
Abstract

INTRODUCTION
Ankle arthrodesis with internal screw fixation is biomechanically sound with proven results 3,6 and fewer complications than other techniques. 5 Solid screw use has been criticized as technically challenging, dissuading many surgeons despite considerable cost savings. We present a simple and reproducible technique of ankle arthrodesis using solid screw fixation with review of 14 consecutive cases using this method.
OPERATIVE TECHNIQUE
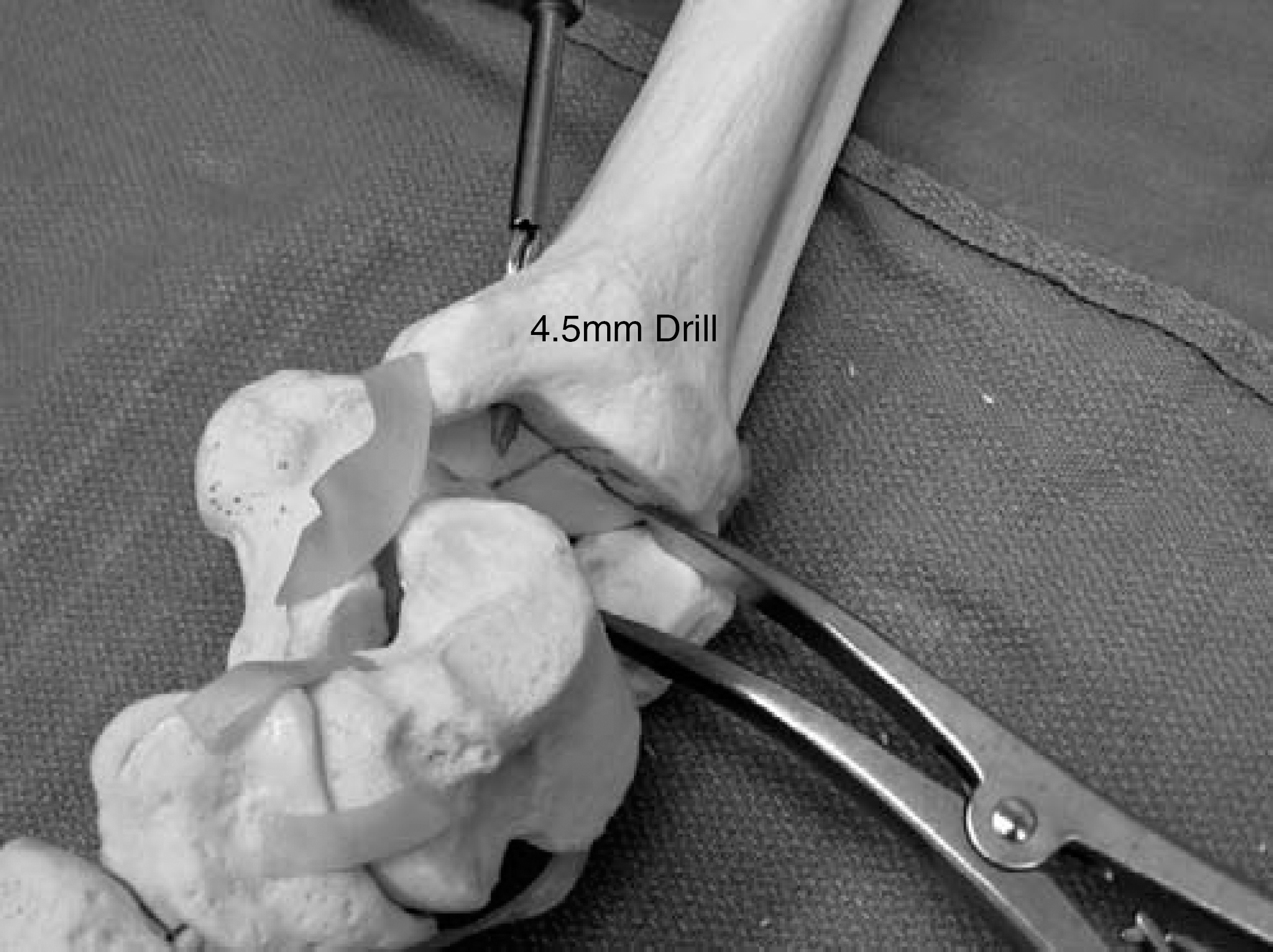
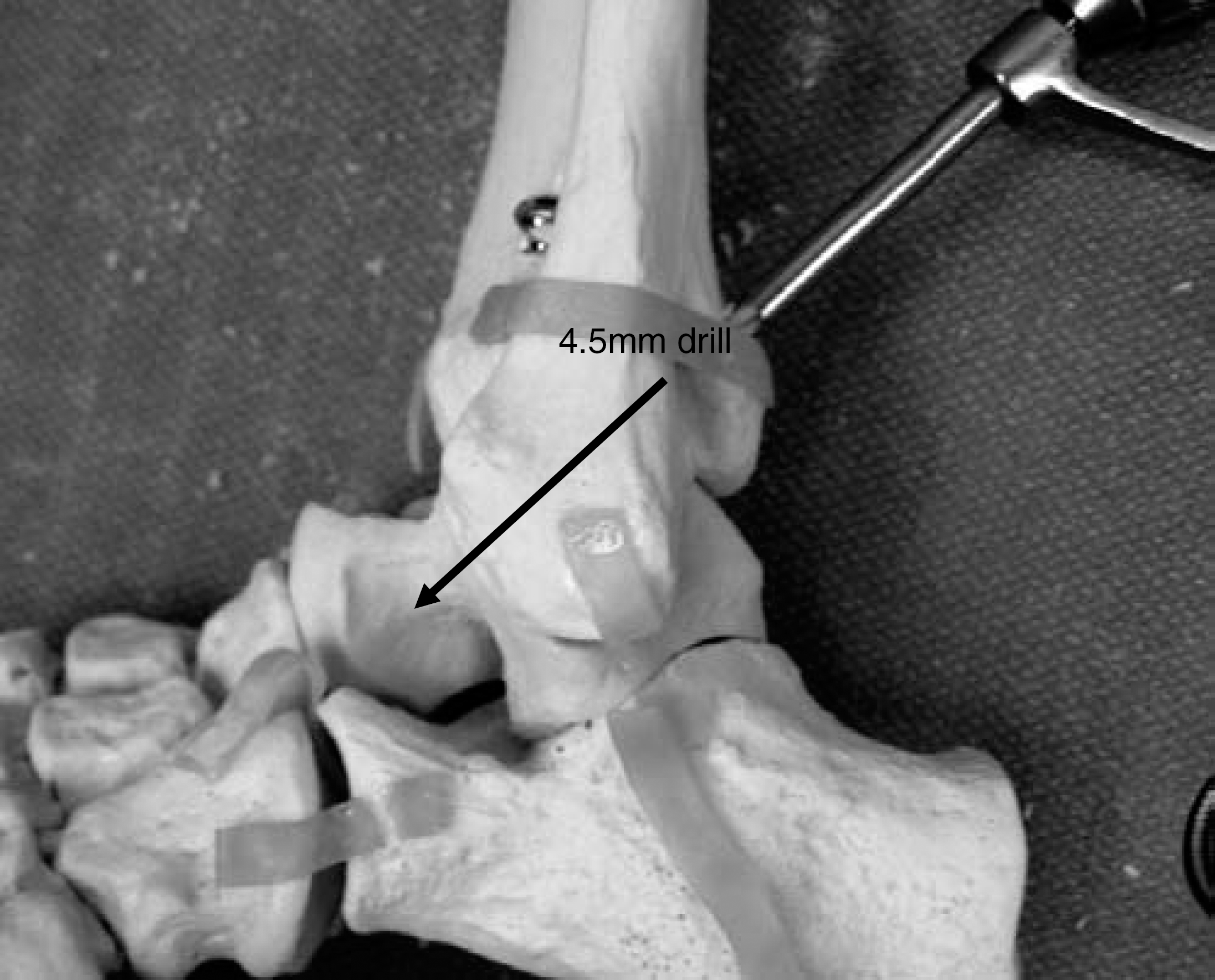
In a supine position supported by bump or beanbag allowing adequate lateral exposure, an extensile lateral approach is made. We expose, osteotomize, and retract the distal fibula in a standard fashion, ensuring the joint surfaces are prepared for fusion in customary