
Abstract
Background: The shallow malleolar groove of the fibula is believed to be one of the important causes of dislocation of the peroneal tendons. However, no studies have investigated the morphological differences between patients with and without dislocation of the peroneal tendons. Materials and Methods: We investigated the morphological variations (concave, flat, or convex) of the malleolar groove of the fibula using magnetic resonance imaging (MRI) in 39 ankles from 36 patients with recurrent dislocation of the peroneal tendons, comparing them with 39 ankles in 39 patients without dislocation. We also evaluated the presence of the false pouch on the fibula surface and fibrocartilaginous ridge injury of the malleolar groove on MRI. Chi-square test was used for statistical analysis between the two groups. Results: MRI at 1 cm proximal from the tip of the fibula demonstrated that the malleolar grooves in patients with dislocation of the peroneal tendon were classified as concave in 4 patients, flat in 23, and convex in 12, whereas they were classified as concave in 6, flat in 22 and convex in 11 in the patients without dislocation of the peroneal tendons. No significant difference could be detected between the two groups. Conclusion: This study demonstrated that no significant difference could be detected in the morphological shape of the fibular malleolar groove between patients with and without dislocation of the peroneal tendons.
Introduction
Although dislocation of the peroneal tendons is not a common disease, it is recognized as one of the main causes of lateral ankle pain and instability.6,11,13 If it does occur, daily or sports activities can be severely restricted, especially for young athletes. 1 The pathogenesis of dislocation of the peroneal tendons is often attributed to congenital dislocation of the peroneal tendons, acute trauma, or a shallow fibular malleolar groove, but none of these suggested contributors has been well investigated.6,11,13
A shallow fibular malleolar groove is believed to be one of the important contributing causes of dislocation of the peroneal tendons. However, previous studies have only investigated either normal subjects or patients with dislocation of the peroneal tendons.4,5,10 No report has investigated the morphologic variations of the malleolar groove of patients with this pathology compared to normal subjects.
A recent anatomical study demonstrated that the shape of the malleolar groove was determined by a thick cartilaginous ridge that covered the convex bone surface. 10 Ogawa and Thordarson 13 stated that this fibrocartilaginous ridge is loosely connected with the periosteum and does not provide a strong attachment for the superior peroneal retinaculum, which blends with the periosteum of the lateral aspect of the malleolus. Thus the ridge usually remains on the fibula while the retinaculum strips the periosteum from the fibula causing a false pouch. Although the fibrocartilaginous ridge and the false pouch may play important roles in the development and/or resolution of dislocation of the peroneal tendons, few studies have investigated the morphological variations of the malleolar groove of the fibula. We believe that it is very important to investigate the morphological variations of the fibular malleolar groove in those with and without peroneal tendon dislocation, when considering the pathogenesis or treatment of dislocation of the peroneal tendons.
The purpose of this study was to investigate the morphological variation of the fibular malleolar groove in those with and without peroneal tendon dislocation using MRI. We hypothesized that there would be no difference in the morphological shape of the fibular malleolar groove between patients with and without dislocation of the peroneal tendons.
Materials and Methods
The ethical review board for human research subjects at our institution approved the use of human subjects for this research. Before performing this study, written informed consent was obtained from all patients.
Between January 2000 and September 2008, we performed a superior retinacular repair on 40 patients with symptomatic dislocation of the peroneal tendons who had failed to respond to at least 3 months of conservative treatment, including modifications of sports activities, bracing, or anti-inflammatory medications. Thirty-six patients whose preoperative MRI was available for evaluation of morphologic shape of the malleolar groove were included in this study. Because three patients underwent bilateral surgery, a total of 39 ankles were evaluated, comprising 26 males and 10 females with an average age of 23.2 (range, 11 to 59) years at the time of surgery. No patient showed lateral ankle instability or hindfoot malalignment. In 31 patients, dislocation of the peroneal tendons occurred in sports activities. In two patients, the first dislocation occurred when they sprained their ankle while walking. The other three patients had their first dislocation in a traffic or work accident. All 36 patients reported a preceding trauma. It was apparent that none were caused by congenital anomalies or variations. All patients had complained of painful dislocation of the peroneal tendons while either playing sports or carrying out their daily activities with their ankle in dorsiflexion. The average preoperative interval from first dislocation to operation was 9.8 ± 8.7 (range, 3 to 37) months.
