12 hours. Before testing, the specimens were left at room temperature until they reached 20 degrees Celsius.
Mechanical Testing
The cadaver legs were positioned under a plate secured to the load cell of a 858 Mini Bionix test machine (MTS Corporation, Minneapolis, MN). A base plate with a 3×3-cm hole through which the screw head could be clamped and adjusted in three dimensions was used to assure that the axial force was directly in line with the vertical axis of the screw. The screw head was secured with a clamp connected to a universal joint on the machine actuator, which again allowed for three-dimensional adjustments (Figure 2). The screw was subjected to constant displacement of 0.2 mm/sec until complete dissociation from the bone. The distal screw was tested first, followed by the proximal screw.
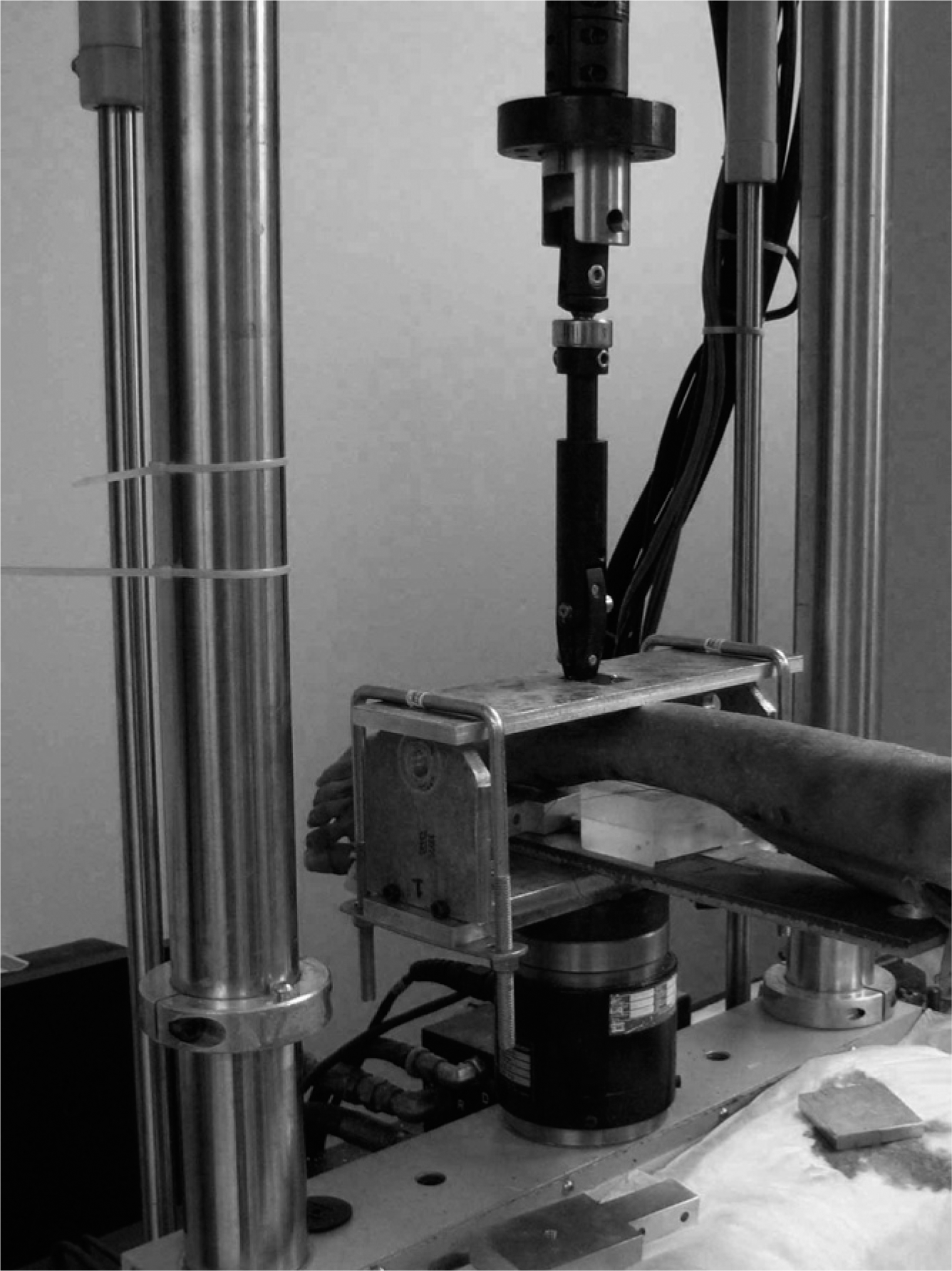
Test setup for screw pull-out in cadaver ankle specimens.
