
Abstract
Background:
The cause of navicular tuberosity pain in adolescents with flexible flatfeet is not well understood. We hypothesized that some of the navicular tuberosity pain may be related to insertional enthesopathy of the posterior tibial tendon at the navicular. Magnetic resonance imaging was performed to look for abnormal signal changes in a series of patients.
Material and Method:
Consecutive adolescent patients presenting with flexible flatfeet and navicular tuberosity pain were prospectively recruited. A detailed foot examination and body fat analysis was performed. Standing radiographs and Tekscan pedobarograph of both feet were obtained. Magnetic resonance examinations were performed on a 1.5-T whole-body magnetic resonance imaging system utilizing a standard extremity coil.
Results:
MRI abnormality was detected in 15 of the 36 feet in 18 adolescents examined. Abnormalities detected included thickening of the posterior tibial tendon insertion, marrow edema in the accessory navicular, marrow edema in the navicular tuberosity, and contrast enhancement at the posterior tibial tendon insertion site. Patients with MRI abnormalities were significantly taller, had a lower body mass index and a lower body fat percentage than those without MRI abnormality. Forward stepwise logistic regression analysis identified low body fat percentage and presence of an accessory navicular as independent predictors for abnormality on MRI.
Conclusion:
MRI abnormality was frequently detected in adolescents with painful flexible flatfeet. The MRI signal changes indicated an enthesopathy like process occurring at the posterior tibial tendon insertion to the navicular which could explain the origin of pain in flexible flatfeet patients without an accessory navicular. Early identification and appropriate treatment to prevent progression may be helpful.
Level of Evidence: IV, Case Series
INTRODUCTION
Flexible flatfoot, which is often a normal variant, is a very common condition in children and adults. The foot arch flattens upon weightbearing, but reappears upon nonweight-bearing, or with toe walking. Most of the children eventually develop an arch naturally with skeletal maturation. 22 For those older children and adolescents with persistent flexible flatfeet, the majority remain asymptomatic and have excellent foot function in adulthood. The need for any intervention for flexible flatfeet has been controversial, and the efficacy of any treatment debatable.
On the other hand, some adolescents with persistent flexible flatfeet develop symptomatic foot pain and poor tolerance to standing and walking. When the pain is localized to the navicular tuberosity, such pain is often ascribed to the presence of an accessory navicular bone and strain of the synchondrosis. 8,13,15 However, similar pain at the navicular tuberosity also occurs in adolescents with flexible flatfeet in the absence of an accessory navicular. In such cases, the cause of the pain is not well understood, and its treatment is uncertain.
We hypothesized that some of this navicular tuberosity pain is the result of an insertional enthesopathy of the posterior tibial tendon to navicular. The objective of this study was to evaluate whether navicular tuberosity pain in adolescents with flexible flatfoot was associated with signal changes in magnetic resonance imaging, compatible with posterior tibial tendon insertion enthesopathy. Patient characteristics that may be associated with abnormalities on MRI were also identified.
