
Abstract
Level of Evidence: V, Case Report
INTRODUCTION
Metatarsal head fracture is an uncommon injury and normally co-exists with other fractures of the forefoot. Isolated fracture of the metatarsal head is very rare, with only four reported cases in the literature. 1,3,4,6 The best method for treatment of this fracture is unclear, with both open and closed methods having been used with success. Vascularity of the metatarsal head is precarious and interruption can lead to avascular necrosis. Consideration must be given to the viability and position of the fracture fragment when deciding how to manage these injuries.
CASE REPORT
An 18-year-old student presented to his local hospital, having sustained an injury to his right foot. He had caught his foot in the handle of a bag, causing a forced plantarflexion injury to the second toe. There was immediate pain and dorsal swelling over the metatarstophalangeal joint (MTPJ). Radiographs showed a displaced second metatarsal head fracture with no other injury (Figure 1). The fracture was treated conservatively with buddy taping and an AirCast™ boot.

Initial radiographs from the referring hospital.
After 5 months of conservative treatment, the patient had continued symptoms of unremitting pain over the forefoot and second toe. While walking was possible in the boot, any attempt to walk barefoot or in conventional shoewear was impossible. He also complained of stiffness of his second metatarsophalangeal joint. He was, therefore, referred to the regional foot and ankle center at our institution. On examination, he was found to have a locked second metatarsophalangeal joint with tenderness over the metatarsal head. A CT scan showed a fracture of the metatarsal head, with the base of the proximal phalanx interposed between the articular fragments, causing locking of the MTPJ (Figure 2). Under tourniquet, a dorsal approach was made and the second metatarsophalangeal joint was exposed between the extensor tendons. The capsule was divided, allowing full exposure of the fracture (Figure 3). The joint was unlocked and the dorsal metatarsal head fragment mobilized. The fracture surfaces were debrided and reduced. The head fragment was not found to bleed significantly before or after fixation. Fixation was achieved with two 2.0-mm screws from the Compact Foot Set (Synthes, inc. Paoli, PA). The wound was closed in layers. Postoperative radiographs were satisfactory (Figure 4).
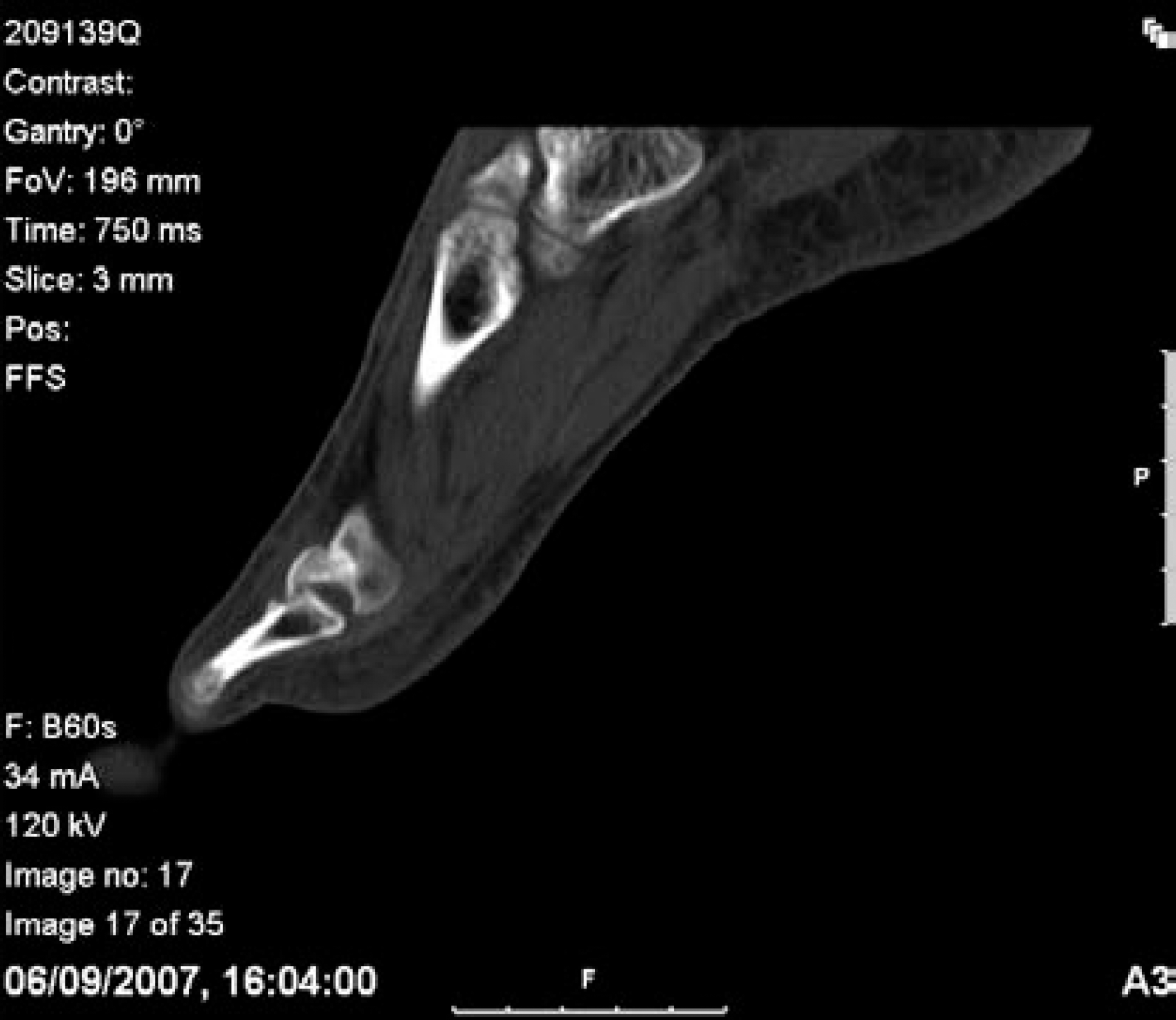
CT scan showing interposition of MTP joint within the fracture fragments.

