
Abstract
Background: Elongation of ligaments during early mobilization after reconstruction may be associated with decreased stability. We evaluated elongation of the anterior talofibular ligament (ATFL) before and after lateral ligament reconstruction within a physiologic range of motion with protected and unprotected, isolated dorsiflexion/plantarflexion range of motion. Materials and Methods: Six fresh frozen cadaver legs were used with the ATFL meticulously dissected. A differential variable reluctance transducer (DVRT) was spaced to span the course of the ATFL using consistent placement points based on previous reports. Elongation was measured in a load frame with protected motion of 30 degrees plantarflexion and 10 degrees dorsiflexion for the intact and sectioned ATFL and for the repaired specimen with and without protected motion. The proximal DVRT anchor point was detached for sectioning and repair of the ATFL and replaced at the same position. Testing was 1000 cycles at 1 Hz for the repaired protected specimen and 10 cycles at 1 Hz for all other stages. Results: Initial elongation in the unprotected, repaired group was significantly higher than initial elongation in the intact (p < 0.01), sectioned (p = 0.02), and repaired, protected (p < 0.01) groups. Final elongation in the unprotected repaired group was also higher than final elongation in all other groups (p < 0.01 for all comparisons). Conclusion: The use of protected range of motion of the ankle after lateral ankle ligament reconstruction was not associated with elongation of the ATFL. The ATFL elongated significantly by comparison without protected dorsiflexion/plantarflexion. Clinical Relevance: The study provides biomechanical support for the safety of early protected dorsiflexion/plantarflexion range of motion after Broström reconstruction.
Introduction
The anterior talofibular ligament (ATFL) is of particular interest in lateral ankle instability because it is the most commonly torn ligament of the ankle. ATFL reconstruction with the Broström procedure for lateral ankle instability has been clinically successful. 1,3,7–9,13 Anatomic lateral ankle reconstruction techniques are favored because the procedure restores anatomy and joint mechanics and preserves subtalar motion. 1,3,3,9 Little information exists regarding safe parameters for rehabilitation after lateral ankle reconstruction. One option is nonweightbearing with complete immobilization, and another is weightbearing with protected immobilization and protected mobilization with a removable boot. Some surgeons advocate nonweightbearing with early protected range of motion after repair of the lateral ligament complex to prevent postoperative ankle stiffness, muscle atrophy, and weakness. Karlsson et al. demonstrated that early mobilization after anatomic lateral ankle ligament reconstruction allows for earlier return to sport and greater plantarflexion strength when compared with patients who have been immobilized. 10,11
However, elongation of ligaments during early mobilization after reconstruction may be associated with joint laxity and decreased stability. No studies yet exist evaluating elongation of the intact and repaired ATFL with physiologic range of motion, and thus the biomechanical effect of early motion on ligament elongation is not known. Knowledge of this effect could help establish the amount of motion advisable in the weeks after surgery and could shed light on the effect of protected motion.
The objective of our study was to evaluate elongation of the ATFL before and after lateral ligament reconstruction within a physiologic range of motion with both protected and unprotected isolated dorsiflexion/plantarflexion range of motion. We hypothesized that motion along the course of the sectioned ATFL and protected elongation of the repaired ATFL would be greater than elongation in the intact ATFL for all specimens with protected range of motion. We also hypothesized that specimens with a repaired ATFL and unprotected dorsiflexion/plantarflexion would show significantly greater elongation than all protected specimen groups.
Materials and Methods
Six fresh frozen cadaver legs were used in the study (donor mean age, 80 [range, 71 to 95] years; sex, two males and four females). Specimens were thawed and checked for previous surgeries or deformities, and the leg was sectioned at 12 inches above the sole of the foot. Approximately 4 inches of soft tissue was removed from the proximal tibia and fibula. The remainder of the soft tissue envelope was kept intact. At approximately 8 inches above the sole of the foot, a 4.5-mm fully threaded cortical screw was placed from the posterior aspect of the fibula to the tibia through four cortices. A lateral incision was made along the posterior border of the fibula. Meticulous dissection of the ATFL was then performed.
