
Abstract
Background:
Chronic exertional compartment syndrome of the foot has been previously described. There has been debate over the exact number and location of compartments. The involvement of the medial compartment has been consistently described in case reports; however, there is little in the orthopaedic literature on the exact anatomy for the fasciotomy and the resultant long term outcomes.
Materials and Methods:
We present the results of five patients (seven feet) who were surgically treated by medial compartment decompression, releasing both superficial and deep fascial layers. There were three females and two males, average age of 23 (17 to 34) years. Decompression was bilateral in one, sequential in one, and unilateral in three. Three patients also had surgical treatment of chronic compartment syndrome elsewhere in their lower limbs.
Results:
Preoperative post exertional compartment pressure measurements were 67.8 (32 to 114) mm at 1 minute and 50.2 (28 to 97) mm at 5 minutes. At an average of 21 (9 to 57) month followup, all but one patient had significant relief of their symptoms.
Conclusion:
Chronic exertional compartment syndrome may affect multiple compartments in the lower limb of a single patient. When affecting the medial compartment of the foot, release of the superficial and deep fascia is a reliable treatment. It is safe to perform bilaterally and in association with other lower limb decompressions as required.
INTRODUCTION
Chronic compartment syndrome is well-recognized, having been first described in 1912 by Wilson in the Antarctic and then again as “march gangrene” by Vogt in 1943, 2 although the first reported fasciotomy was in 1956. 9 It is usually described following exertion, but has been described following a period of dependence during surgery. 19
Chronic exertional compartment syndrome is most commonly described in the compartments of the lower leg, 2,3,6,9,17 but it has also been reported in the upper limb 15 and, less commonly, in the foot. 1,7,10,11,13,18 While there has been debate regarding the exact number and locations of the compartments in the foot, 5,8 all reported cases have involved the medial compartment.
To our knowledge, there are only seven case reports of chronic exertional compartment syndrome of the foot with only short followup. 1,7,10,11,13,18 The description of the decompression of the medial compartment in chronic compartment syndrome in these cases is variable and the resultant longer-term outcome not known. Timing of decompressions when presentation is bilateral has not been described. We present a series of successful decompressions of the medial compartment through two small skin incisions over the proximal and distal end of the affected compartment.
