
Abstract
Background:
Articular cartilage is limited in its ability to repair itself. Matrix-induced Autologous Chondrocyte Implantation (MACI) is an established treatment method for such articular cartilage defects in the knee. Recently the technique has been used in the ankle. We present a series of patients treated with MACI for osteochondral defects of the ankle, and assess the functional and clinical results.
Materials and Methods:
From August 2003 to February 2006, 20 patients underwent MACI grafting for osteochondral defects in the ankle. Age ranged from 19 to 61 (mean, 36) years. Mean followup was 21.1 months. Clinical and functional evaluations were conducted using the AOFAS scoring system.
Results:
The mean size was 233 mm2. There was a significant improvement in mean AOFAS score from 60 (range, 25 to 87) to 87 (range, 41 to 100) (p < 0.0001). Overall improvement in pain scores was also significant (p < 0.0001). All osteotomies healed. Four patients required hardware removal and two underwent arthroscopic debridement for anterior impingement. There were two failures which are awaiting subsequent procedures.
Conclusion:
We believe MACI is a reliable treatment method for talar osteochondral defects. The method usually requires an intra-articular osteotomy, although this proved to be a reasonably simple aspect of the procedure for the treatment of cartilage defects of the talus.
Level of Evidence: IV, Case Series
Keywords
INTRODUCTION
Osteochondritis dissecans (OCD) is a disease of the subchondral bone and cartilage of unclear etiology, though likely to be caused by trauma or vascular insufficiency. It is most commonly reported in the knee, followed by the talus and the elbow. 8,10 Whether OCD of the talus is a precursor to more generalized arthrosis of the ankle remains unclear. 5,21 Nevertheless, the condition is often symptomatic enough to warrant treatment. Spontaneous OCD of the talus usually appears in the second or third decade of life, 3,23 although post-traumatic cases can appear at any time.
In 30% to 40% of cases conservative treatment is not successful and surgical intervention is therefore often sought. 18,24 Several surgical options have been described including: debridement, either in isolation or combined with drilling; excision and curettage; abrasion arthroplasty; and microfracture. 2,3,7,11,17,20,22,24 The optimal solution remains uncertain, and while these methods can give acceptable results in the short term, they lead to formation of fibro-cartilaginous scar tissue which has biomechanical properties significantly inferior to those of hyaline cartilage. 1,16
The introduction of Autologous Chondrocyte Implantation (ACI) advanced the treatment of cartilage defects. ACI involved injecting cultured chondrocytes into the osteochondral defect and sealing it with a periosteal flap or chondrogenic membrane. 4 Postoperatively, over several months, the implanted chondrocytes created a matrix that covered and filled the defect, reducing pain, improving function and creating hyaline-like cartilage. 27
More recently, the technique has been modified to allow chondrocytes to be embedded into a biodegradable scaffold, which is then used to fill the cartilage defect (Matrix-Induced Autologous Chondrocyte Implantation)(MACI), 4,9 thus reducing operative time, eliminating the need for periosteal harvesting, and reducing the likelihood of postoperative complications.
The purpose of this study was to review the results of 20 patients who underwent open MACI grafting of the ankle and to describe the technique. We report our early functional and clinical results of MACI grafting for the treatment of full thickness cartilage defects in the talus.
MATERIALS AND METHODS
After obtaining informed consent, before the surgery, all patients with OCD of the talus treated with MACI grafting between August 2003 and February 2006 were included in the study. Preoperative evaluations included a full clinical history, physical examination of the ankle, and recording of the American Orthopaedic Foot and Ankle Society Ankle—Hindfoot score (AOFAS), 15 which evaluates pain, function and alignment. Preoperative radiographic evaluation included standard anteroposterior and lateral views and a MRI of the ankle.
