
Abstract
Background: There are limited studies on the long term outcome of Mitchell's osteotomy for hallux valgus deformity. We present the long term results of 204 cases. Materials and Methods: Postoperative clinical and radiological evaluation with a mean follow up of 12.9 years was performed on patients with preoperative hallux valgus angles (HVA) of up to 50 degrees and intermetatarsal angles (IMA) of up to 20 degrees. Two crossed Kirschner wires were used to fix the capital fragment; lateral soft tissue release performed when deemed necessary. Comparisons were made between the pre- and postoperative measurements using a Mann-Whitney U-test. Statistical significance was defined at p < 0.05. Results: The mean AOFAS score improved from 49.6 to 87.9 points (p = 0.004). There was significant improvement in the HVA and IMA, 33.8 degrees versus 16.1 degrees (p = 0.002) and 15.2 degrees versus 8.2 degrees (p = 0.004), respectively. Fifty-seven cases (27.9%) had preoperative HVA greater than 40 degrees but only 16 required lateral soft tissue release with no significant difference in the postoperative HVA (21.3 versus 20.8, p = 0.08). There was a significant change in lateral metatarsalgia and symptomatic callosities (18.3% versus 11.8%, p = 0.023). In 97.6% of cases the patients were satisfied with the overall result. Revision surgery was performed in five cases (2.5%). Conclusion: Mitchell's osteotomy was a reliable technique with successful outcome and low complication rate when performed with Kirschner wire fixation and lateral soft tissue release when appropriate. It may also be successfully performed with hallux valgus angles greater than 40 degrees.
Level of Evidence: IV, Retrospective Case Series
Introduction
More than 130 different procedures have been described for the treatment of hallux valgus deformity ranging from first metatarsophalangeal (MTP) joint fusion, excisional arthroplasty to distal first metatarsal or basal first metatarsal osteotomy. 10 Regardless of the procedure, the aim is pain relief, restoration of function, and correction of the deformity. Mitchell's procedure includes an osteotomy of the distal part of the first metatarsal, lateral displacement and angulation of the metatarsal head, exostectomy and capsulorraphy. 8,17 Mitchell's osteotomy has been reported to give satisfactory correction of the deformity in more than 80% of cases. Most reports though present short- to mid- term results, often with small numbers of patients. 6,9,17,20,23 The aim of our study was to evaluate the clinical and radiographic results in a large number of patients at longer followup.
Patients and Method
Study group
We identified from our units' database a total of 184 patients (220 feet) treated with Mitchell's procedures between 1986 and 2001 for hallux valgus deformity. We did not include any patients with coexisting clinical and/or radiological evidence of major congenital lesser metatarsal deformities or rheumatoid arthritis. Cases with co-existent prominent metatarsal heads, callosities, subluxation/dislocation of lesser metatarsal joints, and lesser toe deformities were treated as indicated. We had no cases with previous fractures. Osteoarthritic MTP joints were also included. Seven patients died and nine could not be located. A total of 168 patients (204 feet) were therefore recalled for clinical and radiological evaluation. In addition we analyzed preoperative, intraoperative and postoperative notes and X-rays.
The preoperative protocol included an assessment of severity and site of pain, analgesic or walking aid requirements, limitations of daily activity or sporting ability, requirements for footwear, walking difficulties on uneven surfaces, MTP joint and interphalangeal joint movement, the presence of bunion, callosities and cosmesis. This allowed retrospective conversion into the hallux score according to the American Orthopaedic Foot and Ankle Society (AOFAS). 12 Postoperative assessment for the purposes of the study was performed at a mean of 12.9 years after surgery and included clinical examination of the patient generating an AOFAS hallux score. Weight bearing AP radiographs were obtained pre- and postoperatively (at the 12.9 year followup point) to measure the hallux valgus and intermetatarsal angles (HVA, MTPA, and IMA, respectively) as described by Miller, 16 Schneider and Knahr, 19 and Schneider et al. 18 Sesamoid shift was defined as the distance between the center line of the first metatarsal and the medial border of the lateral sesamoid. 25 In addition we measured the length of the first, second and third metatarsal. The patients were asked whether they were satisfied with the overall result of the procedure or not. Clinical and radiological measurements at the immediate postoperative period were not evaluated for the purposes of this study.