METHODOLOGY
Institutional ethics approval for the study was obtained. Consecutive adolescent patients attending the foot and ankle clinic presenting with painful flexible flatfeet and pain localized to the navicular tuberosity were prospectively recruited over a 12-month period. Written consent was obtained at the time of recruitment. Basic epidemiological data, pain and functional limitations were recorded. Diagnosis of flexible flatfoot was made on physical examination. A detailed foot and ankle examination was performed. With the patient standing, the feet were inspected for general morphology, the presence of a medial longitudinal arch and any heel valgus. With the patient sitting, the feet were carefully palpated to localize the site of tenderness. The ankle and subtalar joint ranges of motion were examined. Criteria used for diagnosis of flexible flatfeet were the absence of a medial longitudinal arch on standing, together with a positive toe-raising test. 11 Rigid flatfeet, polyarthropathy, and other arthropathy conditions were excluded. Presence of generalized hyperlaxity was defined as a Beighton score greater than four. 1 The patients were also asked to perform repetitive single leg heel rise as a test for posterior tibial tendon function. Standing anteroposterior, oblique and lateral radiographs of both feet were obtained. The anteroposterior and lateral talocalcaneal angles, anteroposterior and lateral talo-first-metatarsal angles, calcaneal pitch, and medial and lateral longitudinal arch indices were measured. The presence and the type of accessory navicular bone were noted. 7
A Tekscan HR portable pedobarograph (Tekscan Inc., South Boston, MA) with a sensor resolution of four sensors per square centimeter was used to record footprints. 5 After calibration with body weight, the subject stood on the pedobarograph with weight equally distributed between the two feet. Pressure recording at a sampling frequency of 50 Hz was taken for five seconds, during which the subjects remained stationary. One frame during the steady phase was randomly selected to calculate the Arch Index. 2 The length of the foot axis (base of second toe to center of the heel) excluding the toes was divided into three equal segments. Two perpendicular lines drawn at 1/3 and 2/3 of the foot axis length divided the foot print into three regions. The Arch Index was calculated as the area of the central region divided by area of the whole footprint. Normal Arch Index ranges from 0.21 to 0.26, with flat foot subjects having an Arch Index greater than 0.26. 2
Body fat percentage assay was measured using a Tanita 500 bio-impedance system (Tanita Corporation, Arlington Heights, IL), a lower body analyzer for measuring percentage body fat in healthy subjects with normal hydration. The subject stood barefoot on the footpads. A minute current at 50 KHz was applied to the anterior pressure contact electrode at the ball of the foot and received by the posterior electrode at the heel. The impedance to current flow was measured and used to estimate the body fat percentage based on a two-compartmental model of fat mass and lean body mass. 10,14
MR examinations were performed on a 1.5-T whole-body MR imaging system (Intera NT, Philips, Best, Netherlands) utilizing a standard extremity coil. Pulse sequences comprised T1-weighted (SE, TR/TE, 500/18, 3 mm slice thickness; 250 mm field of view, 512× 512 matrix) images in the axial, coronal and sagittal images along with T2-weighted short-tau-inversion-recovery (STIR) (1728/70, inversion time 150 msec, 3 mm slice thickness; 250 mm field of view, 256× 256 matrix) sequences in the axial plane. Axial T1-fat saturated images (20000/80, 3 mm slice thickness; 250 mm field of view, 256× 256 matrix) were also obtained prior to and following intravenous gadolinium. All axial images were acquired in a plane parallel to the tarsal bones while all sagittal images were acquired parallel to the first metatarsal bone.
Univariate analysis was performed with Mann Whitney U tests for continuous variables and chi-square tests for discrete variables. Parameters statistically significant on univariate analysis were entered into a logistic multivariate regression model with MRI abnormality as the dependent variable to identify independent predictive factors for abnormal MRI changes. All statistical tests were performed with SPSS 13.0 program (SPSS Inc, Chicago, IL). Differences were considered statistically significant at p < 0.05.
RESULTS
Twenty adolescents with flexible flatfeet complaining of pain localized to the navicular tuberosities were recruited. Two patients did not complete the MRI study and were excluded from analysis. There were 12 males and 6 females, with a mean age of 16.4 years (range, 13 to 19; SD 2.4). Pain onset averaged 77.2 minutes of level ground walking (range, 0 to 150 minutes; SD 49.7) and 39.3 minutes of running (range 0 to 90 minutes, S.D. 38.9 minutes). The diagnosis of bilateral flexible flatfeet was confirmed in all patients upon physical examinations. Heel valgus (mean 5.8 degrees; range 0 to 10; SD 2.9) was observed in 32 feet. All patients had tenderness localized to the posterior tibial tendon insertion to the navicular bone. The ankle and subtalar joint ranges of motion were all within normal limits. Nine patients had generalized laxity with Beighton scores over four. Six patients (8 feet) showed some difficulty in performing repetitive single leg heel rise.