Twenty patients were included in the evaluation (seven men, 13 women). Eleven lesion were right and nine were left. There were no bilateral cases. The average age at the time of surgery was 36.2 (range, 19 to 61) years. Mean followup was 21.1 (range, 9 to 42) months. The majority of lesions (n = 11) were on the medial aspect of talus. Five lesions were on the lateral aspect and four were anterior. The mean lesion size was 232.7 (range, 63 to 630) mm 2 .
Operative Technique
All procedures were performed with the patient in the supine position under tourniquet control. General anesthesia with a regional block for post operative pain control was used.
In the first stage of the operation, diagnostic ankle arthroscopy was performed to evaluate the site and size of lesion and to obtain a cartilage biopsy (Figure 1). About 100 g of normal articular cartilage was harvested from the margin of the talar lesion, placed in transport medium and sent to the laboratory (VERIGENAUSTRALIA, Nedlands, Western Australia) to be cultivated with autologous serum.
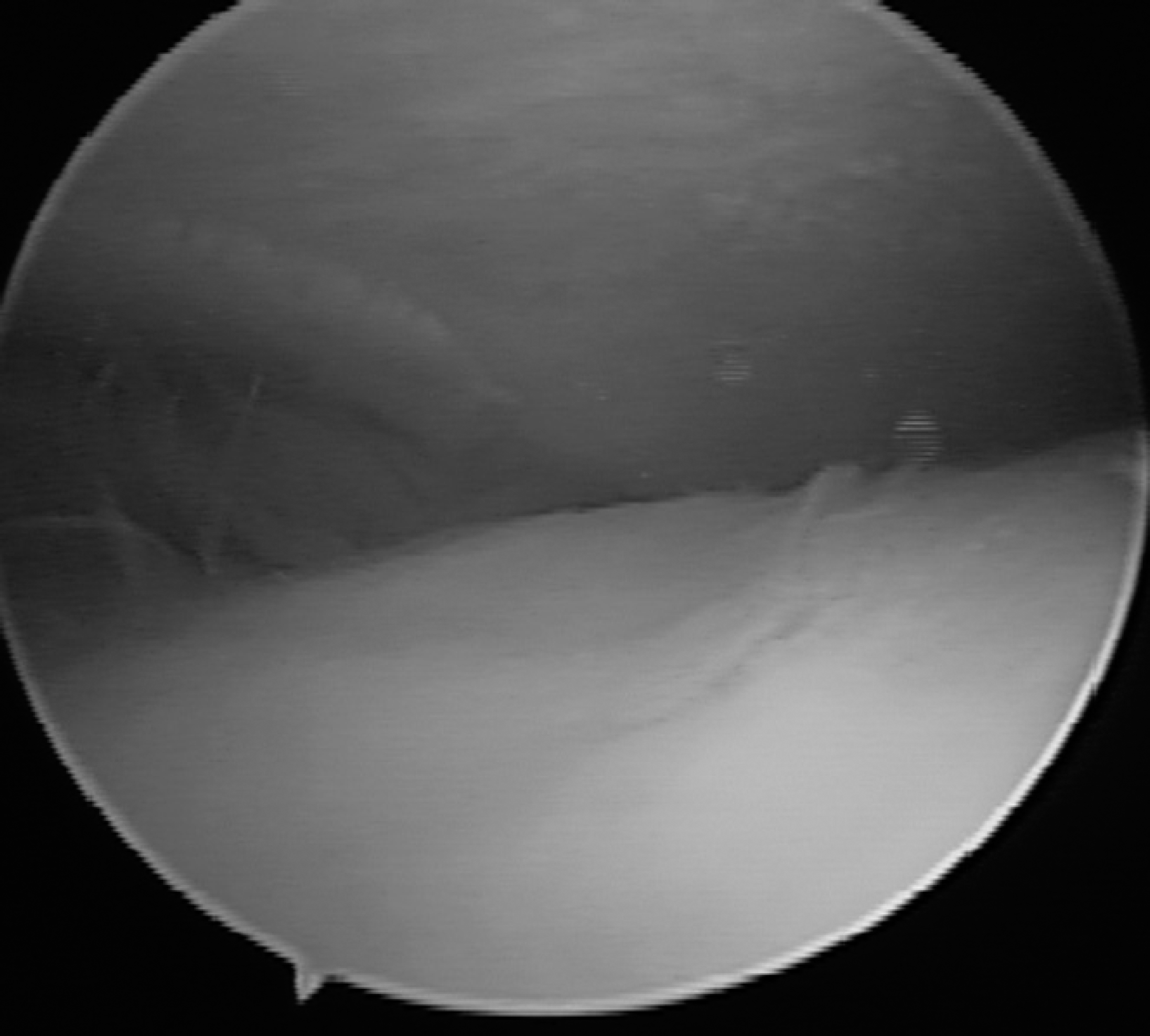
Osteochondral Lesion on the Medial Talar Dome.