MATERIALS AND METHODS
In our establishment over a 4-year period we surgically treated seven feet in five patients with chronic exertional compartment syndrome of the medial compartment of the foot following the exhaustion of conservative treatment. A complete history was taken of the nature and onset of symptoms.
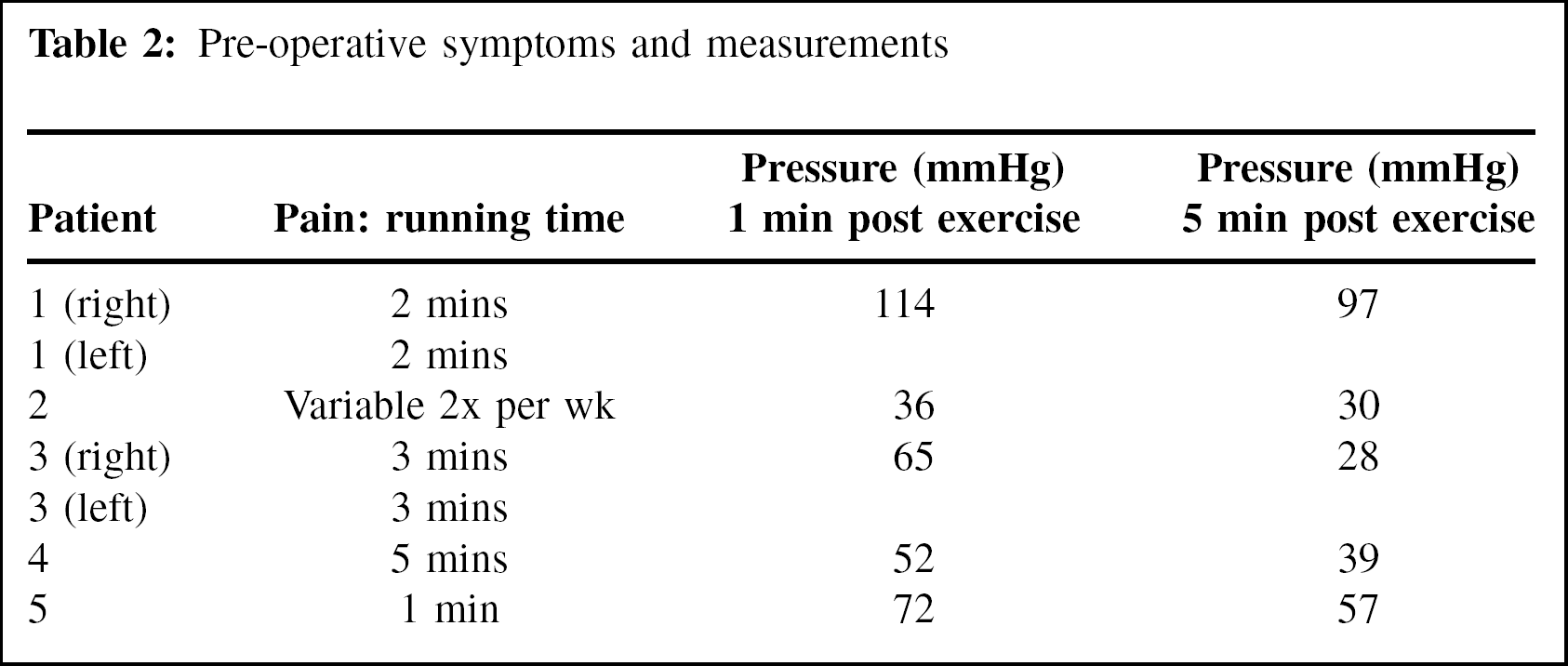
Due to the patients' presenting symptoms, pressures were measured in the medial compartment of the foot only, using the Stryker pressure monitor (Stryker, MI). Patients exercised at our sports medicine facility until they developed pain. The times to develop pain are summarized in Table 2. Measurements were taken at 1 and 5 minutes post-exercise as suggested by Pedowitz et al. 14 This group has clearly defined measurement criteria to be used in the lower leg to confirm the diagnosis of chronic exertional compartment syndrome. They suggested pressures of greater than 30mmHg at 1 minute and greater than 20mmHg at 5 minutes post-exercise as diagnostic. This has been supported by Mollica 12 with reference to the foot.
Measurements were not repeated in bilateral cases when the diagnosis was confirmed on the first side, as the symptoms and clinical findings on the contralateral side were identical in these cases.
The patients all underwent identical surgical release. Two oblique incisions were made over the abductor hallucis muscle, one proximally and one distally (Figure 1). The superficial fascia overlying the muscle was divided longitudinally and the muscle then separated in line with the fibers to allow access to the deep fascia which was divided in a similar fashion. The distal end of the tarsal tunnel was then released as was the superficial aspect of the described central compartment.

Surgical incisions for fasciotomy.
Clinical followup was until an optimal result achieved. Further clinical review was performed for the purpose of the study in all but one patient, who had a review about the same time because of return of symptoms. Patients were questioned as to when, if at all, any of their preoperative pain occurred.
RESULTS
Three females and two males made up the study group. The average age was 23 (17 to 34) years old. All patients were either keen sportswomen/men or involved in military training (Table 1). The classical symptoms described were of tightness developing on the medial side of the foot associated with a burning, throbbing pain with exercise; they also noted swelling in the affected region. The pain eased with rest. One patient (2) also developed pain at other times, not necessarily associated with exercise, while patient 1 had some of the classical symptoms and others that were more difficult to assign to any specific pathology.
