
Abstract
INTRODUCTION
Chronic isolated calcaneocuboid joint instability is an uncommon problem following recurrent ankle sprains and inversion injuries of the foot. It was first described by Krettek and Zwipp in 1986. 16 However, the frequency of chronic isolated calcaneocuboid joint instability may be higher than previously hypothesized 1,6 since establishing the diagnosis is difficult. In case of failure to conservative therapy, several operative treatment options have been described, such as calcaneocuboid arthrodesis and tenodesis with peroneus brevis, plantaris or hamstring tendon. 5,11 –13 The long-term results of arthrodesis of the calcaneocuboid joint or tenodesis are lacking and there are some concerns about the inherent change of foot biomechanics and subsequent development of osteoarthritis in the adjacent joints in young patients. 3 With these considerations in mind Lohrer and Arentz came up with the idea of augmenting and reconstructing the elongated and thinned dorsal calcaneocuboid ligament by a periosteal flap and reported convincing mid-term results in a series of six reconstructed joints. 7 –9 Recently, Punwar et al. reported a reconstructive technique using a hamstring graft in a case of a dislocation of the calcaneocuboid joint. 14 The purpose of this paper is to present a novel, simple, less invasive and effective operative technique that aims to anatomically reconstruct and augment the dorsal calcaneocuboid ligament with an extensor digitorum brevis autograft.
CASE REPORT
A 14-year-old female presented in our clinic after recurrent ankle sprains within the last 2 years. She reported first transient, then permanent, activity related lateral foot pain. In addition, fear of recurrent giving way of the lateral foot and ankle was present. Initially the patient was treated with non-steroidal anti-inflammatories, immobilization until pain relief and proprioceptive training under physiotherapist supervision. But every time she started sport activities, such as basketball, jogging, volleyball or gymnastics, pain on the lateral foot recurred.
Clinical examination at first presentation to our clinic revealed localized point tenderness over the calcaneocuboid joint, increased joint motion compared to the contralateral side and general joint laxity. Furthermore, the pain worsened with inversion of foot. Bilateral proprioceptive weakness in one leg stance was evident.
AP and lateral radiographs of the foot did not reveal any pathological findings. Besides a minor hyperintensity at the cuboid, the T2- and proton density-weighted MRI indicated no abnormality (Figure 1). Stress radiographs in comparison to the contralateral side demonstrated significant laxity of the calcaneocuboid joint during inversion of the foot. An intra-articular infiltration with local anesthetic led to temporary relief of pain.
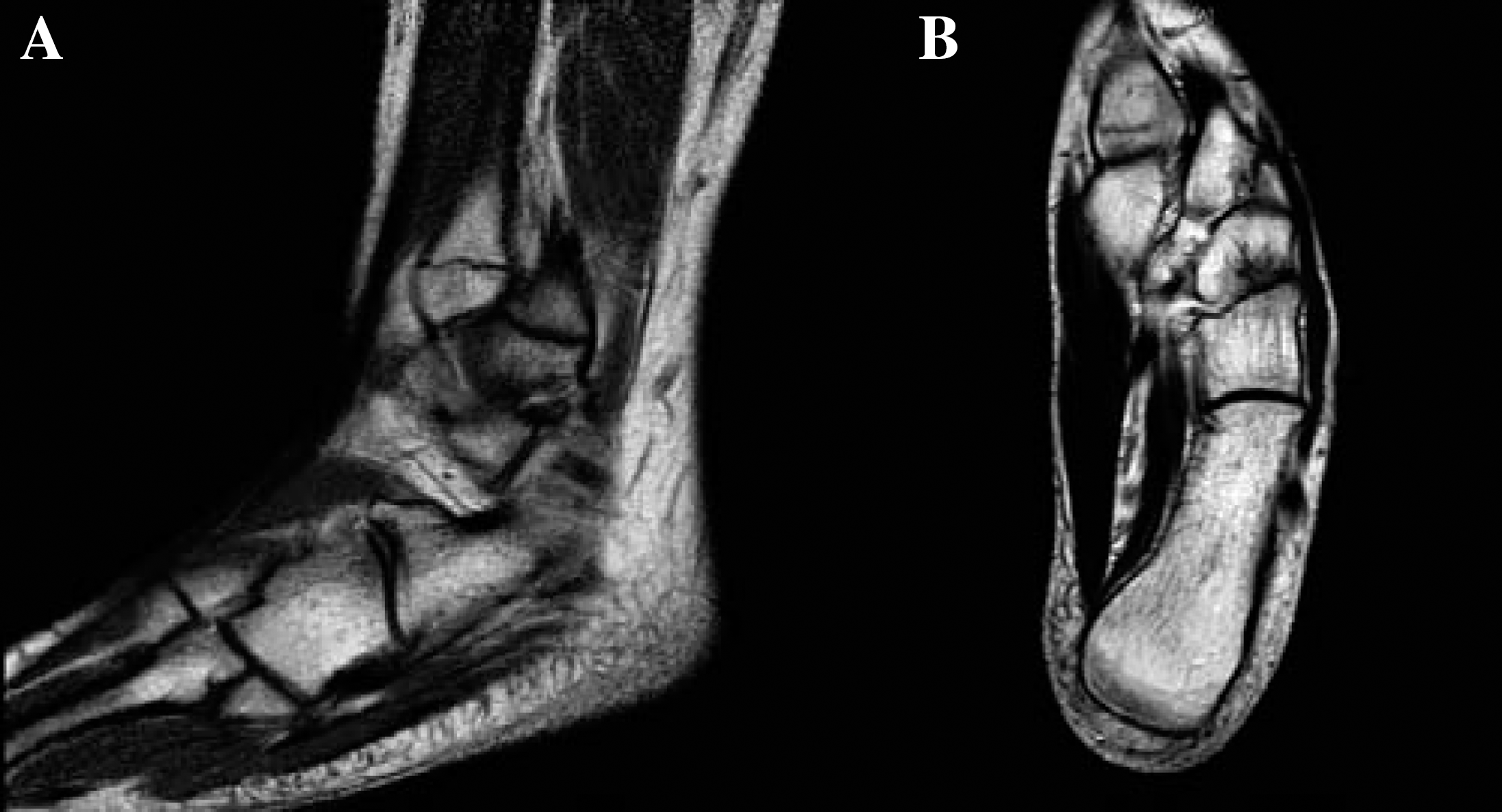
Preoperative MRI of left calcaneocuboid joint.
Conservative treatment with casting, taping and an orthotic device did not result in lasting relief of the symptoms. Non-surgical and surgical options were discussed with the patient and her parents at length and the decision for a reconstructive stabilization of the calcaneocuboid joint was made. The operative technique is described below.