The second stage of the surgery was done after 8 to 12 weeks. It was felt that excellent access was mandatory for this procedure as positioning and seating of the graft was critical. We tended to use an intra articular osteotomy to gain access to the lesion in the talus, 11 patients had a medial malleolar osteotomy (Figure 2), five had a lateral malleolar osteotomy, two had an anterior osteotomy and two had an anterior soft tissue approach. After accessing the lesion, it was debrided to normal appearing cartilage on all margins and stable subchondral bone in the defect. The size of the lesion was measured from a foil template prepared using a suture package and the MACI graft was then cut around the template to fit the lesion.

Medial malleolar osteotomy and preparation of the defect.
The graft was fabricated with a porcine collagen membrane with approximately 1×106 chondrocytes per cm 2 embedded in the ‘rough side’ (Figure 3). After being cut to size it was placed into the lesion with the rougher side (containing the cells) facing the defect. Care was taken to ensure that the graft fit perfectly into the defect with no overhanging material and it was then secured using fibrin glue (Tisseel™, Baxter Health Care Corporation) spread thinly over the entire defect. Firm digital pressure was applied to the graft for one minute while the glue set. Stability of the graft was assessed by putting the ankle through a range of motion and the osteotomies were fixed with pre-drilled titanium screws and plates as required (Figure 4).