A 21-gauge needle was placed at the center of insertion of the ATFL 10 mm proximal to the tip of the fibula as measured along the long axis of the fibula. The needle position was used to ensure consistent placement of the proximal differential variable reluctance transducer (DVRT, MicroStrain, Williston, VT) at an anchor point throughout testing. The distal anchor point of the DVRT was then attached to the midsubstance of the ATFL at its talar insertion 18 mm proximal to the subtalar joint (Figure 1). 16 The distal anchor of the DVRT was left in position throughout testing. The Achilles and anterior tibial tendon were exposed, and a No. 5 Ethibond suture using a Krackow suture technique was placed in the cut end of each tendon. The specimen was then mounted by the tibia to the MTS Mini Bionix test frame (MTS Systems Corp., Eden Prairie, MN) (Figure 2).
Inversion range of motion in all specimens was controlled by using a self-adhesive strap applied around the midfoot to limit inversion of the ankle (Figure 2). The strap limited inversion, simulating the effect of using a boot for protected isolated dorsiflexion/plantarflexion range of motion postoperatively. The strap was attached to a weight to elicit dorsiflexion motion for the protected specimens (Figure 3A).
The proximal end of the Achilles tendon was fixed to the load frame (Figure 3A). The intact specimen was cycled by displacement of the piston through an arc of motion of 40 degrees (10 degrees dorsiflexion and 30 degrees plantarflexion) 12 for 10 cycles at 1 Hz to assess elongation of the ATFL ligament. The range of motion was verified during set-up by placing a solid flat surface under the sole of the foot and measuring the angle with a goniometer. Nonweightbearing was chosen to approximate the postoperative protocol in which the patient is allowed to do range of motion exercises daily out of a brace in a nonweightbearing mode. Data were continuously monitored, and data at initial and final cycle were recorded for each test stage. This testing protocol was based on previous findings by Renstrom et al. 15 and Colville et al. 4 who demonstrated that the ATFL had the greatest strain rate with plantarflexion and inversion.