Force and displacement values were recorded and used to generate load versus displacement curves (Figure 3). Stiffness, failure displacement, failure force, and failure energy were calculated and compared for differences between the augmented and non-augmented groups. The null-hypothesis was that the augmented screws would have better purchase and therefore better resistance against the pull out force.
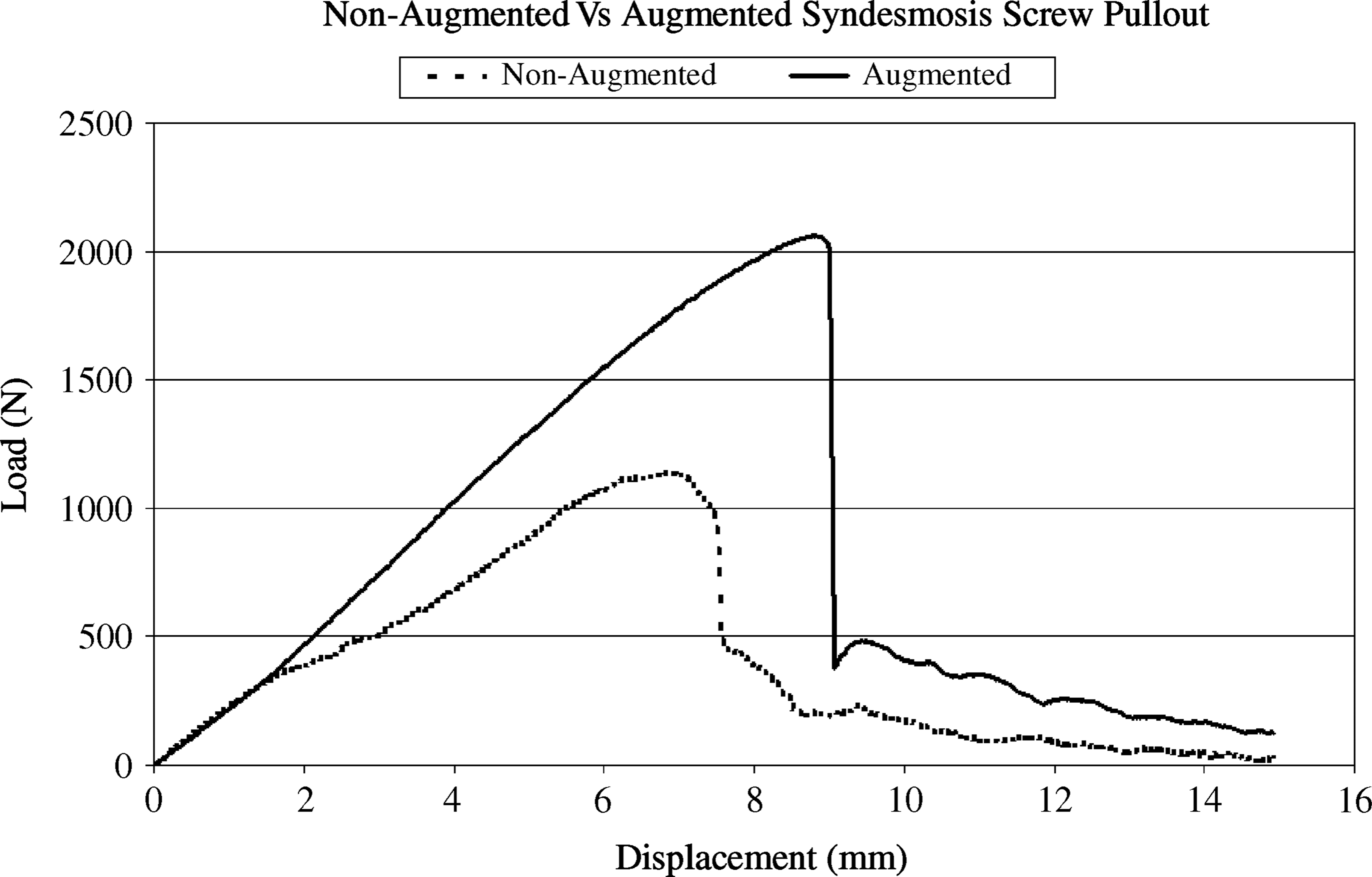
Typical load versus displacement curves for the screw pull-out tests, showing the augmented (solid line) and the non-augmented (dotted line) conditions of the same specimen.