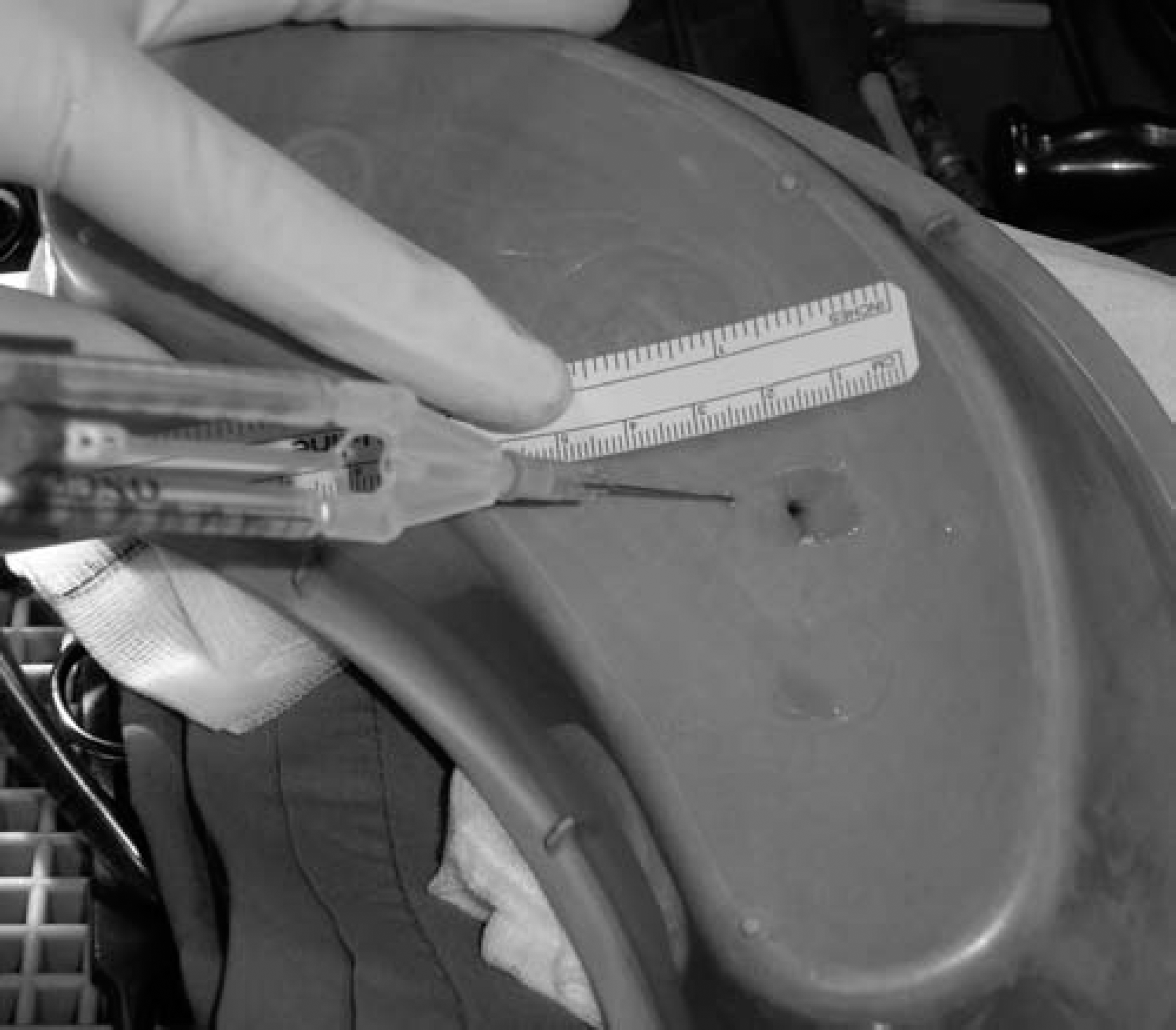
Membrane with implanted chondrocytes after it has been cut to fit the defect. Fibrin glue in the double barrel syringe is laid into the base of the defect and the graft is pressed into it using firm digital pressure.

MACI graft secured in the defect.
Postoperative Management
Patients were kept nonweightbearing for 6 weeks, which included 1 week in a below-knee posterior splint and 5 weeks in a removable walker boot. Range of motion exercises were allowed once the surgical incision healed. The walker boot was tapered off at the end of 6 weeks and full weightbearing allowed over 7 to 9 weeks. Full activity, with the exception of heavy impact activities, was allowed between 9 to 12 weeks.
Clinical evaluations using the AOFAS scores were performed at all followup visits.
Statistical Analysis
The preoperative and postoperative AOFAS scores, pain and site of lesion were compared with paired and unpaired t-tests. The level of significance was set at p < 0.05. Pearson's Correlation Coefficient was used to compare the area of the lesion and improvement in AOFAS scores. 19
RESULTS
The AOFAS score improved significantly from a preoperative mean of 60.0 (range, 25 to 87) to a postoperative mean of 86.9 (range, 41 to 100) (p < 0.0001). Pain improved in fourteen patients, remained unchanged in five and worsened in one. Overall improvement in pain scores was statistically significant (p < 0.0001).