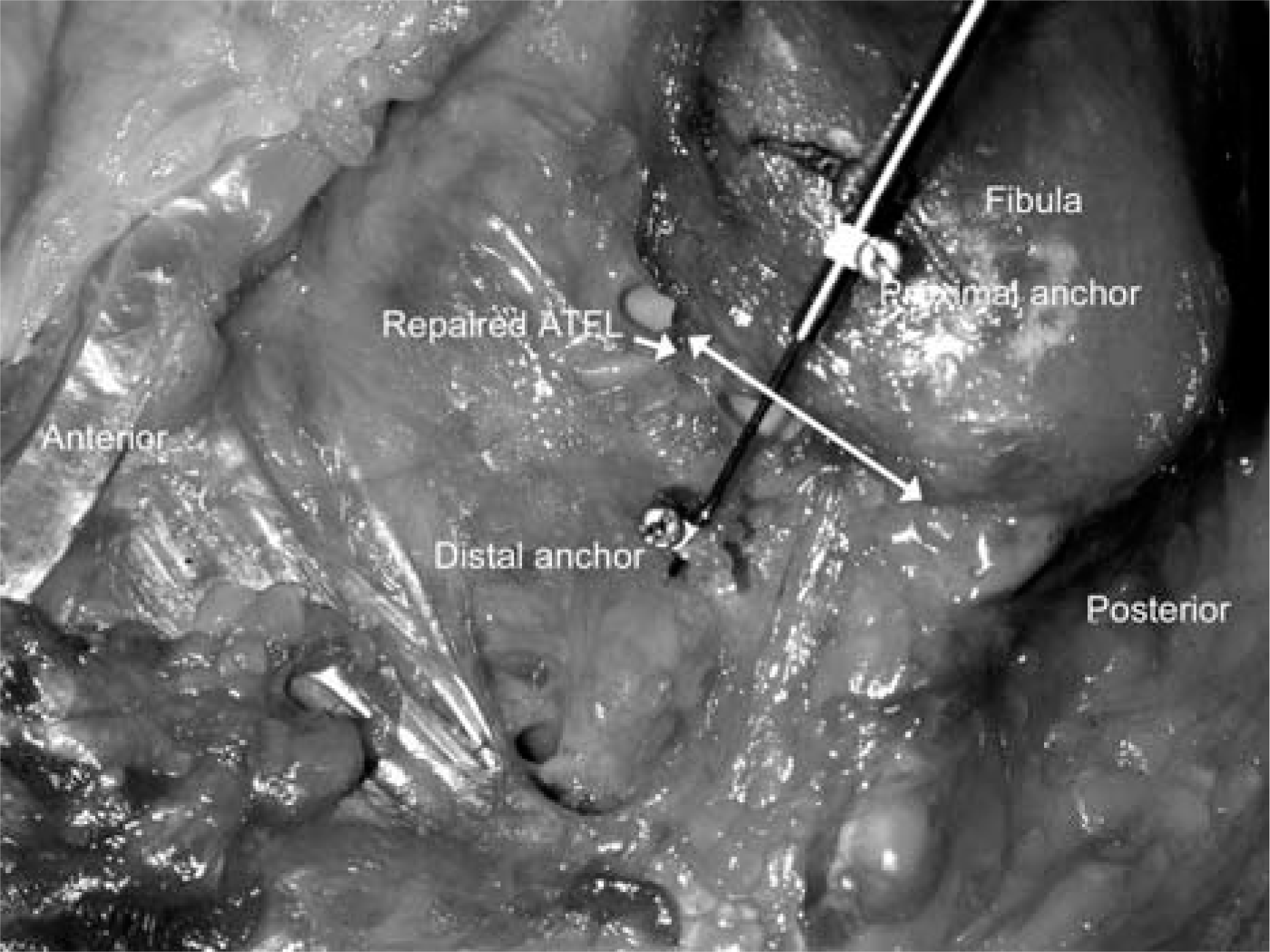
Photograph shows position of DVRT along course of ATFL with the proximal anchor in the fibula and the distal anchor in the talus.

Photograph shows specimen with self-adhesive strap in place to restrict inversion with plantarflexion.
The proximal DVRT anchor was detached, and the ATFL was identified by placing a small hemostat through a 4-mm arthrotomy over the anterior aspect of the fibula at the talofibular junction. While maintaining a full thickness cuff of tissue, the ATFL ligament and capsule were sharply cut 1 mm off the bone extending to the calcaneofibular ligament. The proximal DVRT anchor was replaced at the needle indicating the proximal DVRT position used with the intact ligament. Cycling through an arc of motion of 40 degrees was repeated for 10 cycles at 1 Hz.
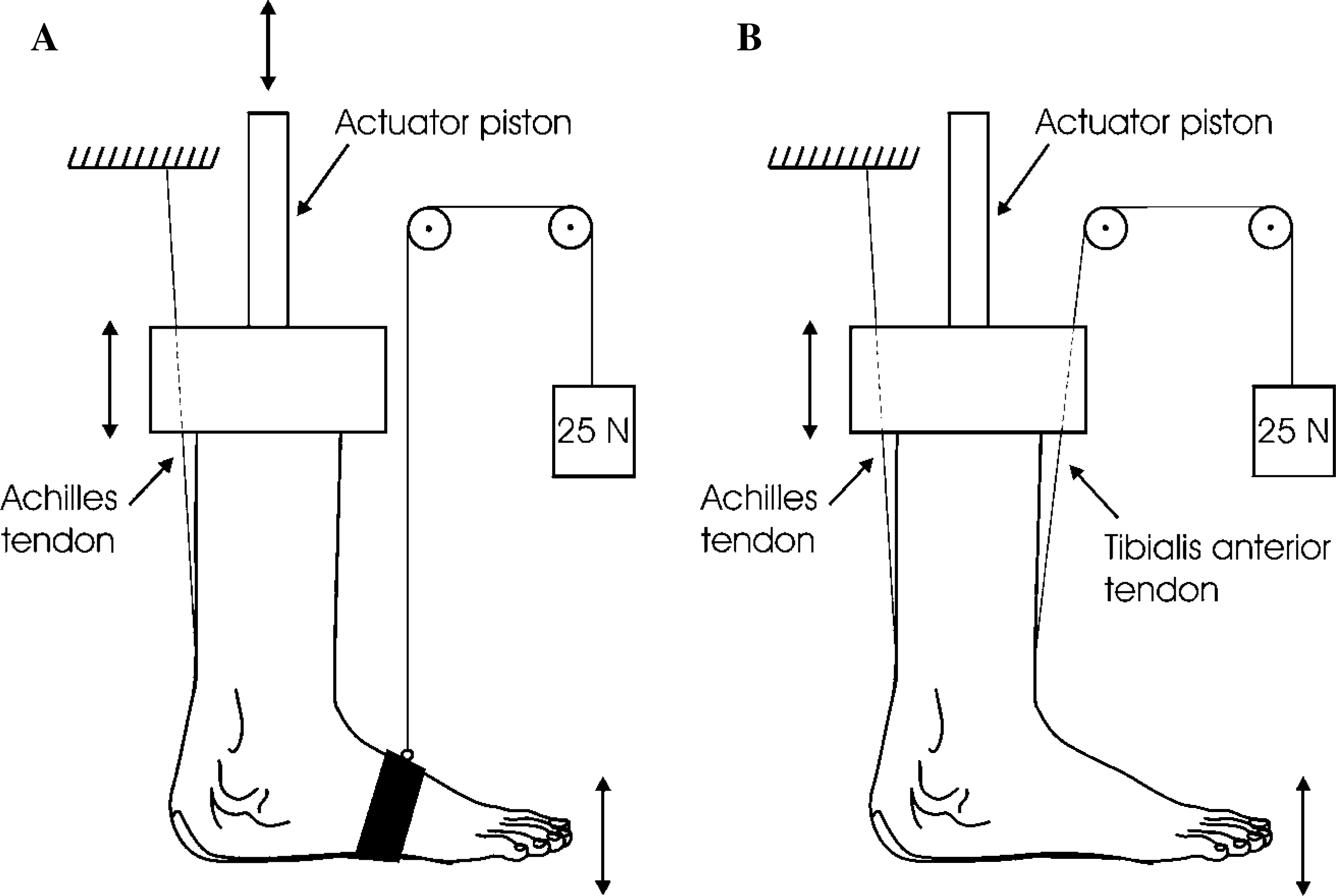
Schematic drawings show test set-up.
The proximal DVRT anchor was again detached and specimens were repaired utilizing the Karlsson modification of the Broström reconstruction. 9 A trough was created with a rongeur in the anterior distal fibula just off the cartilage margin of the talofibular articulation. At the tip of fibula, three parallel drill holes using 0.045 Kirschner wires were made in the direction of the ATFL attachment. The tunnels were created 5 to 7 mm from the edge of the distal fibula and exited in the trough. Using 2-0 nonabsorbable suture, a modified Kessler stitch was utilized to grasp the proximal 1 to 3 mm of ATFL remnant. The sutures were then passed through the drill holes in the fibula following the path created by the K-wire as an assistant removed the wire. The ligament was tensioned appropriately and the knots securely tied as an assistant held the ankle in neutral.
