
Abstract
Background: The effect of the Cotton osteotomy has not been studied in isolation, and no alternative to bone graft has been investigated for this osteotomy. We hypothesized that there would be no difference in radiographic and pressure findings using the Cotton osteotomy with bone graft or an opening wedge block plate. Materials and Methods: Each specimen of eight matched pairs of lower extremities was loaded in simulated double-leg stance via pneumatic cylinders as described previously. Weightbearing lateral and anteroposterior radiographs and medial and lateral pressure measurements were obtained for all intact specimens. Specimens were randomly assigned to receive a Cotton osteotomy with a dorsal opening wedge allograft or an opening wedge plate. Each specimen was cycled at 3 Hz to 720 N for 5000 cycles and measurements were repeated. Results: Calcaneal pitch was lower after the block plate procedure (mean ± standard error of the mean) (intact, 23.4 ± 1.2 degrees versus post-procedure, 21.8 ± 1.1 degrees; p = 0.05). There was a significant difference (p < 0.05) in percentage of total plantar pressure medially and laterally between the intact specimen and the specimen after osteotomy with both methods. Pressure increased medially and decreased laterally. Conclusion: With the numbers available, these methods for performing a Cotton osteotomy did not differ in addressing lateral column overload. Clinical Relevance: Dorsal opening wedge medial cuneiform osteotomy performed with femoral head allograft or a block plate may be effective both in reducing lateral column pressures and increasing medial column pressures when they are deficient preoperatively.
INTRODUCTION
The dorsal opening wedge (Cotton) osteotomy of the medial cuneiform is used in the treatment of adult flatfoot to theoretically correct forefoot varus deformity. In 1936 Cotton described a dorsal opening wedge osteotomy of the medial cuneiform to correct a dorsiflexed medial column. 2 The osteotomy has been used in the surgical management of pediatric and adult flatfoot deformities, often in conjunction with other procedures. 6 Hirose and Johnson 3 reported good results using the Cotton osteotomy to correct flatfoot deformities in conjunction with multiple other procedures including medial displacement calcaneal osteotomies and flexor digitorum longus transfers. Viehweger et al. 9 performed a biplanar dorsomedial opening wedge osteotomy of the medial cuneiform in 31 pediatric feet to treat metatarsus adductus and varus. At 5 years followup, the authors noted improvements of the talonavicular and calcaneal pitch angles. Benthien et al. isolated the effect of the osteotomy in a flatfoot model, showing improved radiographic parameters and normalization of forefoot pressure with the Cotton osteotomy after lateral column lengthening. 1 The procedure contributes to improved balancing of the forefoot, but the effect of the osteotomy has not been isolated in these clinical studies.
Further, it would be useful to have an alternative for this procedure when use of bone graft is not desirable. The reported method for performing the Cotton osteotomy involves autograft harvested from the iliac crest, which provides secure fixation, reliable healing, precise correction, and usually the absence of supplemental fixation. 3,4 Allograft may also be used without adverse effect on operative results, 3 with the benefit of avoiding potential complications of the additional operative procedure to harvest the graft. In a common allograft method reported anecdotally, a corticocancellous allograft wedge from the calcar region of a femoral head and neck is used. However, allograft is not always available. One possible alternative method to using bone graft involves use of a low-profile small bone plate and screw system. The plate is applied dorsally on the medial cuneiform with a metallic opening wedge spacer directed plantarly to hold the osteotomy secure. The spacer maintains the opening wedge by cortical contact and allows for cancellous bone grafting into the gap to facilitate bony union.
We hypothesized that the results of dorsal opening wedge medial cuneiform osteotomy with the opening wedge block plate would not differ from results with bone graft with regard to radiographic correction of deformity and medial and lateral forefoot pressure change. To investigate the effects of the Cotton osteotomy, we evaluated radiographic and pressure changes after performing the osteotomy on normal cadaveric feet.