The patient was followed with radiographs (Figure 2) and clinical assessment regularly and at 6 months after surgery. At last evaluation, 6 months postoperatively, she had no pain. The patient was completely satisfied and successfully returned to school sport activity. The American Orthopaedic Foot and Ankle Society Hindfoot Scale and the Foot and Ankle Outcome Score (minimum 0 to maximum 100) was 100. 4,15

Postoperative radiographs at last followup 6 months after procedure.
OPERATIVE TECHNIQUE
The patient was positioned supine with knee flexed and the foot 20 degrees internally rotated. A tourniquet was used. Antibiotic prophylaxis of 2g ceftriaxone was administered. The calcaneocuboid joint was palpated and the landmark structures of the peroneus brevis tendon and lateral muscle belly of extensor digitorum brevis muscle were identified. Between those structures, a straight skin incision of 3cm length, perpendicular to the dorsal calcaneocuboid joint was made. The fascia of the extensor digitorum muscle was split and the tendinous part of the extensor digitorum brevis muscle was identified and separated. A 3 cm long × 0.5 cm wide flap was prepared and the belly of the extensor digitorum muscle was retracted dorsomedially. After separation of the joint capsule, the elongated and thinned dorsal calcaneocuboid ligament was identified and the laxity was proven by inversion, supination and plantarflexion of the foot. The prepared flap was detached at the cuboid and flipped over to the dorsal calcaneocuboid ligament. After tensioning of the tendinous muscle flap in slight eversion of the foot, it was reattached by a suture anchor (Mitek GII, DePuy GmbH, Germany) to the cuboid approximately 0.5 cm plantar of the original insertion. Additionally, the former calcaneocuboid ligament was reefed and augmented by a double layer suture (Vicryl 2-0, Ethicon, Germany) of the joint capsule. Finally, the fascia of the extensor digitorum brevis muscle, subcutaneous tissue and skin were closed in layers.
After surgery the foot and ankle were immobilized for ambulation in a cast in neutral position for 2 weeks. After 2 weeks the cast was removed and full weightbearing with an orthotic shoe including a medial stabilizing inlay was initiated for 10 more weeks. Return to sport activity was allowed 12 weeks postoperatively.
DISCUSSION
A novel, simple, less invasive and effective operative technique for the treatment of chronically unstable calcaneocuboid joints is described. The calcaneocuboid joint was stabilized by augmentation of the dorsal calcaneocuboid ligament with an extensor digitorum brevis muscle flap fixed with a suture anchor to the cuboid. In contrast to the previously described joint arthrodesis or tenodesis with peroneus brevis or plantaris tendon, this new method aims to address the joint instability with possibly less morbidity and without compromise of lateral foot stability. 5,11 –13 Additionally, the inherent change of lateral foot biomechanics by the other procedures may lead to a load shift from the calcaneocuboid to adjacent joints. This may be even more devastating in young patients as it may result in early osteoarthritis and subsequent need for secondary operations. In fact, Astion et al. found that in a cadaver model, an arthrodesis of the calcaneocuboid joint reduced the range of motion of the talonavicular joint to a mean of 67 percent and the excursion of the posterior tibial tendon to a mean of 73 percent. 2 We believe that both procedures are inadvisable in young patients.