Indications for surgery
Indications for surgical intervention were pain, functional disability, limitation of daily activities, cosmetic issues and shoe fitting problems. We treated all patients with HVA of up to 50 degrees and IMA of up to 20 degrees with Mitchell's osteotomy. Surgery for cosmetic issues alone was not offered, therefore surgery was not performed when pain or hindrance of activities of daily living were absent, even if the hallux valgus was severe. Per the senior authors' (GP and KK) protocol, any patients with a first metatarsal more than 5 mm shorter than the second metatarsal were offered alternative procedures in order to avoid excessive first ray shortening which has been shown to correlate with lateral metatarsalgia. 3,20,21
Surgical technique
The procedure was performed by two senior authors (GP and KK) using the technique described by Mitchell. 8,17 The lateral spike was determined according to the deformity of the IMA. For IMA up to 12 degrees the spike width performed was 1/3 of the metatarsal head. For IM angles more than 12 degrees the spike left was 1/2 of the metatarsal head (Figure 1). The spike osteotomy was made with a reciprocating saw of 5 mm width. We performed the distal, smaller osteotomy and then the proximal osteotomy of the whole of the metatarsal width. Thereafter we used rongeurs to remove the medial bone step. We used a modification of the standard technique by inserting two percutaneous crossed Kirschner wires to fix the osteotomy instead of sutures 10 (Figure 2). We did not use any other method of fixation. If the hallux valgus could not be corrected by gently pulling the medial capsule attached to the proximal phalanx toward the center of the metatarsal, lateral soft tissue release of the first MTPJ was performed. If minimal dissection was desired, a small incision on the lateral capsule was made from inside the joint, but if a more extensive dissection was necessary through the joint capsule, a new skin incision was made in order to dissect the adductor hallucis. The decision to perform lateral soft tissue release was not determined by any radiographic finding. It was always an intraoperative judgement based on the difficulty of hallux valgus correction due to the degree of soft tissue contracture prohibiting and interfering with the capsular repair. We did not perform any specific additional procedure for correction of the sesamoid shift or the distal metatarsal articular angle.

Preoperative X-ray demonstrating osteotomies performed during Mitchell's procedures. Dotted line represents initial bunionectomy. Solid lines represent distal (smaller) and proximal (whole metatarsal width) osteotomies. Shaded area represents bone that was removed using the above osteotomies to produce the lateral spike.
Postoperatively, a walking inframalleolar foot cast was applied to allow the soft tissues to heal and the patients were encouraged to bear weight on the heel. As soon as the swelling subsided, the cast was removed and full weight bearing mobilization with the foot flat was allowed at 6 weeks following surgery provided there was radiologic evidence of osteotomy union. The Kirschner wires were removed 4 to 5 weeks postoperatively. Patients attended the clinic at 3, 6, and 12 months postoperatively and every three years thereafter. HVA less than 10 degrees and HVA greater than 15 degrees were considered to be over-correction and under-correction, respectively. According to the senior authors' policy, patients were offered revision surgery if there was overcorrection or under-correction interfering with shoewear.

The osteotomy was securely fixed with two crossed Kirschner wires to prevent dorsal displacement and angulation.