The control group included 39 patients who underwent MRI examination of their ankle for reasons other than peroneal tendon pathology such as lateral ankle instability or osteochondral lesions of the talus. None of them experienced dislocation of the peroneal tendons. There were no significant gender or age differences between the groups.
The MRI examination was performed with a 1.5-T super-conducting MR unit (Hitachi Medical Corp., Tokyo, Japan), using a transmit-receive coil. The patients were imaged in a supine position with the ankle in 20 degrees plantarflexion in accordance to a standard protocol. The MRI protocol consisted of transverse T1-weighted spin echo (TR/TE: 350/20), and T2-weighted fast spin-echo (TR/TE: 3650/110) sequences. The field of view was 10 cm. The slice thickness was 3 mm with an interslice gap of 1 mm. The image matrix was 256 × 256 pixels.
We evaluated the MRI at the level of the tibial plafond and at 1 cm proximal from the distal end of the fibula. The MRI was retrospectively reviewed by two orthopaedic specialists (T. K., T. N.) who had no access to patients'information. They had at least 3 years of experience in reading MRI under the guidance of radiologists. The appearance of the malleolar groove was defined as convex when the posterior cortex of the fibula bulged outward, concave when the posterior fibular surface had a shallow-to-deep depression, and flat when neither concavity or convexity was found according to Rosenberg et al. (Figure 1). 16 If two examiners disagreed with the appearance of the malleolar groove, they reached a consensus while viewing the MR together. We also evaluated the presence of a false pouch over the fibula and injury of the fibrocartilaginous ridge of the malleolar groove on the MRI. The false pouch on the MRI was defined as a high intensity area in T2-weighted images over the lateral malleolus. The fibrocartilaginous ridge on the MRI was defined as the triangular cartilaginous area at the posterolateral edge of the lateral malleolus. We performed a superior retinacular repair for all patients with dislocation of the peroneal tendons. In this repair, the false pouch was opened at the anterior attachment of the detached periosteum and retinaculum. The retinaculum was advanced to the lateral aspect of the peroneal groove through drill holes. 1 The presence of a false pouch and fibrocartilaginous ridge was evaluated intraoperatively.