The proximal DVRT anchor was replaced on the fibula, and the specimens were cycled through 40 degrees for 1000 cycles at 1 Hz. This number of cycles simulated the number of times in the early postoperative period (weeks 2 through 6) that this arc of motion would be performed, 20 cycles/day × 50 days = 1000 cycles.
For the last stage, the self-adhesive strap was removed and the tibialis anterior was attached to the 25 N weight to allow movement of the tendon during plantarflexion and apply tension to the tendon for dorsiflexion (Figure 3B). Specimens were cycled through 10 cycles of 40 degrees at 1 Hz to evaluate unprotected movement of the repaired ATFL with physiologic range of motion.
Statistical analysis
Data were collected with Testware (MTS Systems, Eden Prairie, MN). Unpaired two-tailed t-tests were used to compare initial to final elongation data for each cycling stage. Friedman repeated measures analysis of variance of ranks (SPSS, SPSS Inc., Chicago, IL) was used to determine whether the observed differences were significant (p ≤ 0.05). Comparisons were made between protected intact, protected sectioned, protected repaired, and unprotected repaired ligaments at both the initial and final stages.
Results
No difference was found between initial and final elongation of the ATFL at any testing stage except with the unprotected repaired specimens (Table 1). No significant difference was found in elongation between the protected intact, protected sectioned, and protected repaired state. Initial (first cycle) elongation in the unprotected repaired group was significantly higher than initial elongation in the protected intact (p < 0.01), protected sectioned (p = 0.02), and protected repaired (p < 0.01) groups. Final (last cycle) elongation in the unprotected repaired group was also higher than final elongation in all protected groups (p < 0.01 for all comparisons).