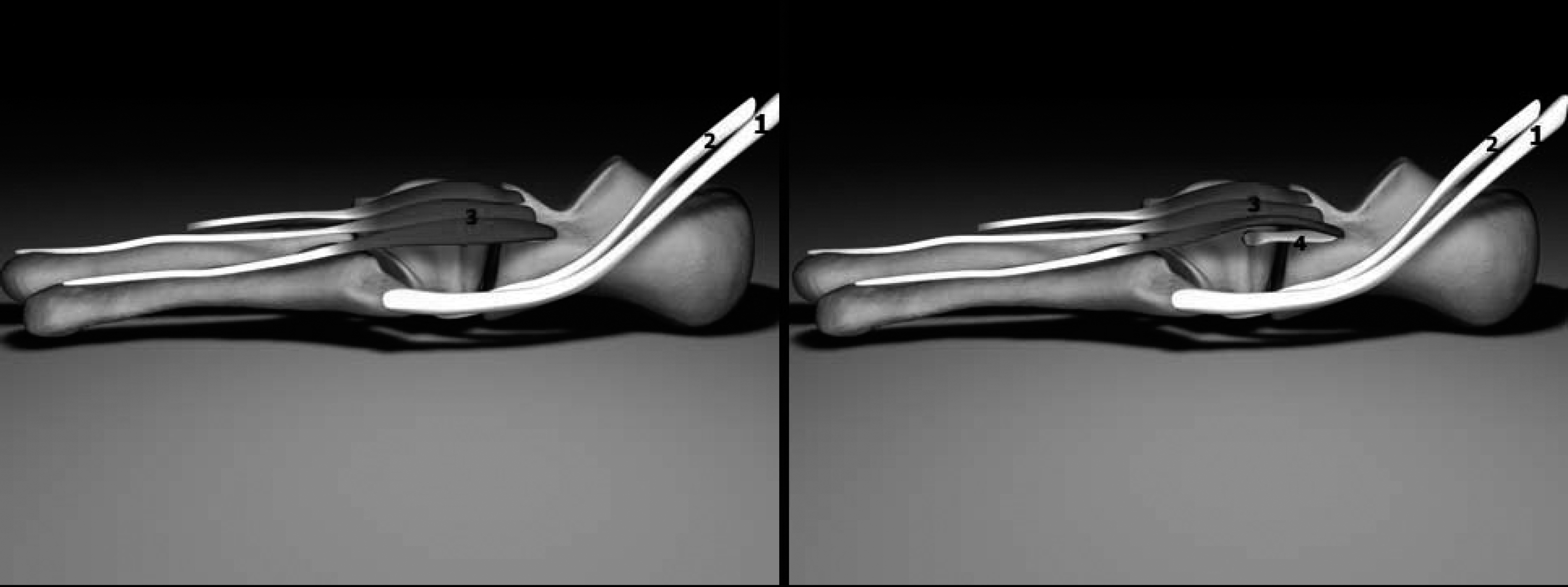
Schematic illustration of calcaneocuboid joint anatomy - peroneus brevis (1) and longus (2) tendon with nearby origin of tendinous part of extensor digitorum brevis muscle (3) and dorsal calcaneocuboid ligament (4).