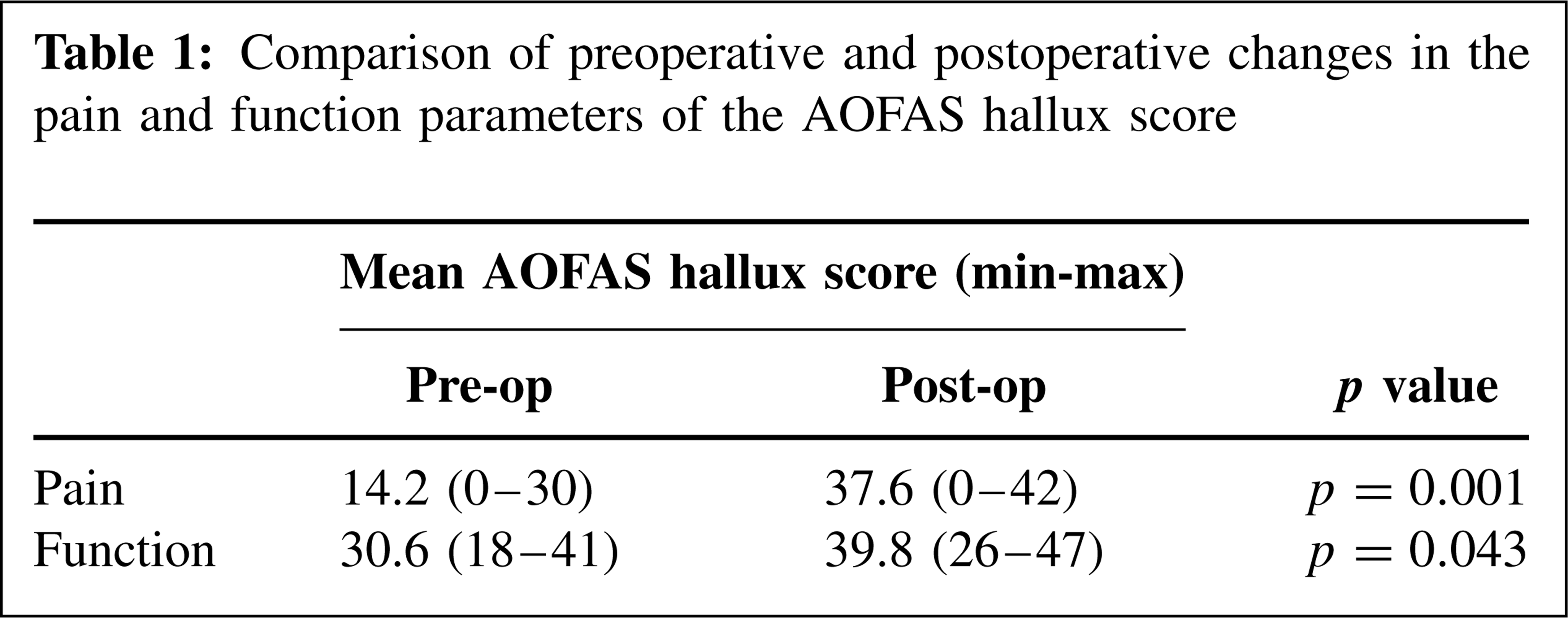
Comparison of preoperative and postoperative changes in the pain and function parameters of the AOFAS hallux score
Statistics
We created a database using STATISTICA for windows 5.0 (StatSoft, Inc., Tulsa, OK). Mann-Whitney U-test was used to analyze the data. Statistical significance was defined at p < 0.05, in order to avoid a Type I statistical error due to the large number of comparisons. 1 We did not perform a power analysis.
Results
We had a total of 152 women (187 feet) and 14 men (17 feet) available for review. The mean age at time of surgery was 58 (range, 22 to 76) years. The mean followup for both groups was 12.9 (4.6 to 19.8) years.