Statistical analysis was performed on the data using PC-SAS (SAS Institute, Cary, NC). A two-way ANOVA using the Proc GLM (General Linear Model) in PC-SAS was used to test for differences in outcome measures due to calcium sulfate, and position. Unless stated otherwise a p value of less than 0.05 was considered to be statistically significant.
RESULTS
Bone mineral density of the distal tibial metaphysis, sex, and age of the four specimens tested are listed in (Table 1). Out of the 16 screws inserted, one proximal screw in the augmented group was inserted incorrectly. For both the distal and proximal screws, significant differences were found between the non-augmented and composite graft augmented fixation. The augmented screws had significantly higher displacement before failure (p = 0.018 distal, p = 0.0093 proximal), significantly higher failure force (p = 0.0185 distal, p = 0.0238 proximal), and significantly higher energy absorbed at failure (p = 0.0071 distal, p = 0.0115 proximal). There was no significant difference found in stiffness, but the augmented group was consistently higher. The distal screws appeared to be stronger than the proximally placed screws. Fluoroscopic examination after the screws were pulled out revealed fibular fracture (Figure 4) only in the specimens that had screws augmented with the composite graft. Figures 5 to 8 show the proximal and distal screws as augmented versus non-augmented groups for stiffness, displacement, failure force, and energy.
X-ray of non-augmented (left) and augmented (right) distal tibia and fibula after screw pull out.
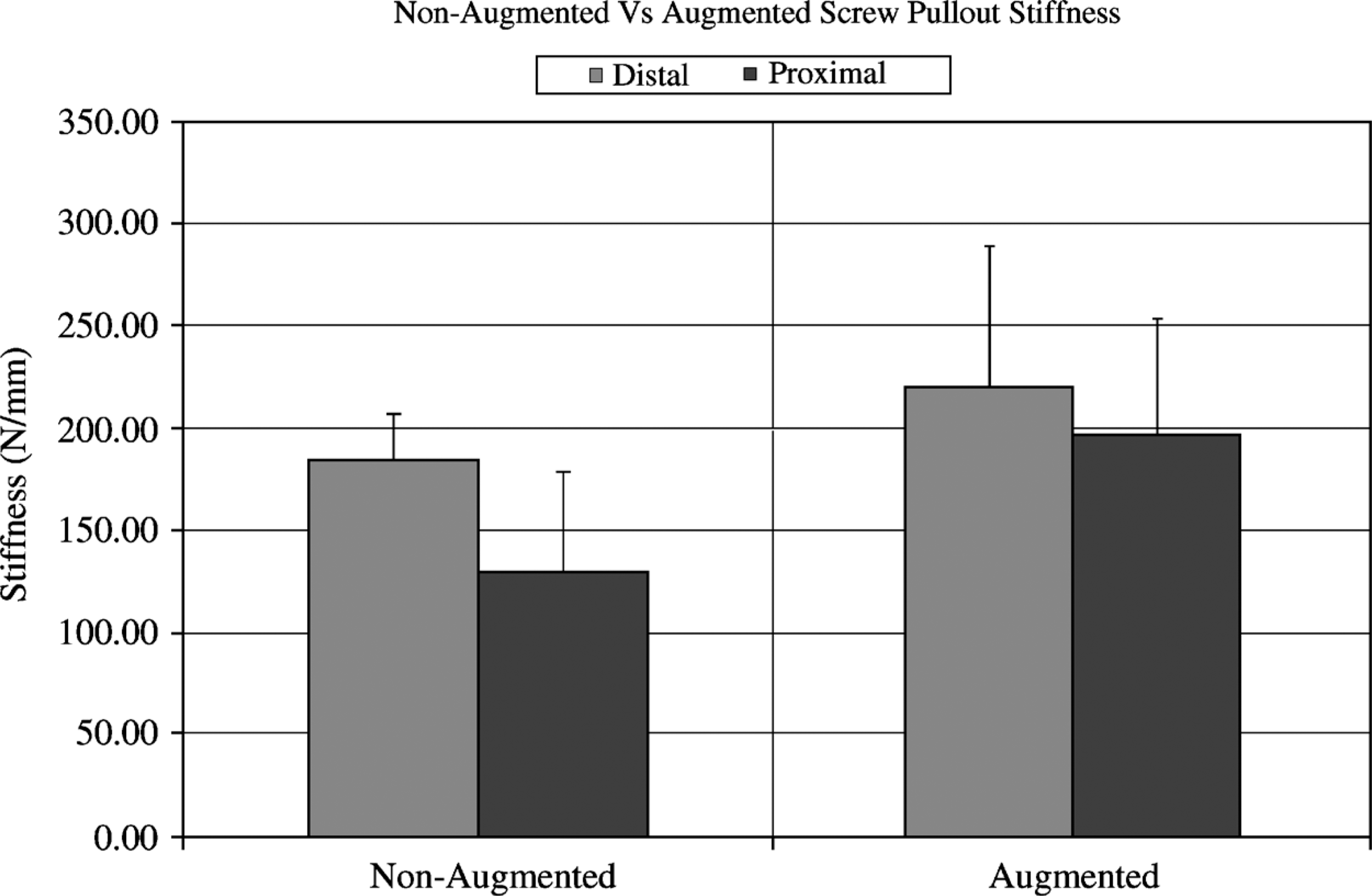
Screw pull-out stiffness of augmented versus non-augmented specimens for proximal and distal screws.