way with meticulous debridement of all remaining articular cartilage and disruption of subchondral bone by drilling. Fixation is obtained by three solid 16-mm partially threaded 6.5-mm screws: medial, lateral and posterior. 3 The talus is appropriately positioned under the tibial plafond. 4 The articular surface of the tibial plafond is divided into 4 quadrants (Figure 1). The tibial portion of the lateral screw is drilled, visualizing the 4.5-mm drill exiting in the antero-lateral quadrant (Figure 2). The depth is measured and 20 mm is added for final screw length. Next, the medial tibial screw is drilled through a standard percutaneous approach, visualizing the exiting 4.5-mm drill bisecting the antero-medial and postero-medial quadrant (Figure 3). Again, the tibial portion is measured and 20 mm is added to this length. The talus is reduced into the plafond and held with Kirschner wires. A 3.2-mm pilot hole is drilled into the talus over the centering sleeve with standard AO technique (Figure 4). The lateral and medial screws are inserted. By adding 20 mm to the tibial length, the 16-mm threads are ensured to pass into the talus and provide compression. Additionally, all threads will be in the talus and this technique ensures that the subtalar joint is not penetrated by excessive screw length. The talus is now stable on the tibia and the final posterior screw can be placed. Through the extensile lateral incision posterior to the peroneal tendons or through a percutaneous approach, a 4.5-mm drill is placed on the posterior tibia proximal to the metaphyseal flare. The dorsal cortex of the talar neck