MATERIALS AND METHODS
Eight matched pairs of fresh or fresh-frozen cadaver lower extremities were used in the study. The average age was 71 years (range, 49 to 85 years), with four male and four female donors. The specimens were chosen after gross visual inspection for pre-existing abnormalities of the foot. Frozen specimens were thawed to room temperature before each experiment. The tibia and fibula were amputated 30 cm proximal to the plantar skin. The proximal 10 cm of skin and subcutaneous tissue was removed and the tendons of the posterior and lateral compartments were dissected free and secured with suture using a Roman sandal technique. The specimens were then secured to an MTS machine (MTS Systems Corporation, Eden Prairie, MN). The sutures were strung through proximal pulleys and connected to pneumatic cylinders using wire cables.
Each specimen was then examined in simulated double-leg stance just prior to heel rise as described previously 10 with axial compression of 720 N and simulated muscle forces. Specifically, the muscle forces were Achilles, 400 N; posterior tibial tendon, 40 N; flexor digitorum longus, 20 N; flexor hallucis longus 20 N; peroneus longus tendon 40 N; and peroneus brevis tendon 40 N. 10
Baseline measurements were then taken in each intact foot. Each specimen had weightbearing lateral and anterior-posterior radiographs of the foot with the muscle forces in effect. The indices measured on anterior-posterior radiographs included the talar-first metatarsal angle, talar head uncovered percentage, and the talar head-navicular angles. On lateral radiographs, talar-first metatarsal angle, calcaneal pitch, and medial cuneiform height were measured. Plantar pressure measurements were obtained using the F-scan computerized gait analysis system (Tekscan, Inc., South Boston, MA) as described previously. 10
A Kirschner wire was placed in the medial cuneiform along the expected plane of the cut. Fluoroscopy was used to determine the correct location and orientation of the osteotomy roughly parallel to the first metatarsocuneiform joint and equally distant from the proximal and distal cuneiform cortices.
Specimens in each pair were randomly assigned to receive either femoral head or block plate fixation. For femoral head allograft fixation, the heads were harvested and dissected free of all soft tissue and a wedge was fashioned using a microsagittal saw. A bicortical wedge was fashioned from the calcar portion of the femoral neck. The depth of the wedge was 18 to 20 mm. Dorsally the width was approximately 12 mm and the length was 7 mm, resulting in a 7-mm dorsal opening wedge. The 7-mm size was chosen because it is the size used most commonly in our clinical experience. The osteotomy was held open, and the allograft wedge was placed using a bone tamp and a mallet. The graft position was maintained through friction and soft tissue tension with no additional methods such as pins or screws used to secure the graft.
The same Cotton osteotomy technique was done on the opening wedge plating group. The osteotomy was secured with a low-profile small bone opening wedge plate (Arthrex, Inc., Naples FL). This titanium plate was developed for use in securing opening wedge osteotomies in the small bones of the hand and foot. It is secured with four fully threaded, self-tapping 2.3-mm cortical screws. Two are placed proximal and two distal to the block. The length of the plate's wedge block in this study was 5 mm, which was the largest available at the time. This corresponded to a 5-mm dorsal opening wedge.
Following completion of the osteotomy, each specimen was secured in an MTS load frame (MTS Systems Corp., Eden Plains, MN) and cycled at a frequency of 3 Hz up to 720 N for a total of 5000 cycles. This loading simulated full weightbearing on the fixation construct with cyclic loading to represent initial steps. After completion of loading, we observed the osteotomy site for signs of graft fragmentation or dislodgment or plate or screw failure. We then repeated weightbearing radiographs and plantar pressure measurements.
A paired t-test was used to determine whether any significant changes occurred in radiographic and pedobarographic parameters after the osteotomy and between osteotomies (p ≤ 0.05).
RESULTS
No signs of graft fragmentation or dislodgment or hardware failure were observed, and no cases of osteotomy narrowing were seen.