Patients and compartments involved
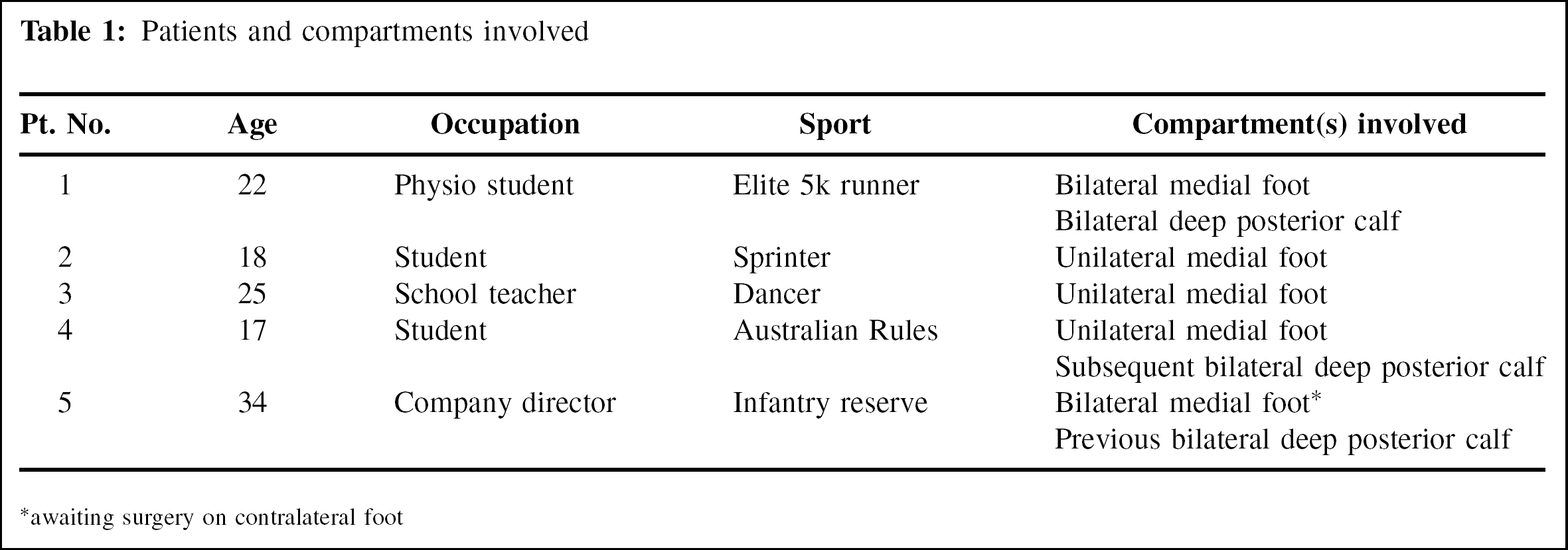
awaiting surgery on contralateral foot
In all cases where the pressure studies were performed, the pressures were in excess of the values recommended by Pedowitz et al. 14 for both 1 and 5 minutes post-exercise (i.e., greater than 30mmHg and greater than 20mmHg). The average pressure at 1 minute was 67.8 (36 to 114) mm and at 5 minutes was 50.2 (30 to 97) mm (Table 2).
Pre-operative symptoms and measurements
In one case, the second side was decompressed 8 months later. One patient had bilateral posterior compartment of the lower leg decompressions as well as medial foot fasciotomies in one sitting. One patient underwent a simultaneous calcaneal osteotomy for a planovalgus foot. This latter patient has chronic exertional compartment syndrome in the contralateral foot and is awaiting decompression.
One patient presented with a history of previous compartment release for chronic compartment syndrome in the lower leg, while another required subsequent release of his deep posterior compartment of the leg due to chronic exertional compartment syndrome.
Most recent followup was, on average, 21.4 (9 to 57) months. All but one patient had significant relief of their preoperative symptoms, with 57% (4 of 7) having complete resolution. One patient (2) who had more varied onset of symptoms had persistence of more mild persistent symptoms following surgery occurring with significantly less frequency (Table 3). One patient (1) (two feet) has persistent/recurrent symptoms, having reported being able to run for an hour and a half at 3.5 months with 20 minutes of walking now being her limit. It is not clear that her symptoms were all related to chronic exertional compartment syndrome. This patient's preoperative pressures were extremely high (114mmHg at 1 minute and 97 at 5 minutes post-exercise).