is visualized and the drill is aimed slightly plantar (55 to 65 degrees) 3,6 and toward the medial column. A solid 6.5-mm screw, typically 55 mm in length, is inserted (Figure 5). Acceptable position of internal fixation by plain radiography or by fluoroscopy is confirmed (Figure 6). The fibula is secured to the tibia and talus with 3.5-mm compression screws and bone grafted as indicated. The wound is closed in layers.
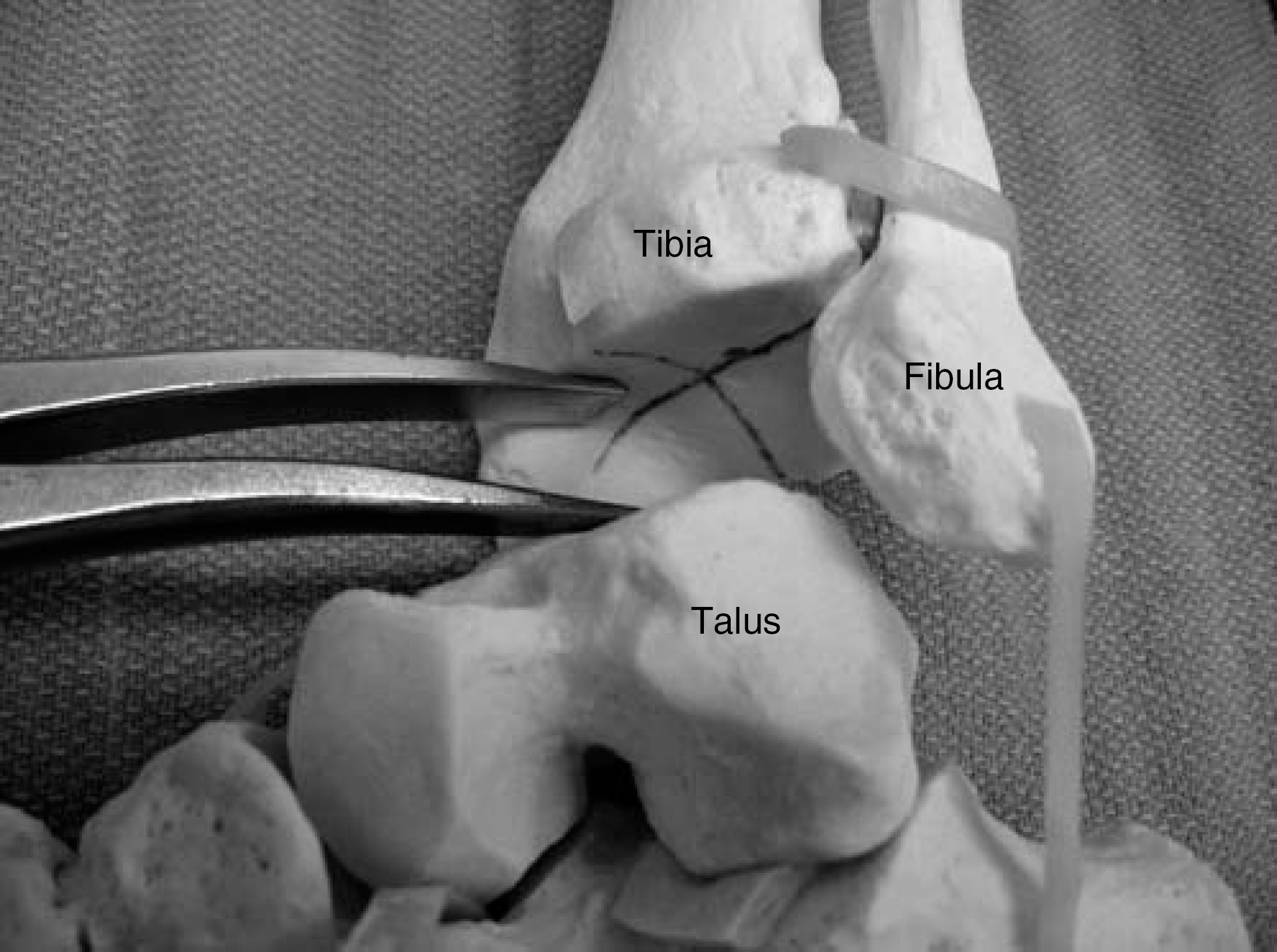
Model of tibial plafond divided into 4 quadrants.

4.5-mm drill exiting the antero-lateral quadrant.
4.5-mm drill placement for the medial screw.

3.2-mm drill over centering sleeve prior to medial screw insertion.
Placement of the posterior screw.
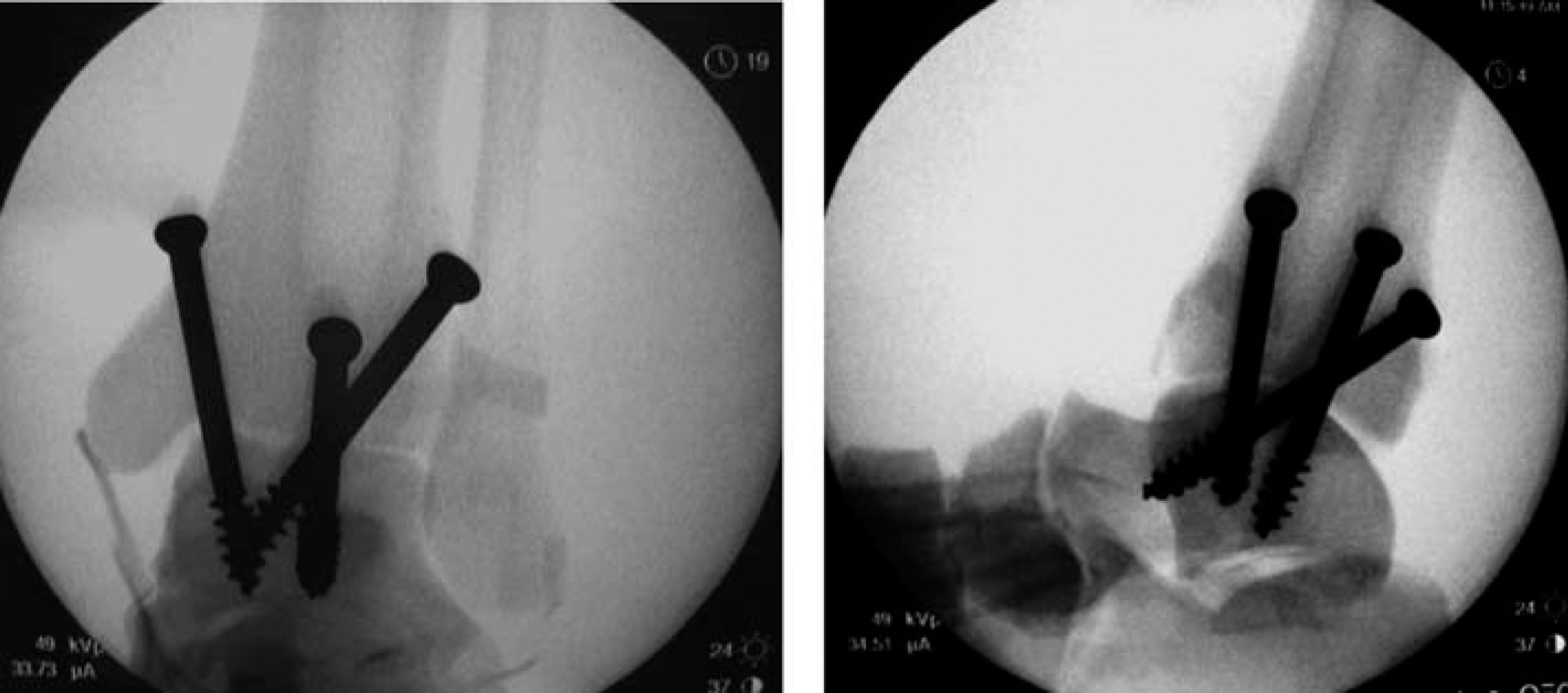
Flouroscopic confirmation of acceptable screw placement.