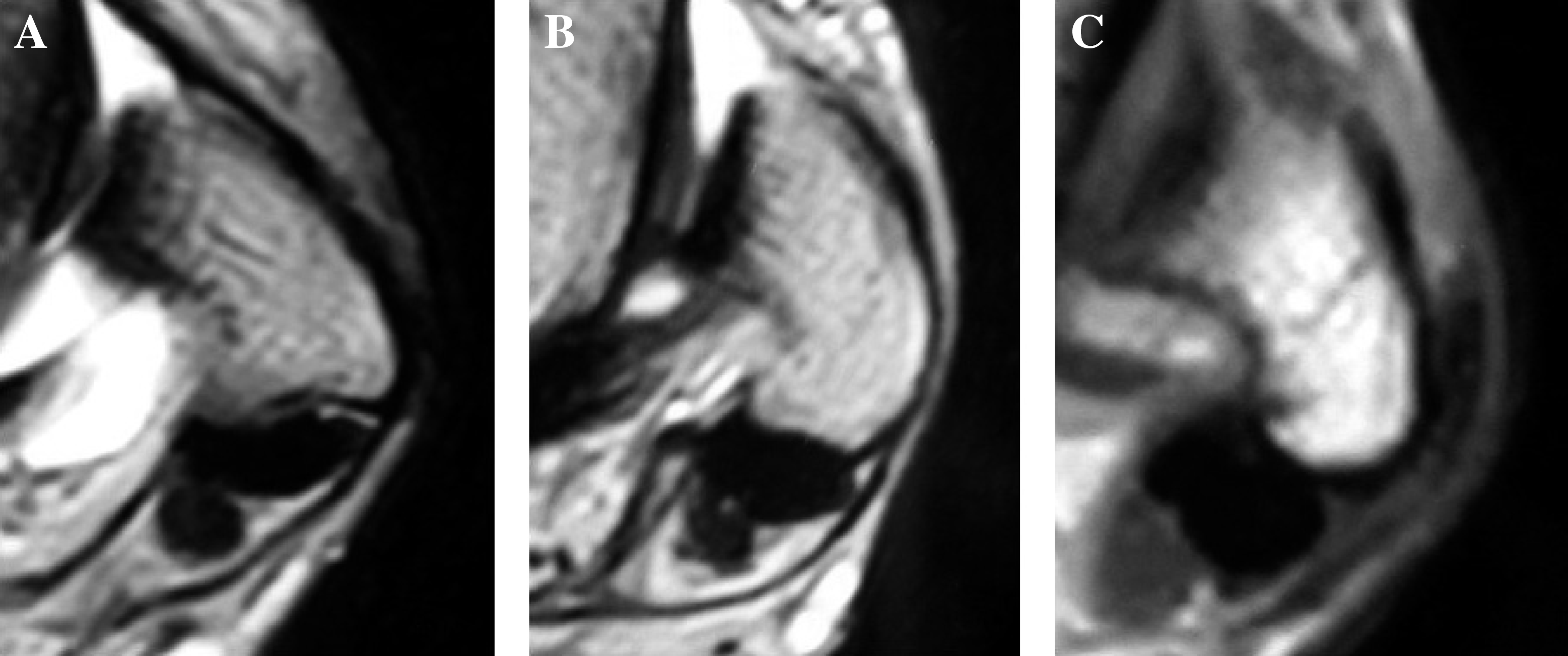
MRI findings of the malleolar groove. The appearance of the malleolar groove was classified as “concave” (A), “flat” (B), and “convex” (C).
Statistical analysis
The chi-square test for independence was used for comparative evaluation of the malleolar groove's appearance in the two groups. A p value less than 0.05 was regarded as statistically significant. All statistical analyses were conducted on Statview 5.0® (SAS Institute, Cary, NC).
Results
MRI at the level of the tibial plafond demonstrated that all malleolar grooves were classified as convex in patients with and without dislocation of the peroneal tendons. The two examiners agreed on all of these images
For the MRI at 1 cm proximal to the tip of the fibula, the two examiners were in agreement on 72 of 78 ankles (92%) at their first evaluation. In the other six cases, agreement was reached after a discussion reviewing the films together. The malleolar grooves in patients with dislocation of the peroneal tendon were classified as concave in 4 ankles, flat in 23, and convex in 12, whereas they were concave in 6, flat in 22 and convex in 11 in patients without dislocation of the peroneal tendons. No significant difference could be detected between the two groups (p = 0.687).
The false pouch on the fibula surface was recognized in only 26 of 39 ankles with dislocation of the peroneal tendons on the MRI (Figure 2). The injury of the fibrocartilaginous ridge of the malleolar groove was also demonstrated in 7 of 39 ankles with dislocation of the peroneal tendons on the MRI (Figure 3). Intraoperative evaluations revealed that all patients with dislocation of the peroneal tendons had a false pouch over the distal end of the fibula. Fibrocartilaginous ridge injuries of the malleolar groove were also demonstrated intraoperatively in 12 ankles including those with positive MRI findings. Therefore, accuracy rates for MRI detection were 67% (26/39) for a false pouch and 58% (7/12) for fibrocartilaginous ridge injury.