XR showed features compatible with flatfeet. There was no tarsal coalition or other arthropathy detected. Accessory naviculars were found in 20 of the 36 feet, of which 9 were Type II, 11 were Type III. No Type I accessory navicular was identified.
MRI abnormality was detected in 15 of the 36 feet examined. MRI abnormalities detected included thickening of the posterior tibial tendon insertion in 16 feet, bone marrow edema in the accessory navicular or navicular tuberosity in 13 feet (Figures 1 and 2). There was no posterior tibial tendon intra-tendinous signal changes or peritendinous fluid detected. Contrast enhancement at the posterior tibial insertion site was found in 12 feet. There was no abnormal signal change detected in other parts of the feet.
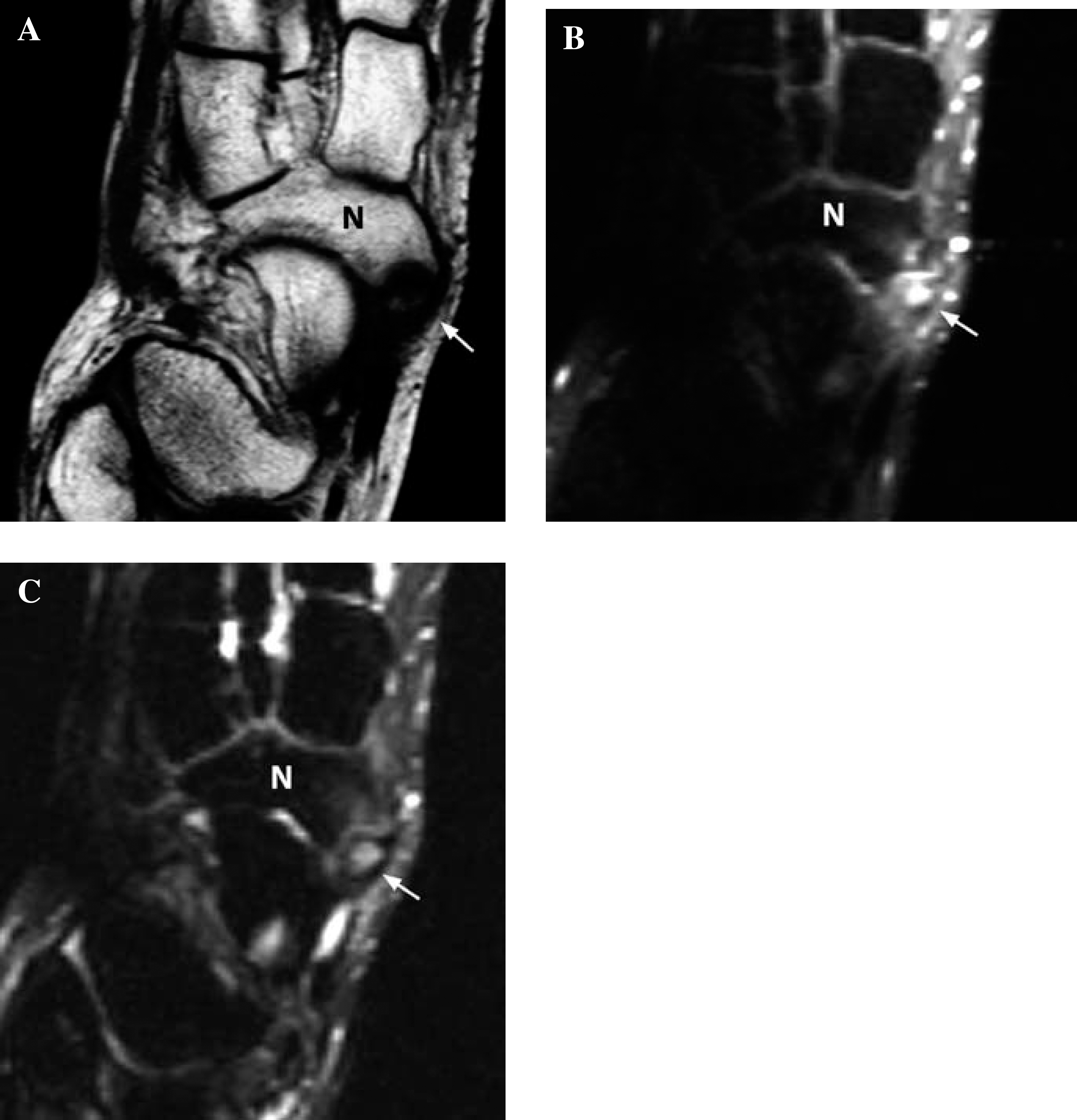
T1-weighted (A), T2-fat suppressed (B), and T1-fat-suppressed (C) images of right midfoot in an adolescent with painful flexible flatfoot. There is a Type II accessory navicular present. Medullary edema and hyperemia of this accessory navicular and the adjacent tuberosity of the navicular bone were detected (N) (arrows).