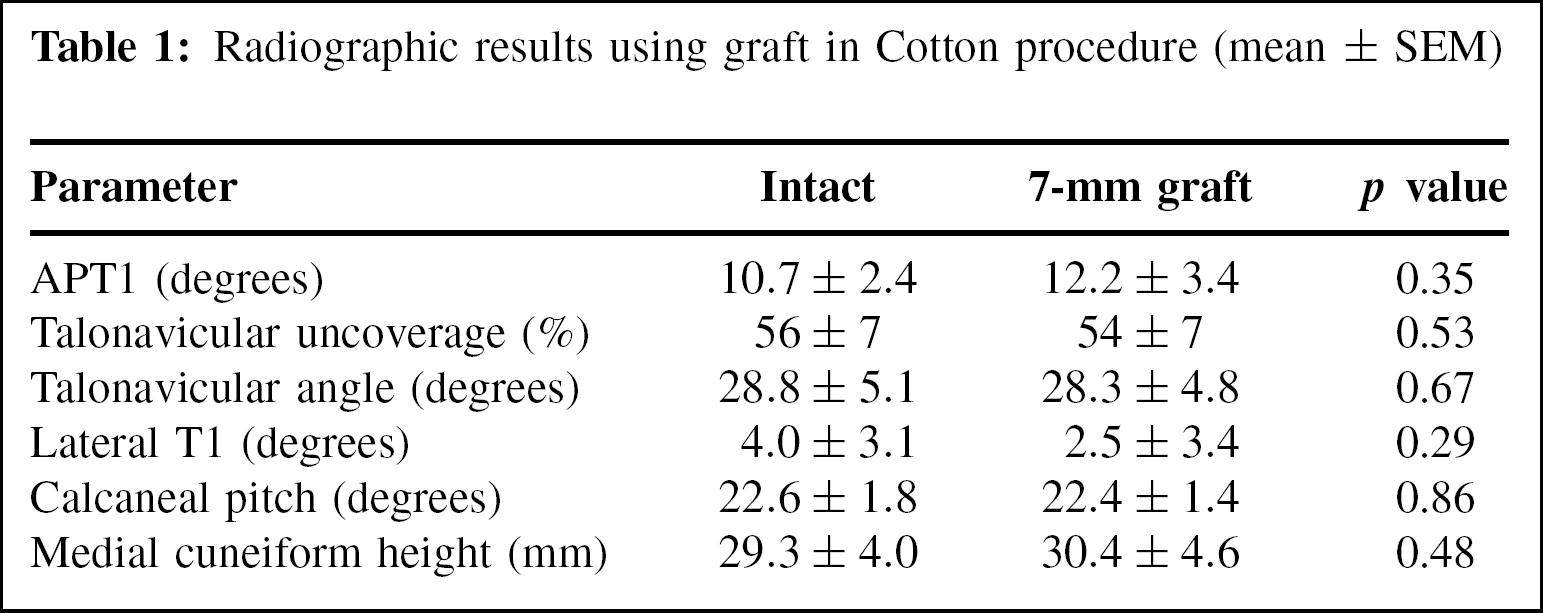
There was no significant difference between the intact specimens for the treatment groups. Radiographic measurements did not show statistically significant changes between the intact foot and the osteotomized foot with either technique except for calcaneal pitch before and after use of the block plate (Tables 1 and 2). There was no significant difference between methods for any radiographic parameter measured.