Intraoperative photograph showing exposure of fracture fragment.

Immediate postoperative radiographs showing fixation.
At 6-month followup, radiographs were satisfactory (Figure 5), the patient was able to walk normally with minimal pain, and had a good range of motion of the second MTPJ.

Six-month followup radiographs (weightbearing).
DISCUSSION
Metatarsal head fractures are rare, and are normally associated with injury to adjacent metatarsals. 3 Isolated metatarsal head fractures are even rarer, and no consensus has been reached regarding their best management. Dutowsky and Freeman 1 described an isolated, osteochondral fracture of the third metatarsal head which was treated successfully with closed reduction. Tanaka 6 , and later Mereddy 4 , describe successful operative fixation of similar fractures. Both of the patients who underwent operative fixation had full resolution of symptoms, with Tanaka's case returning to full athletic activity. Dutowsky and Freeman's case was asymptomatic, but had some residual limitation to the range of motion of the metatarsophalangeal joint.
As with all intra-articular fractures, we believe the greatest prognostic indicator for this fracture type is the ability to adequately reduce the joint surface. If this is not achievable by closed manipulation, then open reduction is necessary. In both Tanaka and Mereddy's papers, closed reduction was impossible. In the case described by Tanaka, it was apparent on plain radiographs that the articular fragment had rotated 180 degrees with the articular surface abutting the fractured end of the metatarsal. In Mereddy's paper, the fragment was displaced medially, and open reduction was performed to preserve the viability of the distal fragment.
The second important prognostic factor is the avoidance of avascular necrosis. The lesser metatarsal heads are supplied from the dorsal metatarsal arteries (which arise from the arcuate artery) and the plantar metatarsal arteries (which arise from the plantar arch). These anastomose approximately 5 to 12 mm proximal to the metatarsophalangeal joint, forming a vascular ring from which small arterial branches run distally into the head itself. 1 This precarious blood supply is at risk from injury in metatarsal head fractures, in distal metatarsal osteotomies or secondary to repetitive minor trauma (as is thought to be the case in Freiberg's infraction). Avascular necrosis can lead to collapse of the joint surface with arthrosis and loose body formation. This situation necessitates salvage procedures such as debridement and bone grafting or extension osteotomy. 2
In this case, the metatarsal head had split in the coronal plane with the proximal phalanx interposed, locking the joint. This position, and the locked position was not appreciated initially. Failure of conservative treatment led to further imaging which demonstrated the need for operative reduction and fixation. The fragment reduced easily and the patient had a good result clinically and radiographically.
While these fractures can be successfully treated with closed reduction, the potential need for operative intervention must be kept in mind. Early operative intervention should be performed when there is significant displacement or rotation of the fracture. This case demonstrates the importance of careful clinical and radiological assessment in these rare injuries.