Percent elongation for protected intact, protected sectioned, protected repaired, and unprotected repaired ATFL at the initial and final stages (mean ± SEM) (n = 6)
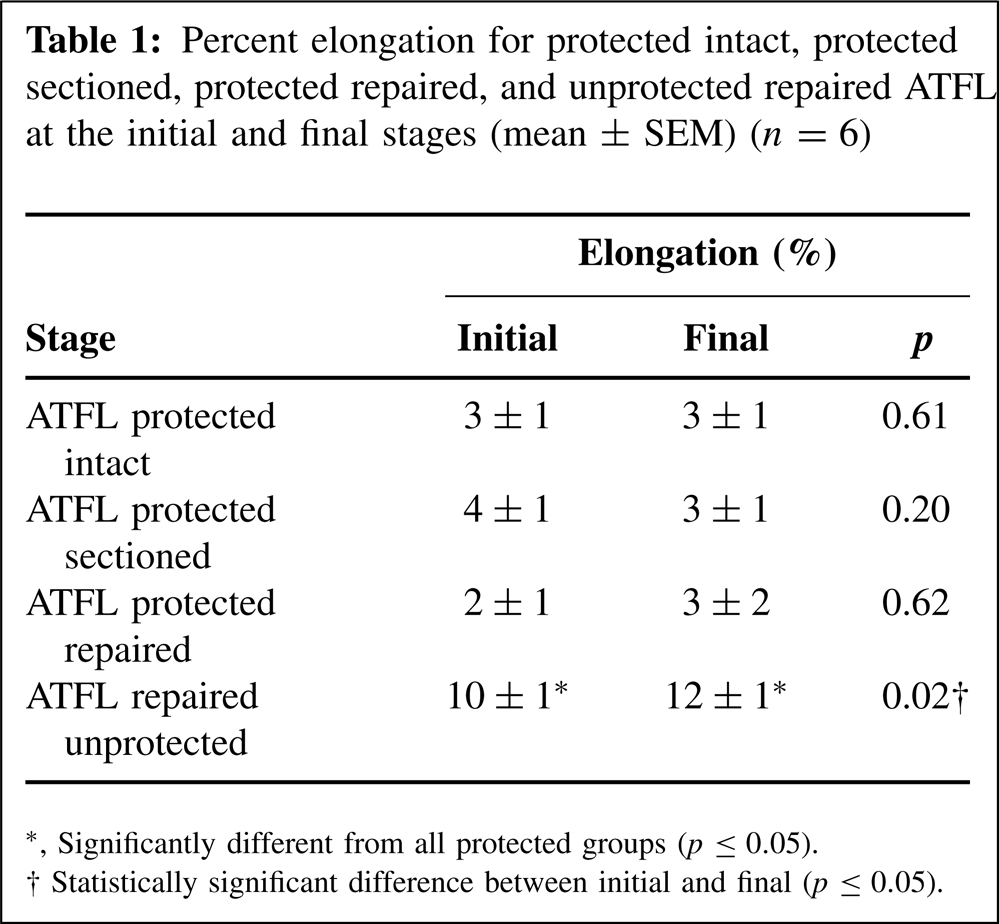
Significantly different from all protected groups (p ≤ 0.05).
Statistically significant difference between initial and final (p ≤ 0.05).
Discussion
The use of protected range of motion of the ankle after lateral ankle ligament reconstruction was not associated with elongation of the ATFL. The ATFL elongated significantly by comparison without protected dorsiflexion/plantarflexion. Although the current study has the limitations of a cadaver study, the findings appear to support the safety of rehabilitation protocols that allow controlled nonweightbearing range of motion exercises after ATFL repair. In compliant patients, the advantage of allowing early range of motion may be important clinically. Complete immobilization, even for short periods of time, may substantially extend rehabilitation time required for full return to activity 5,16,16,17 and causes muscle atrophy. 2 After partial or complete immobility for an extended period, more time may be required for the functional capacity of a ligament unit to return to normal. 14
It is unlikely that nonweightbearing early range of motion is detrimental to ATFL repair. Damaged ligaments show normal histologic changes of inflammation progressing to scar tissue formation as soon as 3 weeks, although ligaments with scar have loads to failure and energy-absorbing capacities of only 60% of normal. 6,14 The strength of the ligament appears to be sufficient for active movement at about 3 weeks. 6,14 Ligaments that undergo repair have a normal histologic picture and good regeneration of ligament tissue with nearly no scar line and good strength within 6 weeks. 16 Motion and stress appear to accelerate ligament healing, but it is not known whether the endpoint of healing is actually changed. 6 The current study suggests that there is no adverse effect of increased laxity with protected range of motion after ATFL repair.