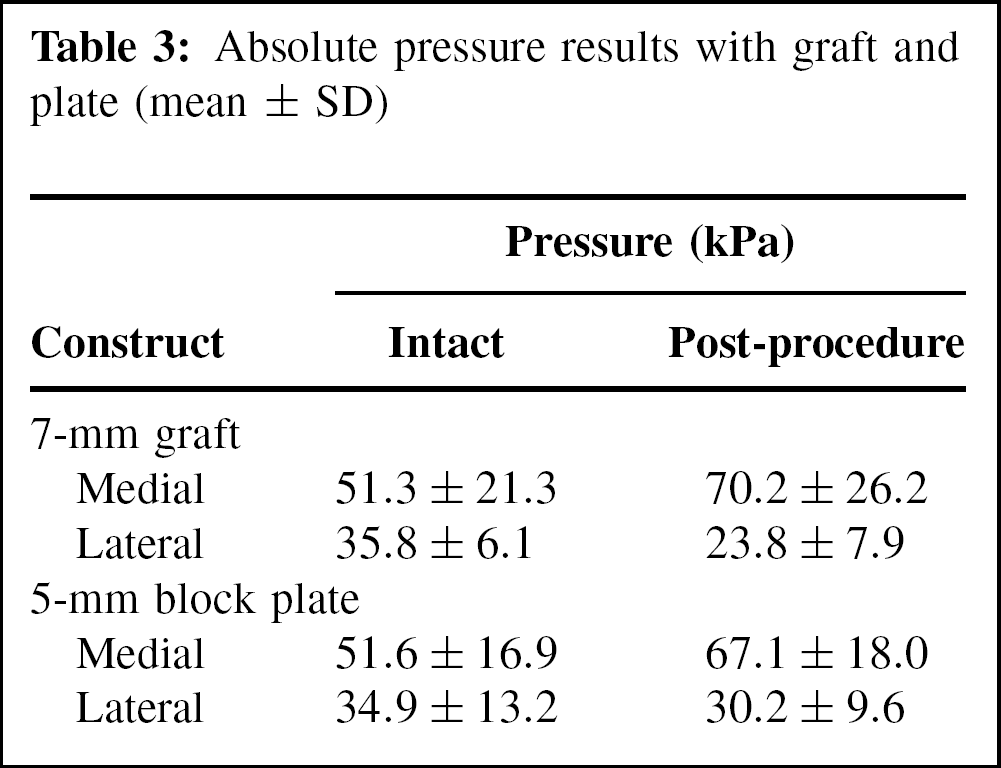
Absolute pressure data are provided in Table 3 for reference. Normalized percent pressure data showed a significant difference both medially and laterally between the intact specimen and the specimen after osteotomy with both methods, with pressure increasing medially and decreasing laterally (Table 4). When the graft group was compared with the plate group, there was no difference in percent medial or lateral pressure (p = 0.25).
Radiographic results using graft in Cotton procedure (mean ± SEM)
Radiographic results using block plate in Cotton procedure (mean ± SEM)
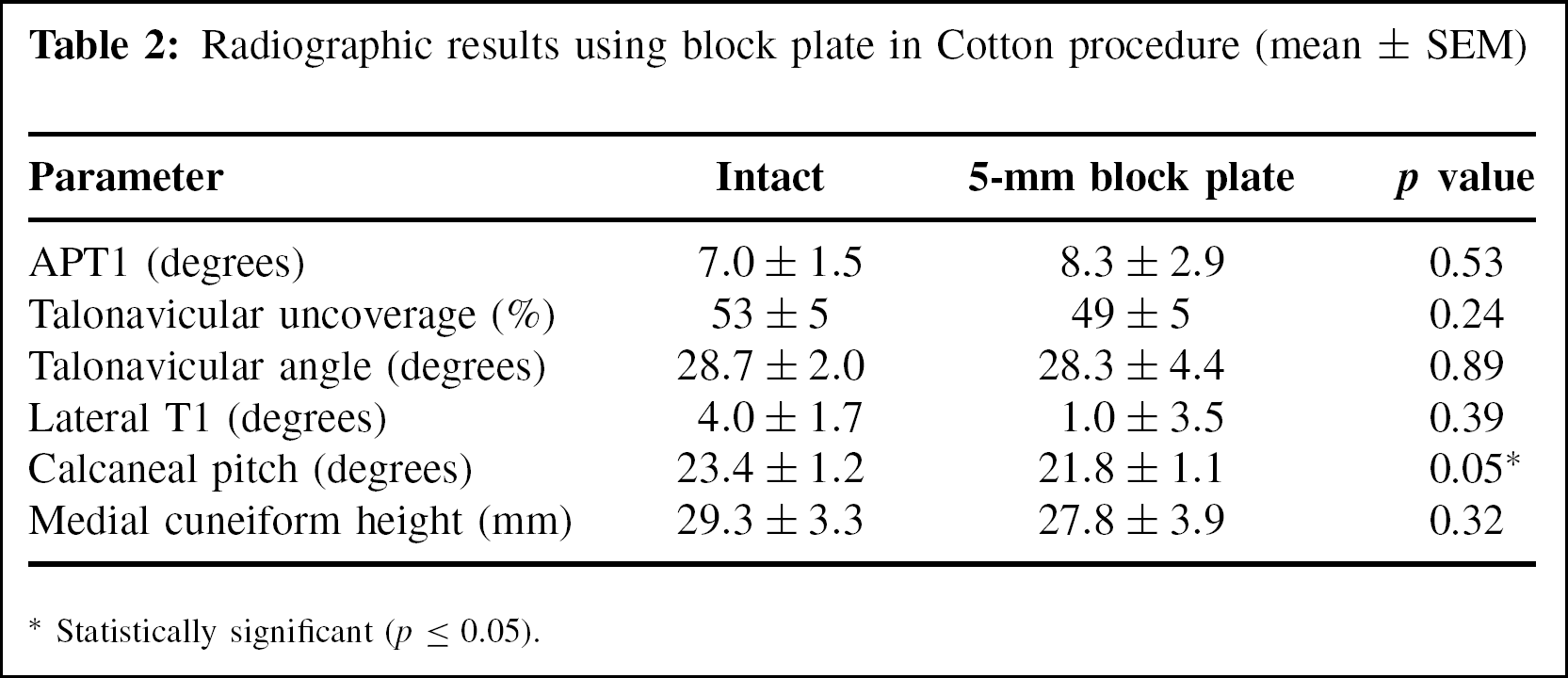
Statistically significant (p ≤ 0.05).
Absolute pressure results with graft and plate (mean ± SD)
Percent pressure results with graft and plate (mean ± SEM)
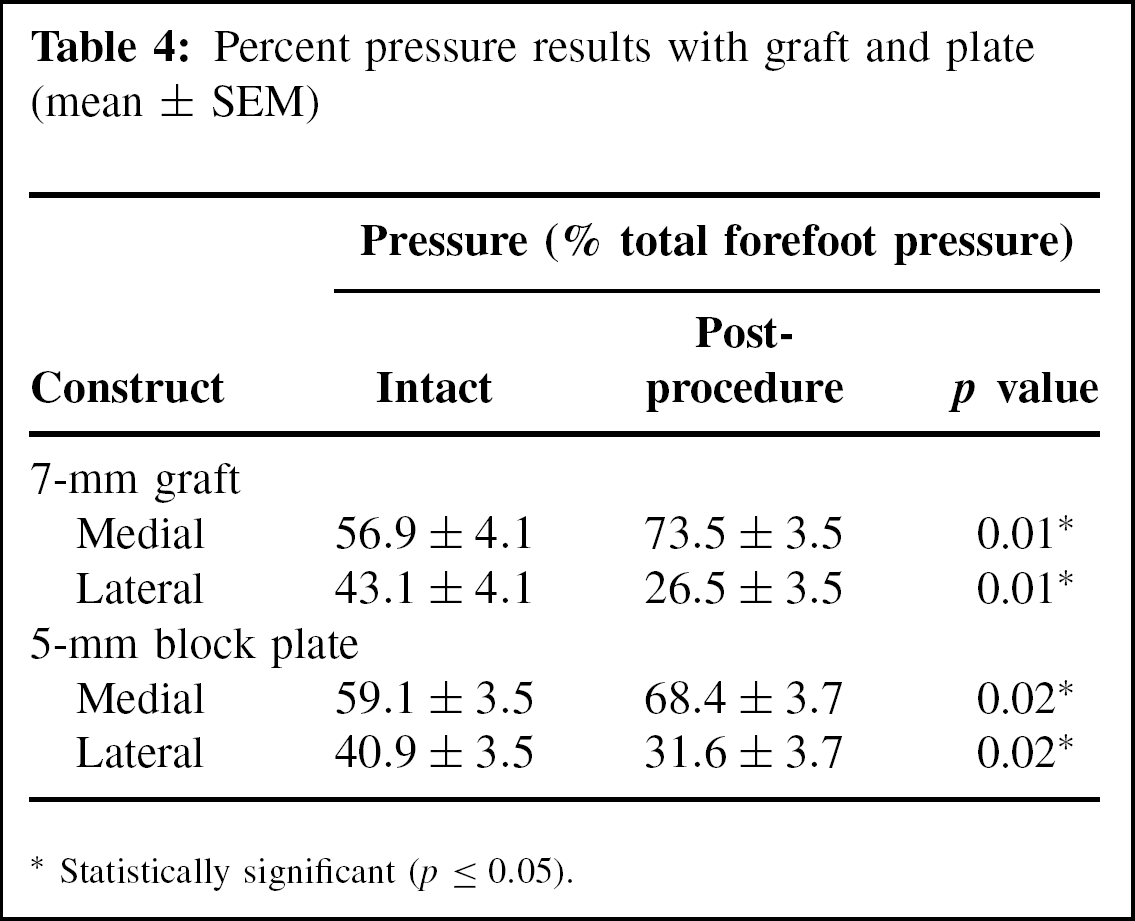
Statistically significant (p ≤ 0.05).
DISCUSSION
The dorsal opening wedge medial cuneiform osteotomy, first described by Cotton, 2 is used in treatment of flexible flatfoot for correction of lateral column overload but has not been studied in isolation. Lateral column overload reflects residual supination of the forefoot elevating the medial column with such procedures as lateral column