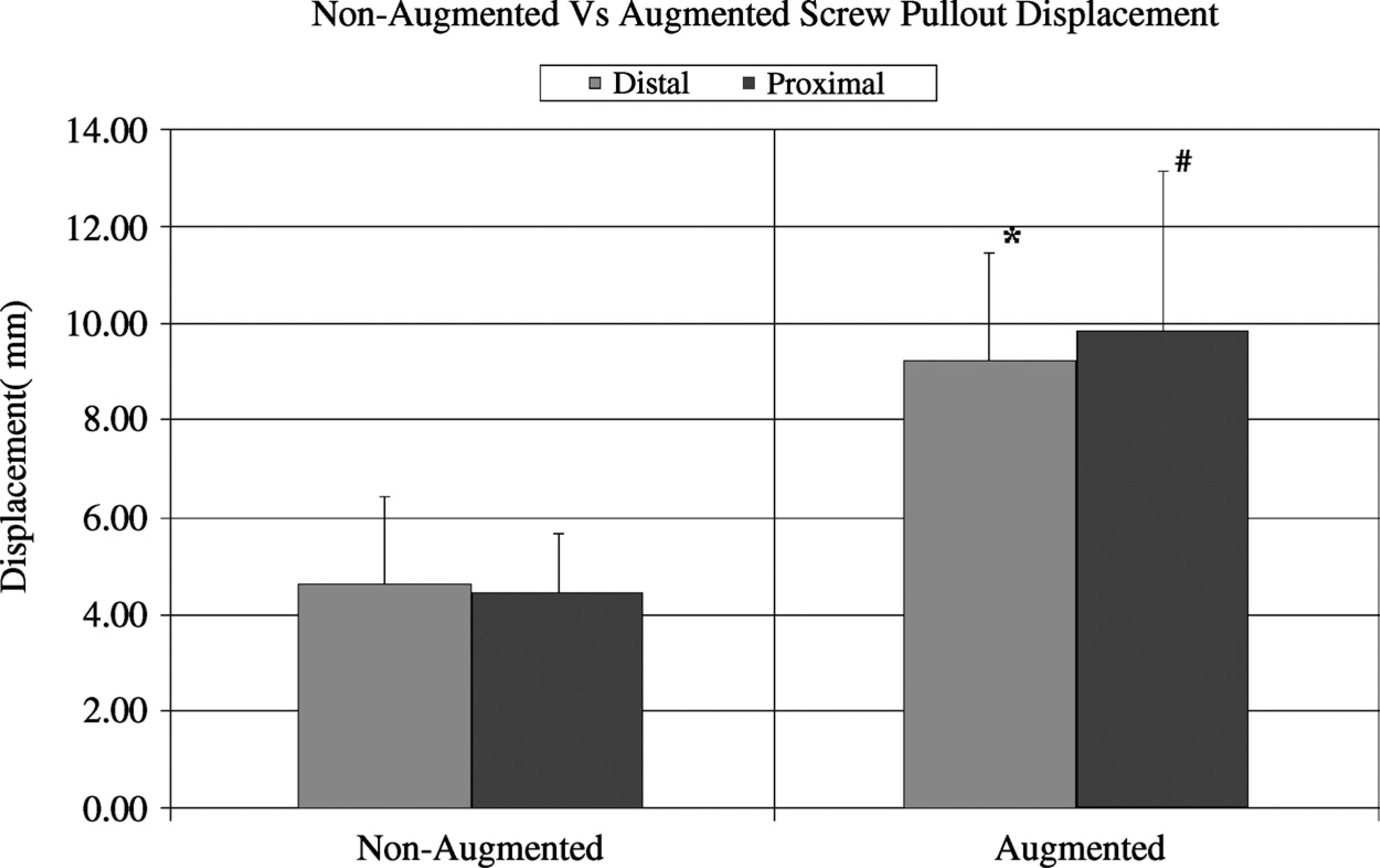
Screw pull-out displacement of augmented versus non-augmented specimens for proximal and distal screws.