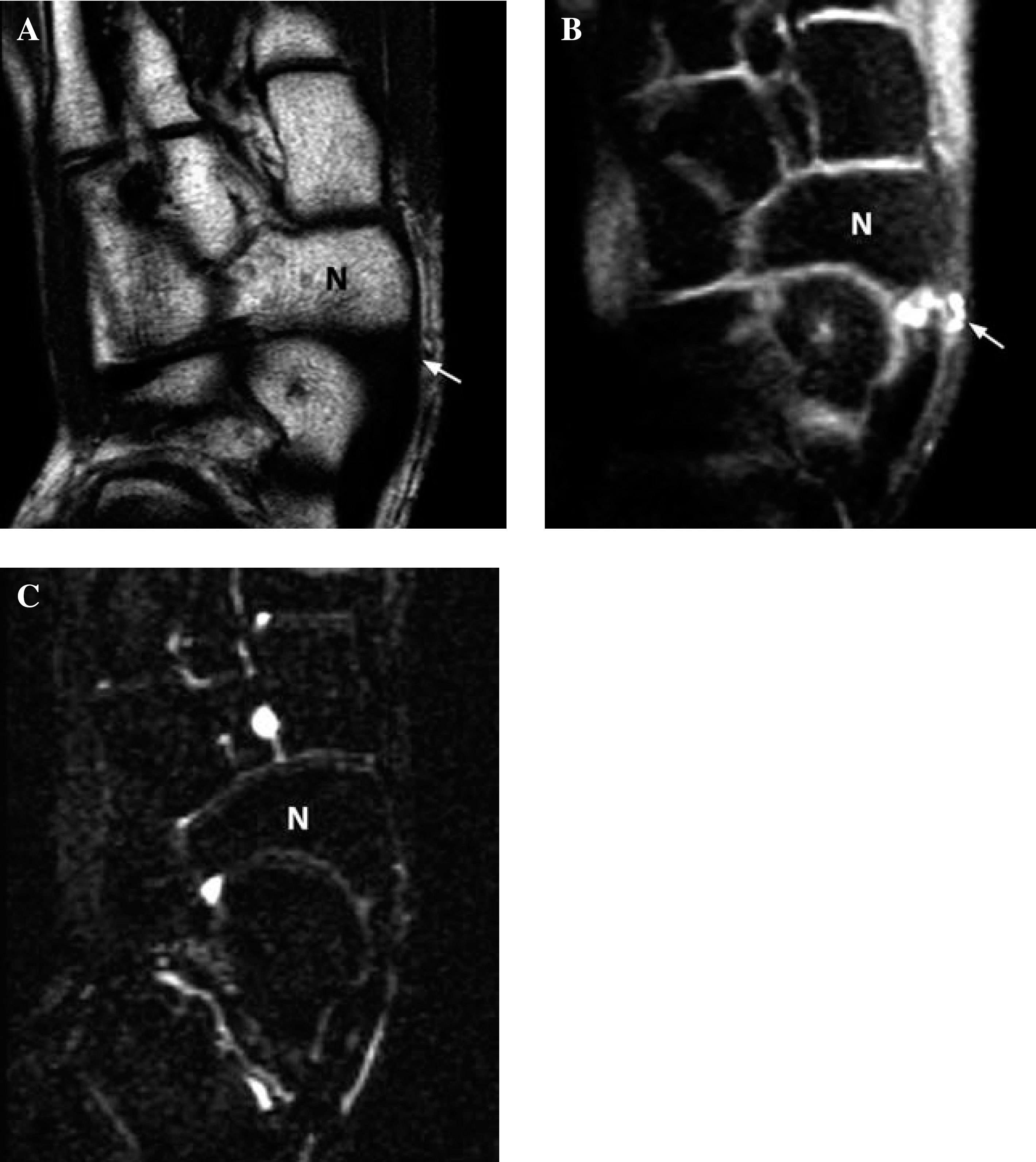
T1-weighted (A), T2-fat suppressed (B), and T1-fat-suppressed (C) images of right midfoot in an adolescent with painful flexible flatfoot. There is no accessory navicular present. Localized hyperemia of the posterior tibial tendon insertion (arrow) to the navicular (N) is present. No medullary edema is present.
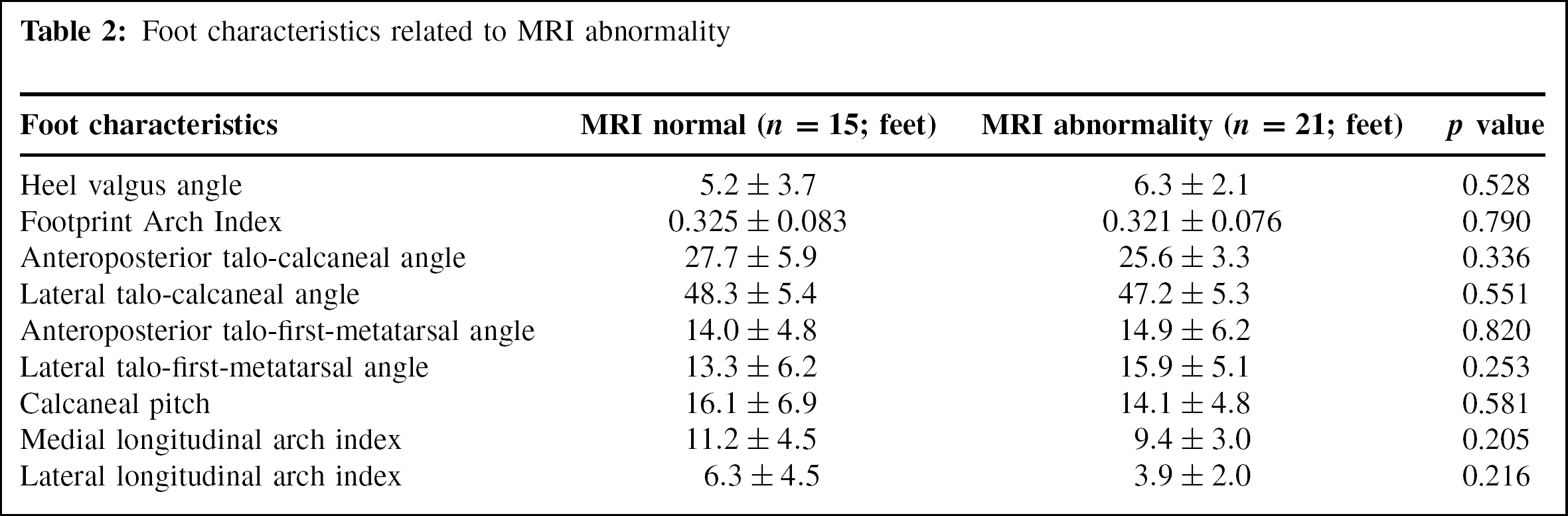
Patients with and without MRI abnormalities were comparable in terms of gender distribution, age and Beighton score. However, patients with MRI abnormalities were significantly taller (1.68 m v.s. 1.60 m, p = 0.045), and had a lower body mass index (21.6 kg/m 2 vs. 24.6 kg/m 2 , p = 0.051) than those without n MRI abnormality. Patients with MRI abnormality also had a significantly lower body fat percentage than those with a normal MRI (21.4% vs 31.5%, p = 0.013) (Table 1). Chi square test showed a significantly higher frequency of accessory navicular bones in feet with an MRI signal abnormality (p = 0.003). No significant difference was found in footprint Arch Index or any of the radiographic measurements between those with and without MRI abnormality (Table 2).