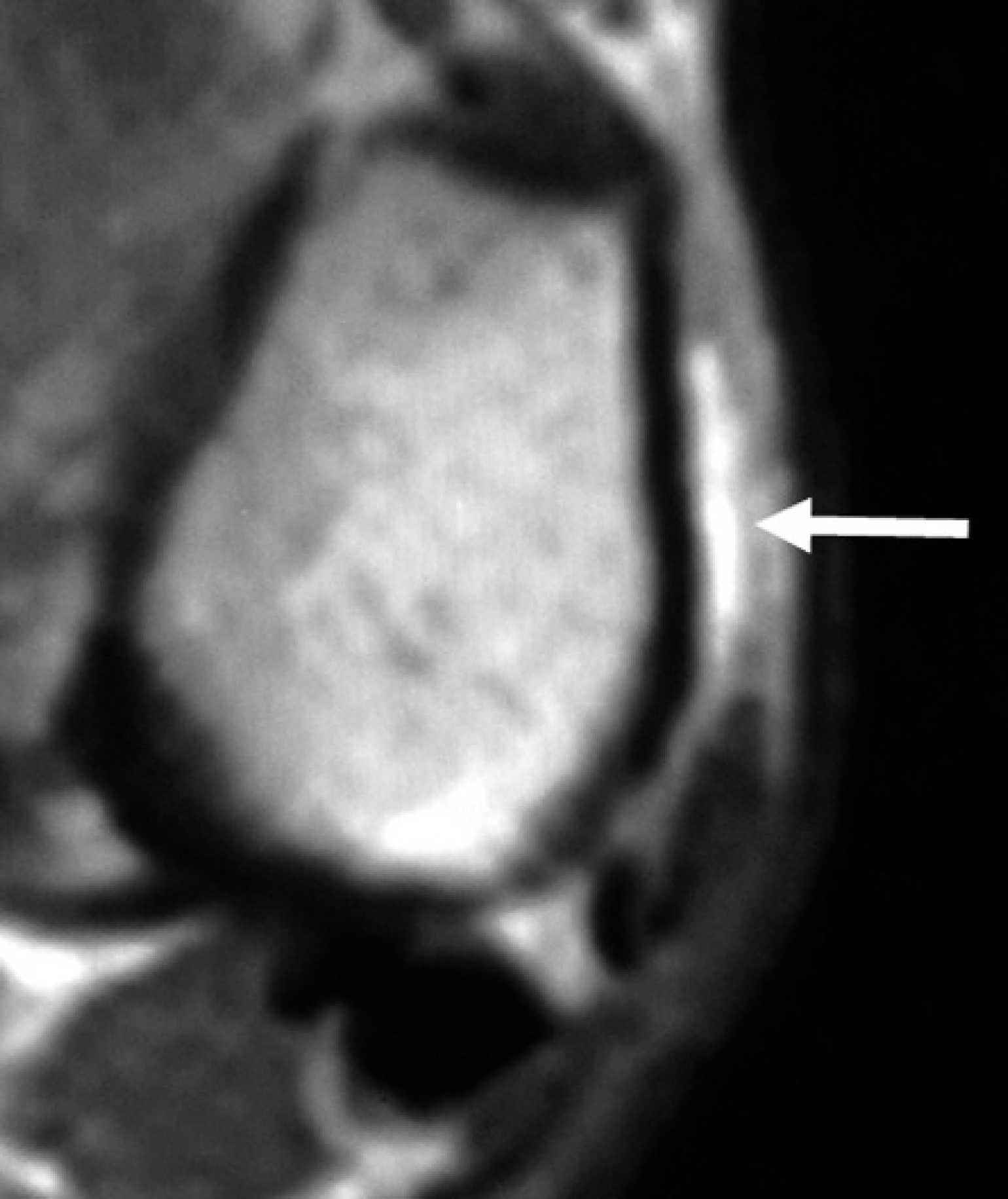
The false pouch (white arrow) on the fibula on MRI.