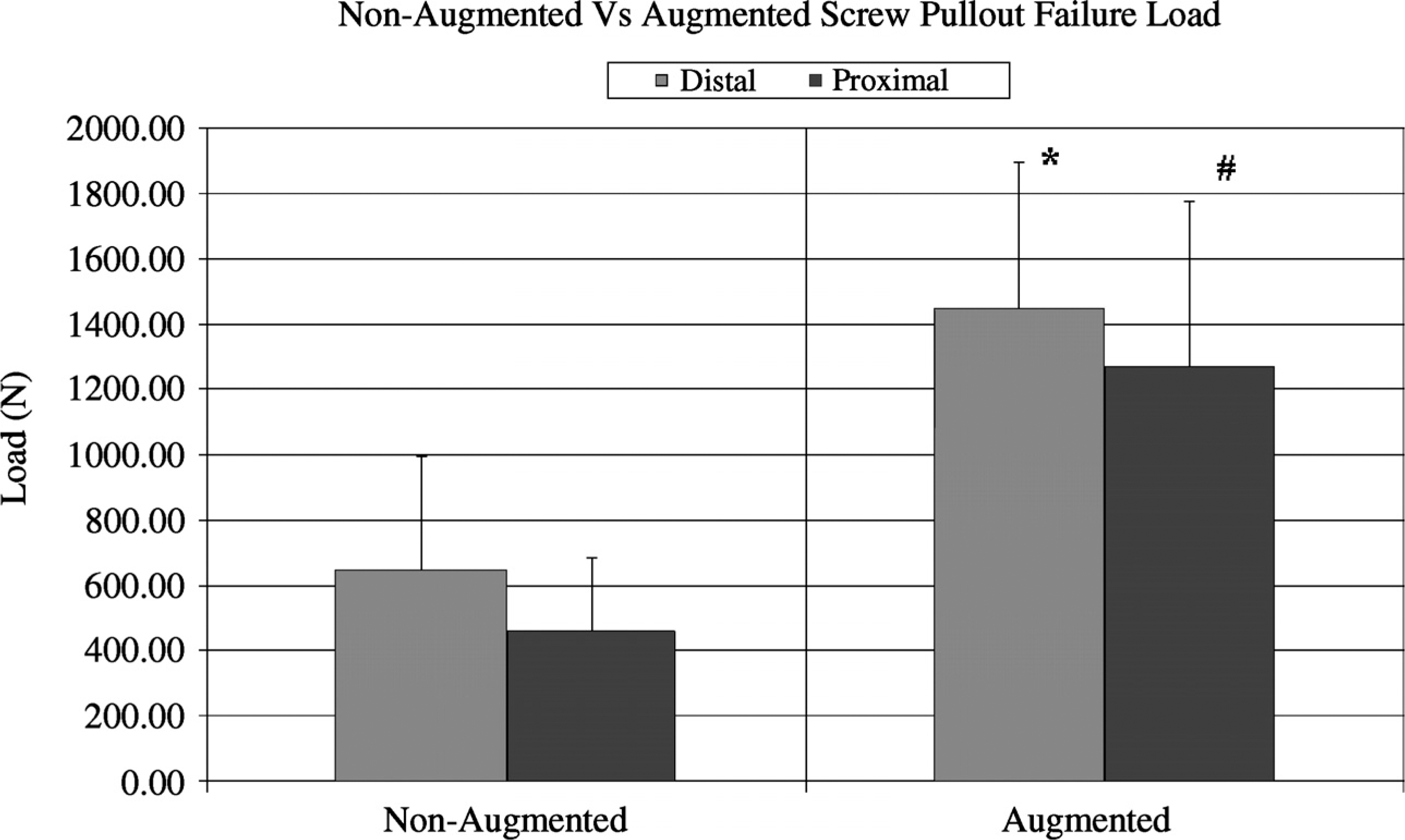
Screw pull-out failure load of augmented versus non-augmented specimens for proximal and distal screws.