Patient characteristics related to MRI abnormality
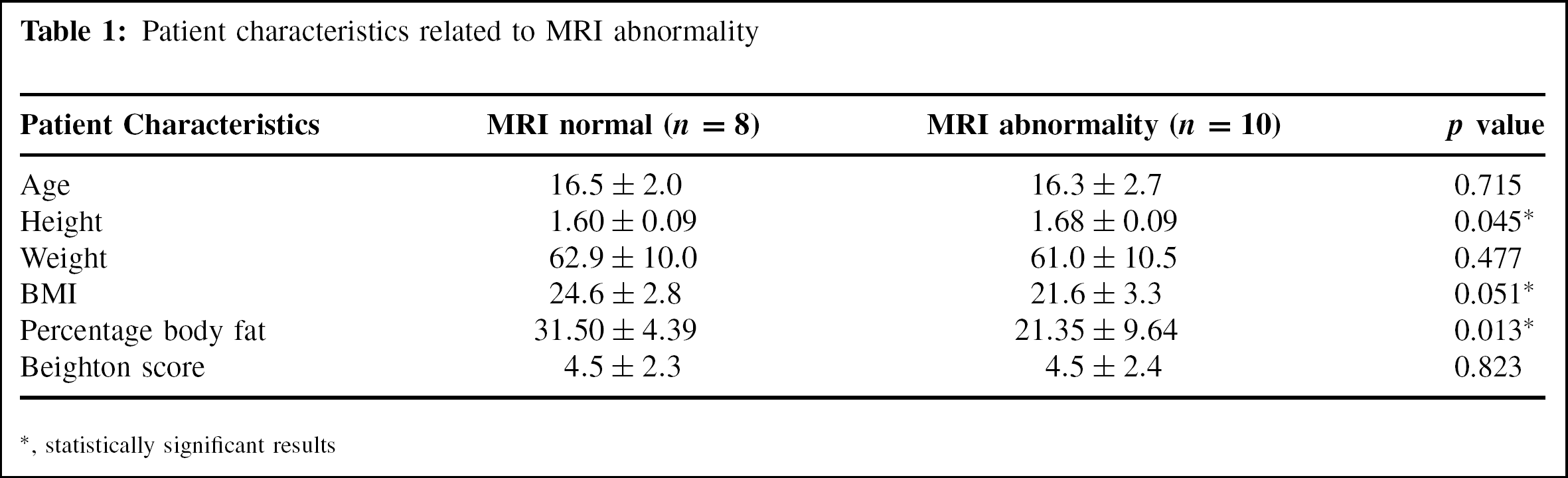
statistically significant results
Foot characteristics related to MRI abnormality
Forward stepwise logistic regression analysis identified body fat percentage as an independent negative predictor (p = 0.010, odds ratio 0.849, 95% CI 0.750 to 0.962) and an accessory navicular as an independent positive predictor (p = 0.012, odds ratio 11.321, 95% CI 1.722 to 74.415) for abnormality on MRI examination.
DISCUSSION
Flexible flatfoot is a very common condition in both children and adults. Most people with flexible flatfeet have no foot pain and excellent foot function. These people do not require any intervention. However, in the group who do develop symptoms, the cause of pain is not always clear. The form and effectiveness of treatment is also controversial. There is often both a lack of explanation for the patient's symptoms and a lack of objective criteria to guide patient treatment.