Early protected range of motion has been found effective for rehabilitation after ligament repair. Safran et al. 17 reported range of motion exercises can be performed in the sagittal plane to improve plantar- and dorsiflexion without undue stress to the ligaments after ankle sprain. Booth 2 recommended the use of casts that allow a limited range of joint movement to decrease the amount of muscle atrophy following immobilization. In a study of 40 patients comparing protected motion versus immobilization after modified Brostrom repair, Karlsson et al. 11 reported decreased sick leave, earlier return to sport, improved clinical results, and increased dorsiflexion at 6 weeks with controlled range of motion. In a similar study of 30 patients with 2-year followup, Karlsson and colleagues 10 found that plantarflexion strength was regained more quickly with early mobilization and did not result in short-term or long-term complications such as joint laxity.
Our study supports these clinical findings in that differences in ATFL elongation were not significant between the various test conditions with protected isolated dorsiflexion/plantarflexion. This finding suggests that ATFL elongation is not a concern when the ligament is subjected to protected early mobilization after repair. A possible explanation for this result is that the articular topography of the ankle joint controls ankle motion and ligament tension within a physiologic range of motion and the ligaments act only as secondary restraints to prevent the ankle from moving grossly out of position. This possible interpretation is consistent with results of Tochigi et al., 18 who demonstrated the principal structures that control stance phase ankle motion are articular surfaces rather than the periarticular ligaments. Inversion with range of motion is an important factor distinguishing the current findings from that previous study, and our study did not simulate weightbearing. However, the current data suggest comparison with these earlier findings may be valid.
In the current study, elongation of the ATFL in the unprotected repaired specimens was significantly higher than motion in the protected repaired state and all other states tested. Also, final elongation was significantly higher than initial elongation during cycling of the unprotected repaired specimens. It is not known whether the increased elongation of the ATFL with unprotected range of motion found in this study correlates with a clinically important threshold. However, the lack of difference between the intact, sectioned, and repaired ligaments under protected motion and the significantly increased elongation that occurred with unprotected motion appears to support the clinical use of a boot to restrict early range of motion after ligament repair.
There were several important limitations of this study. The testing of ligaments in elderly cadaveric specimens does not fully reproduce the tissue characteristics seen clinically in young athletic patients in whom this surgery is commonly performed. We are not able to simulate in vivo healing and remodeling in this model. Our model assumes that use of an immobilizing strap mimics the limitation of inversion produced by a standard boot brace. Although exact comparison to a boot brace is not possible, we expect that the boot brace is far more effective in limiting inversion than our strap in this study. We selected two arbitrary points in the ATFL for measurement of elongation in this study. We were able to obtain consistent results using these points, but the results could have been different if other points on the origin and insertion had been selected. Finally, our protocol includes nonweightbearing testing that supports the use of early protected motion but does not address the effect of weightbearing on ATFL repair. Further study with loading could help answer this question. Although we found significant differences for the protected versus unprotected groups, the power to detect differences among the protected groups was low. However, the small differences found between the protected groups suggest these differences may be clinically unimportant.
In conclusion, the use of protected isolated dorsiflexion/plantarflexion range of motion of the ankle after lateral ankle ligament reconstruction was not associated with elongation of the ATFL in this limited cadaver study. Elongation of the ATFL was significantly higher with unprotected range of motion after ATFL repair, suggesting that protected range of motion may prevent injury to the repaired ligament with its subsequent decreased stability.
Footnotes
Acknowledgment
The authors thank Lyn Camire for her editorial work on this paper.