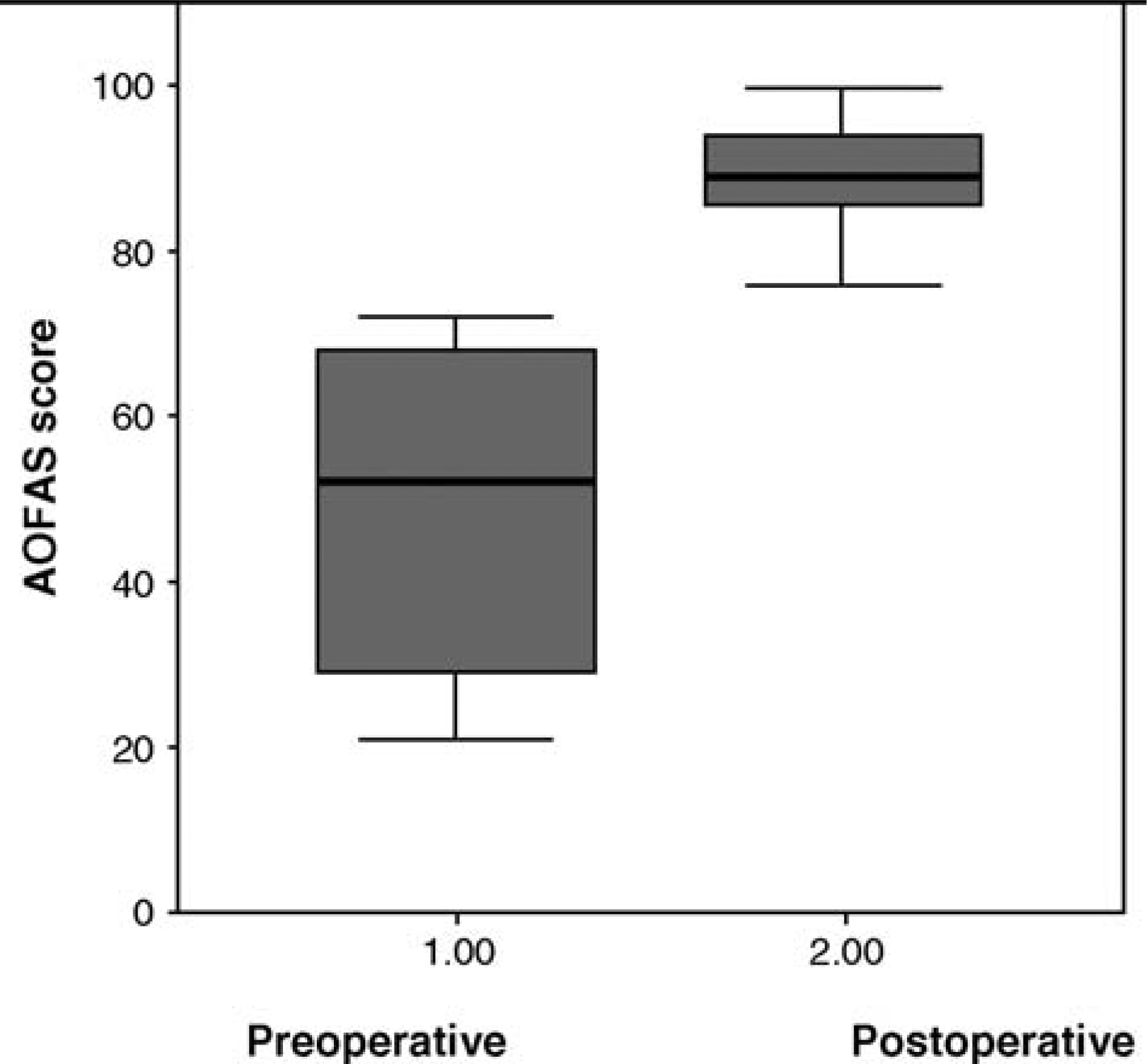
Improvement in the mean AOFAS hallux score from a preoperative of 49.6 (SD = 17.7) to a postoperative of 87.9 (SD = 10.9) points (p = 0.004).
In 97.6% of operated feet the patients stated that they were satisfied with the overall result. There was a statistically significant improvement in the mean AOFAS score from 49.6 to 87.9 points (p = 0.004) (Table 1 and Figure 3). There was a statistically significant improvement in the pain score. A difference was also noted between the pre- and postoperative function score (p = 0.043). There was no difference between the preoperative and postoperative mean range of motion (combined plantarflexion and dorsiflexion) of the first MTP joint preoperative = 71.4 degrees ± 35 versus postoperative = 72.6 degrees ± 31.4 (p = 0.84).
Comparison of preoperative and postoperative changes in hallux valgus (HV) angle, intermetatarsal (IM) angle and sesamoid shift.