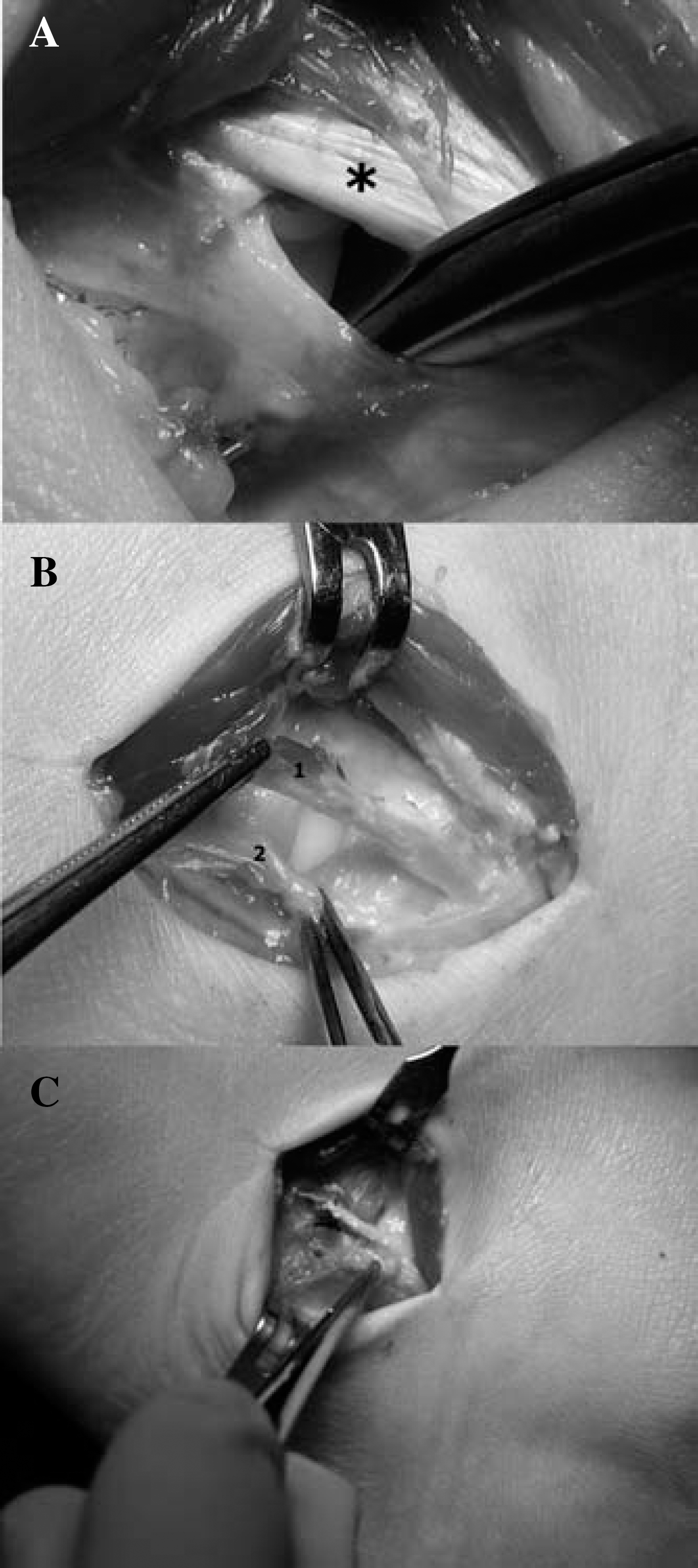
Dorsal calcaneocuboid ligament reconstruction of left foot.
Thus, care must be taken to reconstruct the normal lateral foot anatomy as accurately as possible to preserve the sophisticated equilibrium of hind- and midfoot biomechanics. Recently a less invasive reconstructive technique of repair of the dorsal calcaneocuboid ligament with a periosteal flap from the lateral calcaneus was introduced by Lohrer and Arentz. 7,8,10 In a series of five consecutive patients excellent functional and radiological outcomes were reported. 9 Furthermore, the biomechanical stability of the double layer periosteal flap reconstruction was proven. 10
Like Lohrer's, our reconstructive technique can be performed through one small skin incision as the graft lies directly adjacent to the calcaneocuboid joint. Alternative allografts are not commonly available in Europe. In addition, we believe care must be taken to avoid use of autografts like hamstring or plantaris tendon. 1,14 In case of failure of our described reconstruction technique, reconstruction with a periosteal flap repair, hamstring tenodesis or arthrodesis remains feasible.
Our case further emphasizes the fact that establishing the diagnosis of an unstable calcaneocuboid joint may often be difficult. Besides a thorough clinical examination, stress radiographs with the forefoot adducted in comparison to the contralateral side 1 and intraarticular infiltration with local anesthetics are considered to be helpful, particularly in questionable cases.
The presented case of a 14-year-old patient demonstrated good subjective and functional resulting in a pain-free and stable joint 6 months postoperatively. Our technique seems to be a promising alternative treatment option to the periosteal flap repair in patients with chronically unstable calcaneocuboid joints. However, one could argue that a muscle would not provide much support for stability of the calcaneocuboid joint, but we used the tendinous part of the extensor digitorum brevis muscle. Thus, the reconstructive flap theoretically has more characteristics of a tendon than a muscle. Intraoperatively the stability was tested before and after reconstruction and a definite increase of stability was observed, which supports our point of view that this flap adds relevant stability to the joint. An increase of stability due to scarring of soft tissue alone would not be observable until weeks after surgery. Tensile testing of the reconstuctive flap and calcaneocuboid joint should be performed to answer the question of which grade of joint instability allows the use of this reconstructive technique and will allow the comparison of the construct stability to the periosteal flap repair.
Finally, our favorable experience was obtained from just one case, and has to be confirmed by a larger series of patients. Due to the rarity of the injury it may only be possible in a multi-center setting.