lengthening used in the treatment of flexible flatfoot 8 or resulting from an existing structurally deficient medial column. Clinical studies have reported improvements using the Cotton osteotomy, 3,4,9 but given the complexity and variability of some of the deformities, the specific impact of the Cotton procedure is difficult to isolate. The current study provides preliminary data on how the Cotton osteotomy contributes to correction, particularly with regard to pressure change from lateral to medial in the forefoot.
The current findings are consistent with those of Benthien et al., 1 who found significant change between the flatfoot and the corrected foot with use of a Cotton osteotomy. These investigators reported radiographic and pedobarographic data with simulated weightbearing in cadaver feet in four sequential conditions: intact, severe flatfoot, lateral column lengthening (LCL)/flexor digitorum longus (FDL) transfer, and LCL/FDL with Cotton osteotomy. Adding a medial cuneiform osteotomy decreased the lateral talus-first metatarsal angle from −7 degrees to −4 degrees, decreased the talonavicular coverage angle from 24 degrees to 20 degrees, and increased the medial cuneiform height from 20 to 25 mm. After the added medial cuneiform osteotomy, lateral forefoot pressure was significantly different from that of the flatfoot (p = 0.01) and was not significantly different from that of the intact foot (p = 0.14). Medial forefoot pressure was overcorrected as compared with the intact foot with the addition of the medial cuneiform osteotomy, indicating a substantial correction with the Cotton osteotomy.
Our pressure findings show that the osteotomy itself has a substantial effect on pressure parameters in balancing the foot with congenital or acquired medial column deficiency or lateral column overload after lateral column lengthening. Based on a theoretical clinical goal of achieving a pressure shift of at least 10% from lateral to medial, both constructs tested met the performance criterion. We found a statistically significant change in pressures in both the medial and lateral forefoot after both fixation techniques. With the bone block, pressure on the medial side was 13% greater than that on the lateral side in the intact specimen and was 47% greater than the lateral pressure after the procedure. Similarly, with the plate construct the intact medial load was 18% higher than lateral load and then was 37% higher than the lateral load after the procedure.