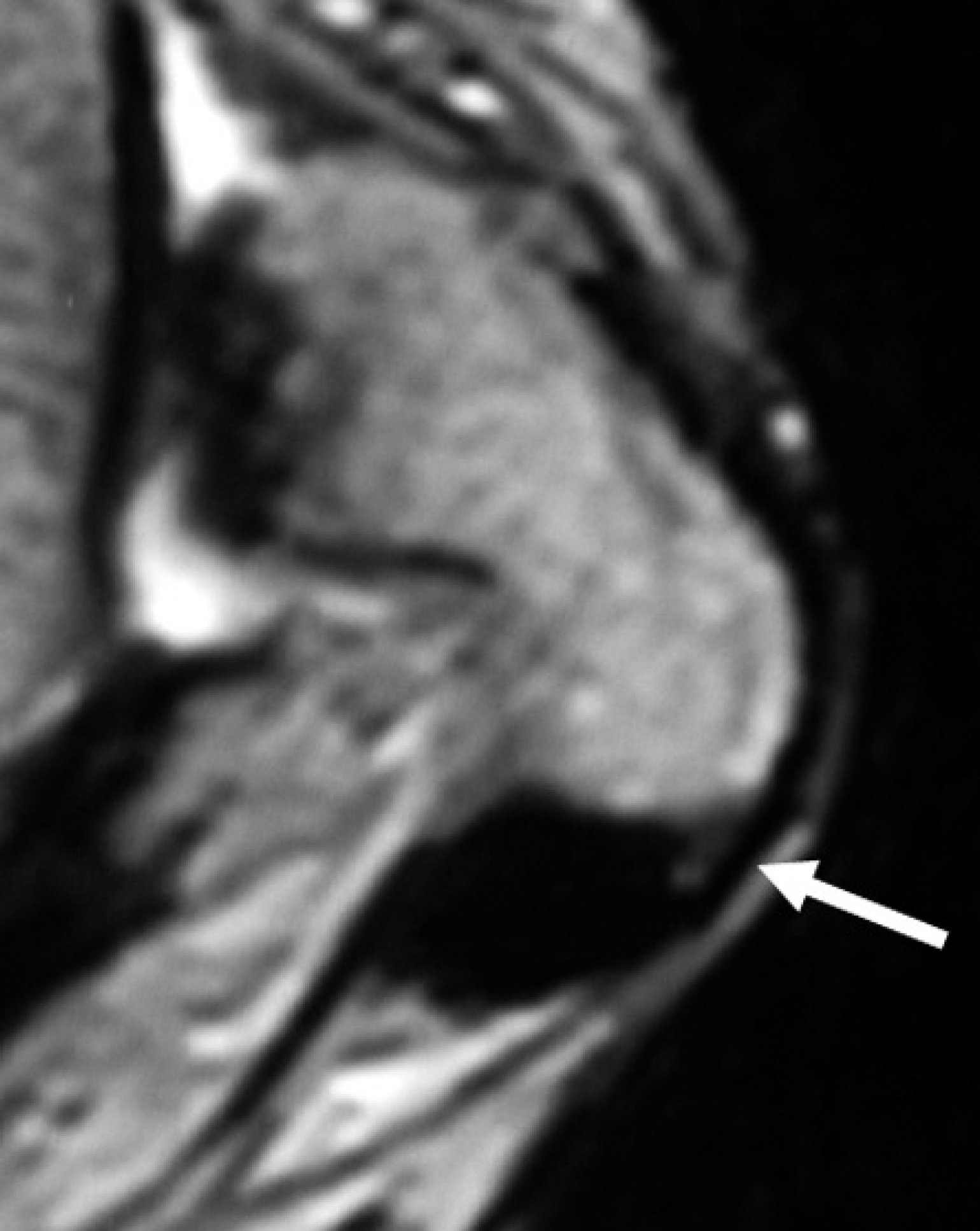
MRI detects the fibrocartilaginous ridge (white arrow) of the malleolar groove.
There were no false positive findings on MRI for either the false pouch or injury of the fibrocartilaginous ridge of the malleolar groove in patients without dislocation.