Post operative symptoms at most recent followup
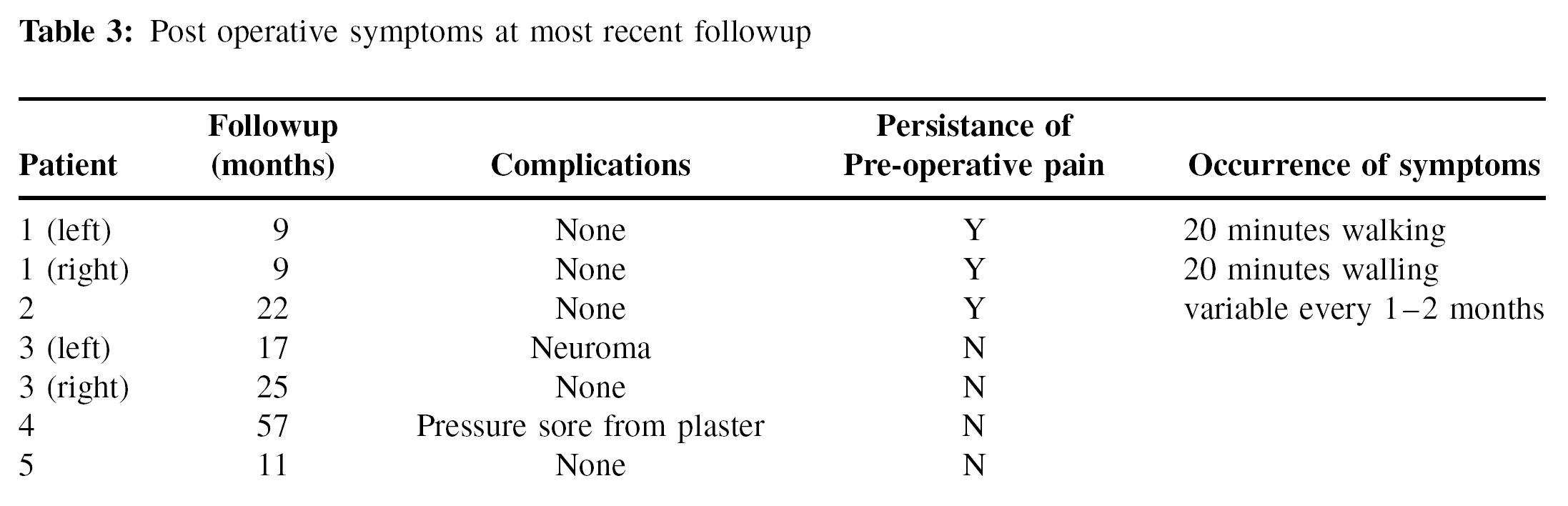
There were two postoperative complications; one was a pressure sore as a result of the plaster, which resolved with debridement alone. Patient 3 had numbness in the region of the medial plantar nerve for 6 months postoperatively and now has symptoms and signs consistent with a small neuroma of the medial plantar nerve under the proximal incision. This causes the patient few symptoms (rating it as 2/10), which is only bothersome when wearing shoes with a strap around the back of the ankle.
DISCUSSION
Compartment syndrome is defined as increased pressure within a fibro-osseous space leading to a reduced blood flow and tissue perfusion leading to ischemic-type pain. 3 Its occurrence following exercise is thought to be related to the fact that during strenuous exercise muscle fibers can swell up to 20 times their resting size and lead to a 20% increase in muscle volume. 4 The exact reason that this leads to the chronic exertional compartment syndrome in some people is unknown, but has been hypothesized to be due to abnormal arteriolar regulation as well as limited osseofascial expansion. 3
Pedowitz et al. 14 have clearly defined measurement criteria to be used in the lower leg to confirm the diagnosis of chronic exertional compartment syndrome. The post exercise pressures were shown by Mollica 12 to be applicable in the foot in his group of nine patients, however he did not find elevated resting pressures in most cases. This latter study only assessed the patients prior to any surgical intervention.
Surgical release of both the superficial and deep fascia was performed, as we feel that division of the relatively flimsy superficial fascia would be inadequate. Our theory was supported when we successfully treated a patient who had previously had surgical release at another location of just the superficial fascia without resolution of their symptoms. In our series, we appreciate that some symptoms may have been emanating from the calcaneal compartment (suggested to be involved in some reports 7,10 ). Measurement of the pressures in this region has been shown to be difficult, however, without an anesthetized patient and complex imaging modalities. 5 This release needs to be performed with care and understanding of the underlying anatomy. The use of two small oblique incisions was felt to reduce any subsequent scar irritation due to shoewear.
In our group of patients, the condition affected both feet in three of the five patients and the deep posterior compartment of the leg also in three. This would concur with the published literature that it is a condition that does not just affect an isolated muscle group. Two of the case reports of affected feet had bilateral 7,10 involvement and reports of the condition in the calf suggest it to occur bilaterally in about 70% cases. 16
Persistent symptoms following deep posterior compartment release is said to be around 55%. The long term relief of foot symptoms following release of the medial compartment of the foot would appear to be better than this; our study, although only having small numbers, revealed persistent symptoms in only 43%. The results appear to be less consistent when symptoms are not absolutely classical or when the pressures are extremely high.
In summary chronic exercise induced compartment syndrome in the medial compartment of the foot is not common, but its prevalence does appear greater in those patients who have the condition elsewhere in their lower limb. Releasing the superficial and deep fascia is an effective way of treating the condition, and can be performed on both feet at the same time.