Radiographic change in this model was inconclusive. The small radiographic differences noted in this study fall within the 2- to 3-degree variation in angle measurements taken by different examiners. 5,7 We might have found significant radiographic differences in a flatfoot model, 1 though the differences might not have reached the threshold of clinical importance with the Cotton procedure used in isolation. We did find a significant difference between the intact foot and the post-procedure foot in calcaneal pitch with the plate construct. This difference is not clinically important, but we speculated that the significant results with calcaneal pitch may have occurred because of superior fixation with the plate construct. There was no fragmentation of grafts, and the plate did not dislodge in any sample. The actual block, either metal or bone, essentially served the same function. In the plate construct, the dorsal plate anchored into the bone with screws and may have provided additional support to the construct.
The current study suggests that the block plate should not be excluded from consideration when performing a Cotton osteotomy if allograft is not available. Use of autograft with this procedure has been shown to provide secure fixation, reliable healing, precise correction, usually without supplemental fixation. 3,4 Results with allograft have not been reported, but anecdotal findings suggest that allograft has all the advantages of the autograft, but without the additional potential for complications from iliac crest graft harvest. 3 However, allograft is not always available, and the alternative of autograft harvest may not be desirable. The block plate tested in the current preliminary study could provide an alternative for such situations. Additional studies testing other factors may be warranted to further investigate use of the block plate for this application.
The study was limited in that the openings in the two techniques differed in size. Our first technique utilized a wedge shaped piece of femoral head allograft tapered from 7 mm and providing an opening of 7 mm, the size used most commonly in our operative experience. This was compared to a technique utilizing a relatively new 5-mm block plate, the only size available. Because the block occupied the osteotomy site with a depth of about 2 mm, the corresponding opening distance was likely larger than 5 mm, but there was a difference in the opening size between constructs. It would have been preferable to use a 7-mm block plate to ensure that the osteotomy opening was the same for both constructs. Another study could compare results with openings of the same size and could also look at the effects of progressively increasing wedges or block plates and the impact on the factors studied.
This study has several additional limitations. This biomechanical study was performed on intact specimens, which does not reflect the clinical scenario. However, we believe the substantial pressure shift found in the study may indicate usefulness in the clinical setting. Further, the complexity of the clinical variables found in conjunction with a pes planovalgus foot limits our ability to isolate the impact of this technique. These biomechanical findings do not extrapolate directly to the clinical setting because of the use of this procedure in normal feet and other limitations common to cadaver studies, such as inability to evaluate important factors like stability and time for healing. Finally, we did not consider the effect of bone mineral density on the findings.
The Cotton osteotomy performed with femoral head allograft or an opening wedge block plate on intact cadaver feet produced a substantial shift in forefoot pressures from lateral to medial. These findings suggest that these techniques do not differ in addressing the forefoot pressure imbalance associated with congenital or acquired medial column deficiencies or surgically induced lateral column overload.
Footnotes
ACKNOWLEDGMENTS
The hardware used in this study was donated by the manufactures. The authors thank Lyn Camire for editorial assistance.
EDITOR'S NOTE
The authors are to be commended for performing a sophisticated biomechanical study which nicely demonstrates an increase in medial forefoot pressure after an opening wedge medial cuneiform osteotomy. While a flatfoot model may have demonstrated a slightly different magnitude of change, logic suggests that it still would have demonstrated a significant change in forefoot pressures. However, the clinical validity of the difference between the two surgical methods is unclear as this study by necessity required testing of feet where no graft incorporation had occurred. The block plate would obviate the need for structural autograft but some type of graft would still need to be placed beneath the plate to allow bony healing through a gap of 5 to 7 mm.