Medial arch pain in children with flexible flatfeet is often ascribed to the presence of an accessory navicular. The compressive force along the medial longitudinal arch together with chronic tension and shear force by the posterior tibial tendon in patients with flatfeet and excessive pronation is thought to lead to accessory navicular synchondrosis pain. 20 Type II accessory navicular is most commonly associated with symptoms. 8,20 However, the association between an accessory navicular and flexible flatfoot symptom is not clear. An accessory navicular is found in up to 16% of asymptomatic subjects, 19 and many patients with painful accessory navicular have normal foot arches. 8 The current study shows that the disease process is not confined to the accessory navicular synchondrosis. MRI abnormality was also frequently apparent in the posterior tibial tendon insertion and navicular tuberosity. These changes were detected in patients with and without an accessory navicular. Patients with MRI abnormality were more likely to be taller, have relatively less body fat and more likely to have an accessory navicular than those without MRI abnormality. While the absence of any Type I accessory navicular in the current series may be incidental, it may also reflect a low propensity of Type I accessory naviculars to cause pain.
Previous investigators have used technetium bone scintigraphy and MRI to identify the cause of pain in symptomatic Type II accessory naviculars. 4,18,21 As only Type II accessory naviculars were studied, abnormal changes were found to center at the synchondrosis. The current study recruited consecutive flexible flatfeet adolescent patients with navicular pain, irrespective of whether an accessory navicular was present or not. A more diffuse pattern of involvement was found. The posterior tibial tendon insertion site and navicular tuberosities also frequently manifested abnormalities. This helps to explain the origin of pain in flexible flatfeet patients without accessory naviculars. The overall disease pattern was similar to that seen in enthesopathy.
The posterior tibial tendon is the most powerful invertor of the foot. Posterior tibial tendon contraction initiates hindfoot inversion at heel rise, thereby stabilizing the talonavicular and calcaneocuboid joints to maintain the medial longitudinal arch. 17 Posterior tibial tendon dysfunction leads to the loss of this locking mechanism, resulting in acquired flatfoot in adults. 6,12,16 The tendon pathology ranges from tenosynovitis, degenerative tendinosis, longitudinal tear, tendon attenuation to complete rupture. Though most of the cases occur in middle aged obese adults with degenerative tendinopathy, 9 other conditions leading to functional deficiency of the posterior tibial tendon have been reported to result in progressive flatfoot. 3
The MRI signal changes detected in the current series indicated an enthesopathy-like process occurring at the posterior tibial tendon insertion to the navicular. Enthesopathy at the posterior tibial tendon insertion may lead to functional insufficiency of the posterior tibial contraction similar to posterior tibial tendon dysfunction. Though these patients have had flexible flatfoot since childhood, the superimposed enthesopathy can lead to persistent pain, progression of the flatfoot and further functional deterioration. We believe early identification and appropriate treatment to prevent progression is therefore imperative.
Ultrasonography is useful in differentiating accessory navicular synchondrosis separation from posterior tibial tendon attenuation and rupture. 3 However, ultrasonography does not show bone pathology well. MRI has the advantage of allowing better anatomical delineation with simultaneous assessment of both bone and adjacent soft tissues. As most of the abnormality detected in these flexible flatfoot patients was located in the enthesis, these changes were better defined with MRI. Fluid sensitive fat-suppressed sequences in particular allowed better visualization of bone marrow edema than conventional T2-weighted spin echo sequences. 18
CONCLUSION
MR abnormalities in terms of thickening of posterior tibial tendon insertion, contrast enhancement and marrow edema were demonstrable in a high proportion of adolescent flexible flatfoot subjects with navicular pain. The enthesopathy-like condition may lead to functional deficiency of the posterior tibial tendon. Recognition of the pathological process may help to guide early treatment and prevent deterioration.