DISCUSSION
Ankle arthrodesis is a preferred method of treatment for advanced arthritis of the ankle that fails non surgical management. All methods require meticulous technique, careful joint preparation and attention to positioning. We offer a technique tip to simplify an important and often technically challenging aspect of the procedure: placing internal fixation reliably in order to standardize screw position and allow correct choice of screw length.
Initial rigidity of the ankle arthrodesis is related to the position and the mechanical properties of the internal fixation, in addition to the density of the bone into which the screw is inserted. 1 Because of the perceived technical challenges of solid screw fixation, cannulated screws have become popular. The mechanical properties of the fixation device are an important consideration. These properties include pullout strength, compressive force, ultimate bending moment and fatigue strength. 1,2,7 In an idealized computer model, the mechanical properties of cannulated screws theoretically mimic those of solid screws. 2 There is a potential that cannulated screws are weaker in less dense bone due to a larger root diameter required to accommodate the central cannulation 1 and this effect may be greater if short thread cancellous screws are used. 7 However, even if cannulated screws can offer the same initial fixation rigidity and strength, the undeniable disadvantage is cost. In 14 consecutive cases performed at an outpatient center utilizing this technique, the implant cost for all cases was less than one ankle arthrodesis using cannulated screws. No screws in our review were discarded due to improper length.
Any technique that can minimize radiation exposure can also be advantageous. This technique allows screw length and position to be reliably predicted, resulting in decreased fluoroscopic and surgical time as well. In our cases the mean tourniquet time from incision to splint application was 80 minutes. These cases were in a teaching setting with orthopaedic residents participating with a range of diagnoses from post traumatic to adult acquired flatfoot deformity with tilted ankle arthritis requiring deformity correction (Figures 7 to 10).

Pre-op standing AP ankle radiograph showing tilted ankle arthritis due to advanced adult acquired flatfoot deformity.

Pre-op standing lateral radiograph showing advanced adult acquired flatfoot deformity, negative medial cuneiform height, no calcaneal pitch and a plantarflexed talus.

Post-op standing oblique ankle after arthrodesis, medial lateral and posterior screws. Fibula is fixed with two 3.5-mm screws.

Post-op standing lateral foot radiograph after ankle arthrodesis showing corrected foot position. Proper talar positioning is crucial as foot position follows talar position. A tendo-achilles lengthening in conjunction with arthrodesis allows foot deformity correction through coupled subtalar joint motion. Successful arthrodesis maintains this correction.
Our protocol for ankle arthrodesis involved an outpatient procedure when medically appropriate. General anesthesia with pre-operative popliteal block was also universally utilized. A bulky post operative splint was applied for 2 weeks, followed by short leg nonweightbearing cast for 4 to 6 weeks. Gradual weightbearing over the next 4 weeks in a fracture boot with rocker bottom was then allowed. Patients were encouraged to return to comfortable footwear after 3 months, assuming radiographs confirmed healing.
Ankle arthrodesis can be a challenging procedure and surgeons should utilize techniques they are most comfortable performing. We offer a simple method to facilitate a critical but often time consuming and technically demanding portion of this procedure. This can result in decreased operative time and minimize implant costs which is particularly important in an outpatient surgery setting.