Discussion
This current study investigated the morphological variations of the fibular malleolar groove using MRI in patients with or without dislocation of the peroneal tendons. We demonstrated that no significant difference was detected in the morphological variation between the groups. Regardless of whether the patients had peroneal tendon dislocation or not, many bony malleolar grooves were essentially flat and were reinforced by the fibrocartilaginous ridge. This ridge may play an important role in preventing dislocation of the peroneal tendons which other authors have also suggested,4,10 although the intraoperative incidence of the fibrocartilaginous ridge injury was 31% (12/39) in this study. Therefore, we have to pay considerable attention to fibrocartilaginous ridge injuries of the malleolar groove intraoperatively, especially for patients whose injury was not detected on preoperative MRI. However, because accuracy for detecting fibrocartilaginous ridge injury on MRI is not high (58%), we have to evaluate these injuries carefully intraoperatively. It is also important to note that the false pouch was observed in all patients with dislocation of the peroneal tendons. While we believe that false pouch is a result of the tendon dislocation, it likely plays an important role for persistence of this pathology.
Dislocation of the peroneal tendon is one of the causes of ankle pain and instability that can hinder daily or sports activities, especially in young patients. The pathogenesis of dislocation of the peroneal tendons is often attributed to congenital dislocation of the peroneal tendons, acute trauma, and/or a shallow fibular malleolar groove.6,11,13 Hindfoot malalignment also may contribute to dislocation of the peroneal tendons. The presence of an accessory peroneus quartus muscle may cause stenosis of the malleolar groove, thereby increasing the risk of dislocation of the peroneal tendons. 6
After Edwards 5 reported a gross anatomic study using dry bone to investigate variations in the malleolar groove of the fibula, there have been several other reports that describe the shape of the fibular malleolar groove.4,10,16 However, no report has compared the morphological difference between patients with and without dislocations. Considering that morphological variations in the malleolar groove did not appear to be significantly different between the two groups, the fibrocartilaginous ridge may play an important role for preventing dislocation of the tendons. In 1976, Eckert and Davis 4 described the pathological anatomy and the results of operative repair of the superior peroneal retinaculum in patients with dislocation of the peroneal tendons. They found the cartilaginous ridge to be elevated along with the retinaculum and periosteum in 33% of their patients. Kumai and Benjamin 10 investigated the histological structure of the fibular malleolar groove and found that distally the bone was convex and the shape of the groove was determined by a thick periosteal cushion of fibrocartilage that covered the bone surface.
There have been many operative procedures described for recurrent dislocation of the peroneal tendons, including anatomical reattachment of the retinaculum,1,2,7 bone block procedures,3,9,18 tissue transfer procedures,12,14,15,17 or groove-deepening.8,19 Each procedure has its advantages or disadvantages. In order to perform tissue transfer procedures, the sacrifice of normal important structures is inevitable. For bone block procedures, we need to use internal fixation which may require a second operation for its removal. The groove-deepening operation may be technically difficult, which requires raising an osseous flap from the posterolateral aspect of the fibula. 13 In 1985, a successful result after an anatomic reattachment of the detached superior peroneal retinaculum and periosteum of the fibula was reported. 2 This procedure is minimally invasive which can recreate the normal anatomy of the superior peroneal retinaculum without any hardware and without sacrificing important normal structures. We have reported a modified, less invasive repair of the detached superior peroneal retinaculum. 1
In this retinacular repair, the detached superior retinaculum and periosteum of the fibula are reattached to the posterior aspect of the fibula to close the false pouch. The injured fibrocartilaginous ridge can be repaired simultaneously if it is present. Although we still do not know the true pathogenesis of dislocation of the peroneal tendons, the superior retinacular repair may be one of the more straightforward procedures for this pathology.
We recognize several limitations of our study. First, the number of patients was small. There is a possibility that our inability to detect a difference in morphology types between patients with and without tendon dislocation was due to the relatively small number of patients, possibly causing a Type II error. Second, we did not evaluate the morphology of the malleolar groove of the fibula quantitatively. Future research could utilize methods that allow quantification of the depth of the malleolar groove. Third, the intraoperative findings of the false pouch and fibrocartilaginous ridge of the malleolar groove in the control group were not evaluated.
Conclusion
Our hypothesis that there was no significant difference in the morphological shape of the fibular malleolar groove between patients with and without dislocation of the peroneal tendons was supported. The presence of the false pouch as well as injury to the fibrocartilaginous ridge may play important roles in the development and/or resolution of this condition.