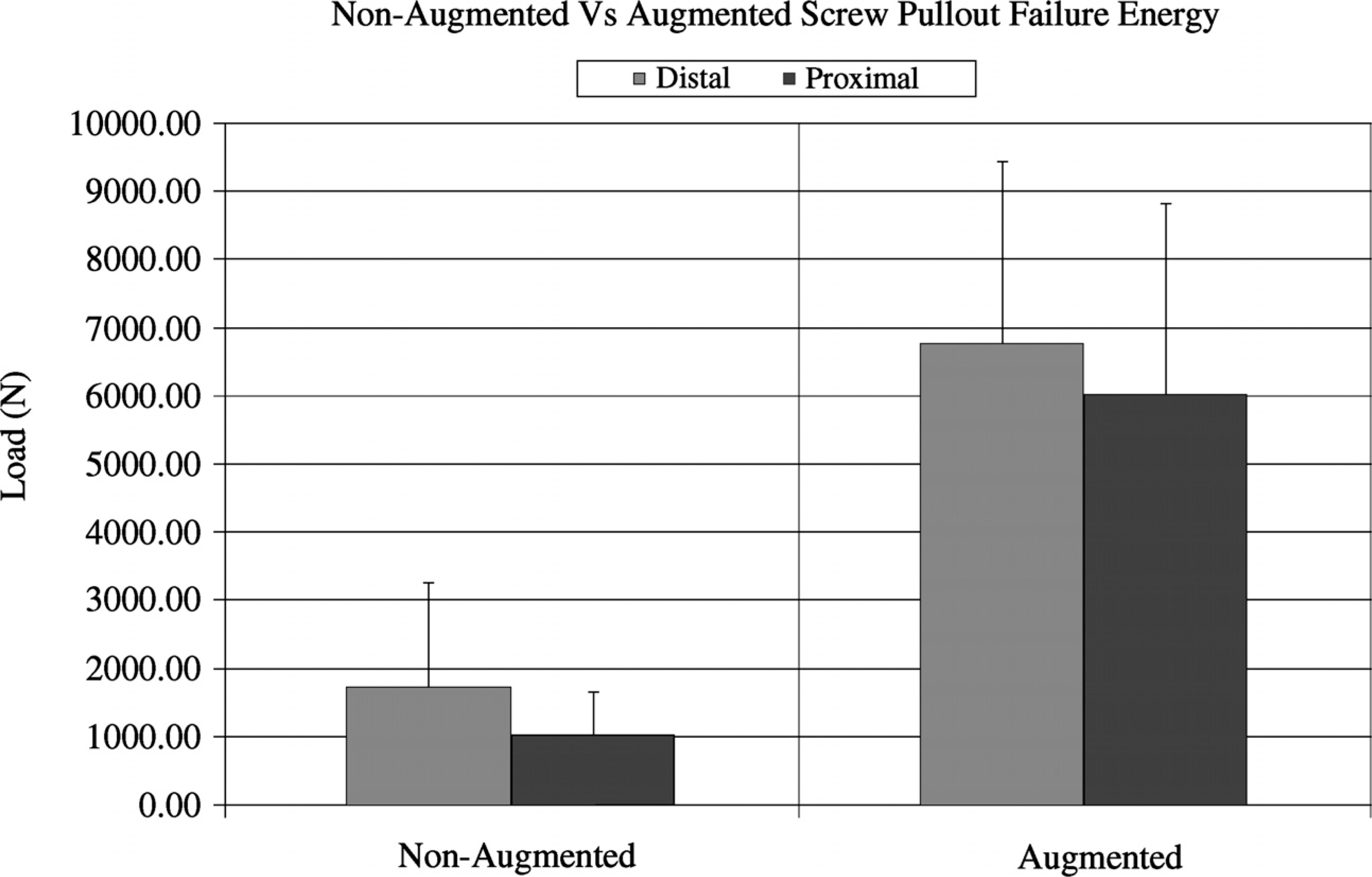
Screw pull-out failure energy of augmented versus non-augmented specimens for proximal and distal screws.
DISCUSSION
The force and energy necessary to pull out the composite graft augmented screws was 240% and 450%, respectively, greater than the force and energy necessary to pull out the non-augmented screws. The augmented screws displaced 200% more before they failed when compared with non-augmented screws. ANOVA was used instead of a Student's t-test to analyze the results because there were unequal numbers to compare as one screw which was placed incorrectly was excluded. Statistically significant differences were noted after testing just 4 pairs of specimens, therefore the study was stopped.