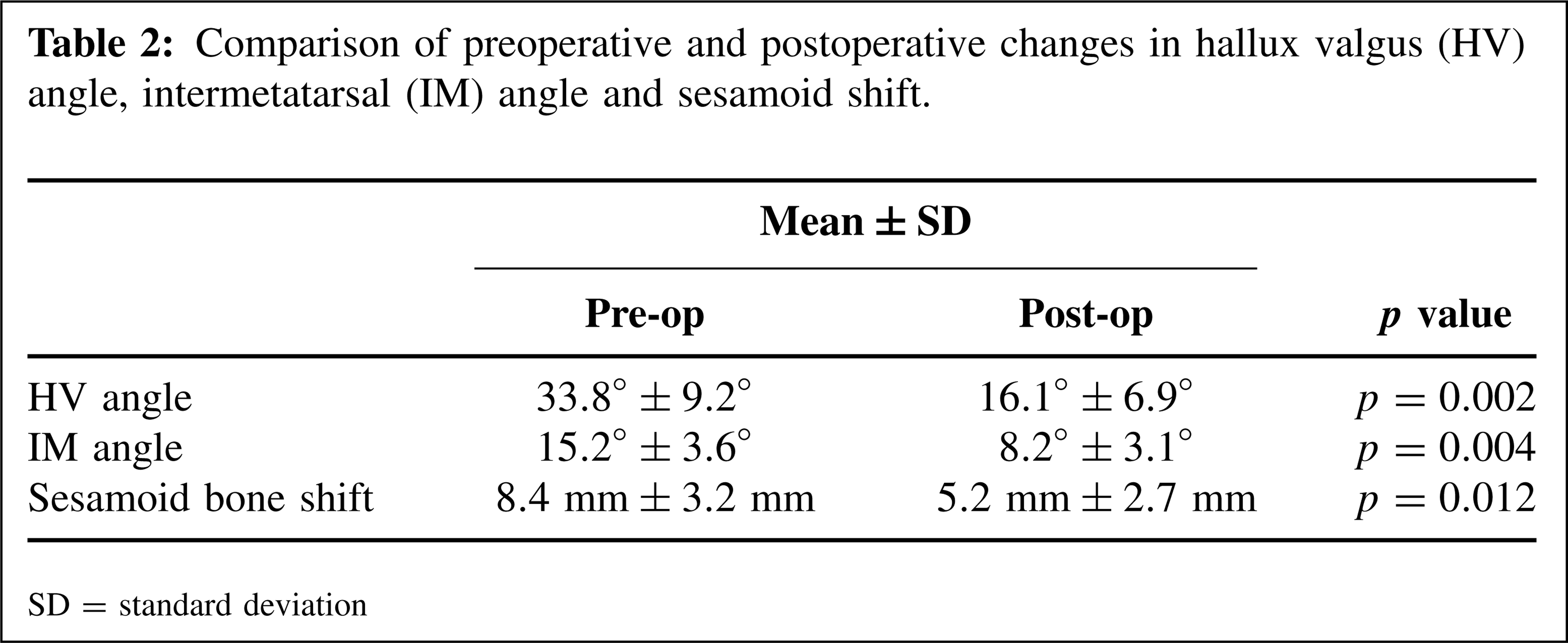
SD: standard deviation
Significant improvement between the pre- and postoperative HVA and IMA was found but not in the sesamoid shift (Table 2). Fifty-seven cases (27.9%) had HVA greater than 40 degrees. Lateral soft tissue release was performed in only 16 of these cases. The mean postoperative HVA in this group of patients was 21.3 degrees ± 11.8 degrees which was not significantly different from the mean HVA of the group not requiring lateral soft tissue release (20.8 degrees ± 13.1 degrees), p = 0.08.
The mean difference between the first and second metatarsal bone length was 4.2 mm. There was a decrease in the preoperative versus postoperative incidence of lateral metatarsalgia and symptomatic callosities, 18.3% and 11.8% respectively (p = 0.023).
We had a total of 14 cases in 14 patients with complications. These included over-correction in one case and painful recurrence in four cases. These five cases underwent revision surgery as the patients were not satisfied with the results of the initial surgery. In the case of over-correction the revision surgery was performed soon after it was diagnosed at the first clinic appointment. In addition, we had three cases with under-correction of the deformity but none of which requested revision surgery as they were satisfied with the overall result. There was one case of avascular necrosis of the metatarsal head which is still pain-free. This patient did not have a lateral release. There were also three minor superficial wound infections and two cases of delayed union.