The distal subchondral screws, when compared to the proximal one, required more displacement, higher force and energy to fail whether augmented with composite graft or not. Augmentation had little effect on pull-out stiffness, which was consistent with previous studies. 7 The change in stiffness after augmentation was linearly correlated with the BMD of the bone (Figure 9). Interestingly, the failure energy did not correlate with the BMD in non-augmented screws. We assume that the injectable composite graft did not produce a cement mantle because stiffness did not change statistically; instead, it filled in the trabecular spaces and produced a stronger combined bone cement interface, which provided better purchase of the screw. 27 The holding power of the combined composite graft and bone interface may be dependent on BMD [bone quality] because the energy to pull out augmented screws was trending higher as BMD increased.
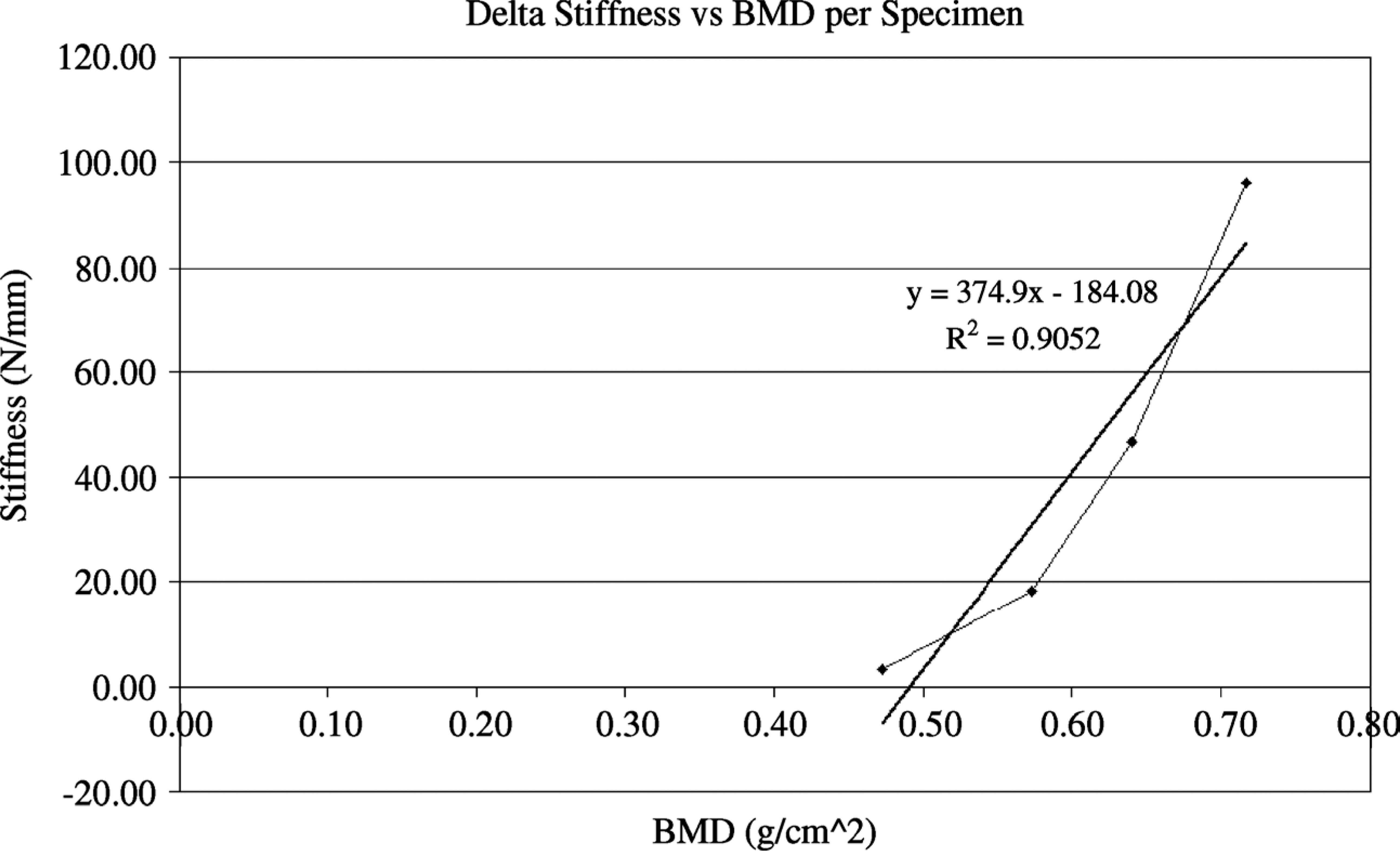
Correlation between change in Stiffness after augmentation and BMD.
Fibular fracture occurred in augmented specimens at the proximal screw site (Figure 3). The significance of this finding could be that the pull out resistance of augmented screws is equal or higher than the strength of the osteoporotic fibula. The fibular fracture also could be due to the stress reactions from the mounting plate used in the experimental set up.
In non-augmented screws, failure occurred through simple stripping of the bone at the bone-screw interface. In the augmented group, we assume failure often occurred through stripping of the screw-cement bone interface, as the augmented screws were clean when pulled out and had very little or no augmented substance attached to them. None of the augmented screws produced a larger defect than the non-augmented screws when checked under fluoroscopy after failure (Figure 3). Failure of an augmented screw at the screw-cement bone interface would not create a large bony defect that complicates revision, unlike a failure occurring at the cement-bone interface with PMMA. 34
Polymethylmethacrylate (PMMA) injection into the screw hole before pedicle screw insertion has been recommended as a means of augmenting the screw bone interface in older, osteoporotic patients as it dramatically improves axial pull-out resistance and the resistance to screw toggle caused by cyclic caudocephalic loading. 16,17,36,39,49,51 However, it is not commonly used clinically because of intraoperative and long term problems, including the risk of neural injury, risk of thermal necrosis during polymerization, cement extrusion into the fracture site and joint, 3,15 the toxicity of the polymerization reaction of PMMA 42 and complications of revision surgery and hardware removal. 16,45,48 Furthermore, PMMA can physically block endosteal and periosteal new bone formation during fracture healing, 50 and PMMA evokes the formation of a fibrous membrane at the bone cement interface, which produces a number of cytokines and inflammatory mediators that lead to bone resorption, 46,47,13 which is also caused by particulate PMMA wear debris. 21 Finally, retained PMMA can act as a stress riser, 11 which increases the risk of refracture.
Composite graft may be a better alternative to PMMA. It can be injected or packed into irregular bony defects as a paste and it hardens rapidly; it solidifies in minutes, and sets in 25 minutes. It is not associated with exothermic necrosis of adjacent tissues. Most importantly, composite graft is biocompatible, bioresorbable, and osteoconductive, so it has the potential for replacement by new bone during healing and normal bone turn over. Composite graft is resorbed in 180 days. Resorption of conventional calcium sulfate pellets was apparent at 2 weeks and completely absorbed in 6 weeks. 22,44 This early absorption of the augmented cement may weaken the screw purchase before complete fracture healing. The calcium sulfate in the composite graft resorbs early but the calcium phosphate takes 180 days for complete resorbtion. The rapid onset but slow rate of absorption promotes bone formation deep into the bolus of cement while a portion of calcium phosphate continues to provide a scaffold which eventually is incorporated into new bone. 22,44
Studies have shown that PMMA provides superior holding strength to calcium phosphate. 6,10,14,18,23,32,41,43 A study on augmentation of lumbar pedicle screws showed no significant difference in the pull-out strength between screws augmented with calcium sulfate and PMMA (p = 0.0791). 34 Spivak et al. performed an animal study evaluating a hydroxyapatite / calcium sulfate mixture and found increased strength at six weeks time. 37 The author determined that the increased pull-out strength was the result of bony in-growth into the paste mixture.
Monotonic testing of only one mode of failure is a limitation in this current cadaver study as there may be other modes by which failure of fixation can occur. Further biomechanical and clinical evaluation is necessary to determine if augmentation of screw purchase using calcium sulfate can increase the strength of internal fixation in an osteoporotic ankle fracture enough to allow the elderly patients full weightbearing on the injured extremity without risking failure of fixation.
Failure of a plate and screw construct following internal fixation of an osteoporotic ankle fracture occurs due to screws backing out. Improving screw purchase hopefully will prevent this method of failure. The aim of this study was narrowly defined to address this issue and was limited to testing screw purchase in the distal tibial and fibular metaphysis. The specimens therefore were loaded onto the MTS machine in a way that would allow the most direct method to test their resistance against being pulled out.
There are no previous studies to the authors' knowledge that determine if injectable composite graft can augment screw purchase in osteoporotic long bone metaphysis, particularly in the distal tibia. The current study shows that composite graft augmented screws are significantly stronger in one-time axial pull-out testing than non-augmented screws in osteoporotic distal tibial and fibular metaphyseal bone.