Discussion
Distal first metatarsal osteotomies have been reported to correct the HV deformity in 82% to 95% of cases 4,7,11,16,17 and two large series reported good or excellent results in 91% and 97% of patients. 2,8 In our study the clinical results were satisfactory and 97.6% of cases (operated feet) were satisfied with the overall result. The AOFAS hallux score improved at 12.9 years mainly in the pain and function parameters. In addition, there was significant correction of both the HV and IM angles. Only five patients (2.5%) had revision surgery as they were not satisfied with the overall result (four due to painful recurrence and one due to overcorrection of the deformity).
The upper limit of HV angle in which good results can be obtained has been previously shown to be 30 degrees ±5 degrees. 14,22 In addition, HV angles greater than 40 degrees have been reported to be associated with poor results. 5,14 The most common cause of failure of reduction of the HV angle is inadequate soft tissue rebalancing. 3,13 In our study there was no statistically significant difference in the HV angle correction in cases of preoperative HV angles greater than 40 degrees that had Mitchell's and lateral release compared with those that had no lateral release. These findings contradict the previously reported results. 5,14 In our experience, all hallux valgus deformities can be corrected if the Mitchell's osteotomy is performed in combination with lateral soft tissue release when soft tissue contraction prohibits HV angle correction during capsular repair, provided the first IM angle is not greater than 20 degrees.
Dorsal displacement and/or angulation of the capital fragment has been suggested to cause excessive shortening, leading to transfer metatarsalgia. 6,15 In order to prevent this, plantar displacement 2,6,8,17 and plantar angulation 15,23,24 have been proposed to reduce the amount of shortening. We used the percutaneous crossed Kirschner wire technique to achieve stability of the osteotomy. 10 This led to a mean shortening of the first metatarsal of 4.2 mm but none of our patients had more than 8 mm of metatarsal shortening. We believe that the small amount of shortening achieved in our study groups was probably due to our Kirschner wire fixation which provided better stability than other methods thus encouraging us to perform less bone removal. Also, this technique decreases the risk of dorsal displacement of the metatarsal head postoperatively while at the same time allows early joint mobilization to prevent stiffness. In addition we did not have an increase in lateral metatarsalgia which confirms the previously reported evidence of positive corelation of lateral metatarsalgia and excessive (greater than 10 mm) first ray shortening. 3,20,21
No change in the mean range of motion of the first MTP joint (combined plantar flexion and dorsiflexion) was found. In our experience, the first MTP joint motion tends to generally decrease during the early postoperative months compared to the preoperative condition. After approximately a year, we generally see an improvement that lasts for a number of years. Long-term range of motion deteriorates most likely due to degenerative changes affecting the first MTP joint. In view of the longer followup in our study group, this may explain this finding.
Under-correction and recurrence of the deformity are also recognized as common complications (about 10%) following this osteotomy. 2,4,23,24 We recorded three cases with under-correction, four patients with painful recurrence of the deformity and one case of over-correction. All patients had a preoperative HV angle more than 40 degrees. Most important, only the four patients with recurrence experienced significant pain. All eight patients were offered revision but the three patients with under-correction declined.
One patient developed avascular necrosis of the first metatarsal head, which can be attributed to vascular compromise related to surgery. The patient has so far been pain-free, with only minimal reduction in the MTP joint range of movement and has declined further surgery.
A limitation of this study is the preoperative AOFAS hallux score 12 was retrospectively calculated using the relevant information in the notes as documented by the surgeons before surgery. This particular clinical scoring system was used as it is used widely in the literature and is currently routinely used in our units. A large number of patients were reviewed and underwent surgery before the AOFAS hallux score was even published. It was not established in our units until 5 years ago.
Conclusion
This study has shown satisfactory long term results in a large number of patients who underwent Mitchell's osteotomy. It has also demonstrated that Mitchell's osteotomy with lateral soft tissue release can be successfully performed for HV angles greater than 40 degrees and IMA of up to 20 degrees. When performed properly with accurate surgical technique and stable fixation, a successful outcome with few complications can be achieved. We believe that this procedure is still useful in the treatment of hallux valgus.