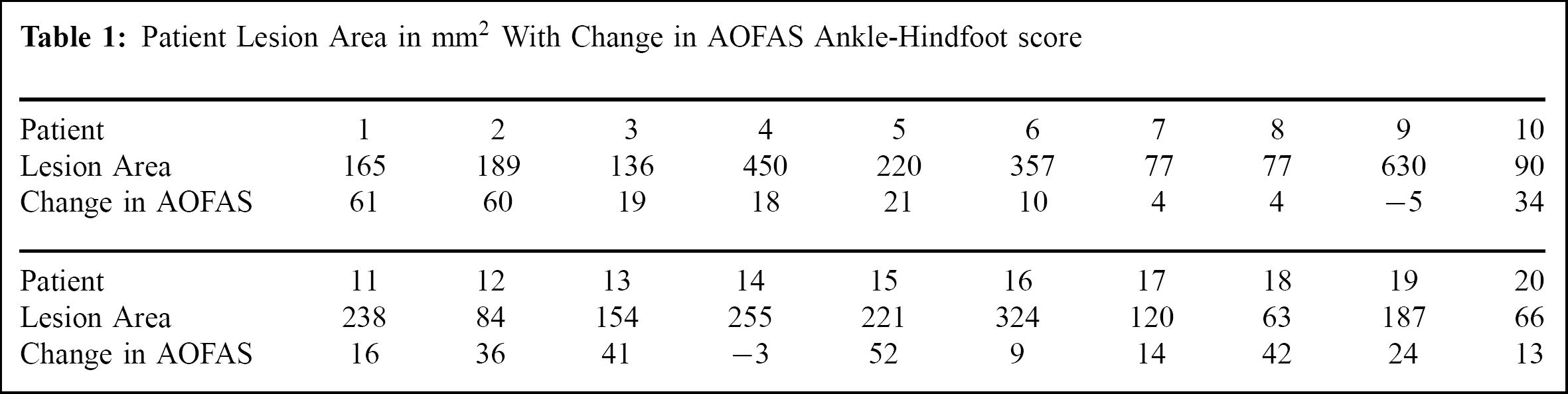
The mean lesion size was 232.7 (range, 63 to 630) mm 2 . There was a moderate inverse correlation between lesion size and improvement in AOFAS scores (Pearson's Correlation Coefficient, r = −0.394). There was no association between age or the site of lesion and change in AOFAS scores.
Complications included two anterior graft impingements, two patient with recurrent pain associated with hardware, and two clear failures with persistent pain and synovitis. One of the failed cases had the graft removed. Additional surgery was required in seven patients, which included hardware removal (five cases), arthroscopic ankle debridement (three cases) and posteromedial release of ankle with tendoachilles lengthening (one case). Some patients had a combination of procedures. All patients who had hardware removal had arthroscopy of the ankle and biopsies taken for histological assessment.
DISCUSSION
This paper reports the results of 20 MACI graft implants to the talus for osteochondral lesions. Seventeen out of 20 patients reported a satisfactory outcome based on AOFAS Ankle-Hindfoot scores which is a comparable short term outcome to any other reported method of management of these lesions. 1,3,13,14,16,18,22,25 One review paper 24 described the success rate for conservative treatment at 45%, for excision of lesion, 38%, for excision and curettage, 78%, and 85% for excision, curettage and drilling, although they reported a range of treatments and study designs making definitive conclusions difficult
With up to 88.8% excellent results reported treating OCD of the knee using osteochondral autografts 1,13,14,18 some surgeons were encouraged to consider applying the technique in the ankle, The main disadvantages of this technique however are donor site morbidity and difficulty in matching the talar surface geometry, particularly at the edges.
ACI, with its potential to produce hyaline-like cartilage at the defect site, has opened up new possibilities in the treatment of OCD of the ankle. Several papers 16,25 reported good to excellent results, but there were technical limitations related to ACI including non homogenous distribution of chondrocytes in the defect, the risk of leakage if the periosteal patch is inadequately sealed, complications at the periosteal donor site, and periosteal patch hypertrophy.
Patient Lesion Area in mm 2 With Change in AOFAS Ankle-Hindfoot score
The MACI technique avoids these problems. No periosteal patch is required and the collagen membrane can be secured using fibrin glue. There is some uncertainty about the use of fibrin glue in ACI grafting. 16 However, other studies have proven that chondrocytes migrate through fibrin glue within 2 weeks of implantation and form an integral part of the MACI biscaffold. 26 While the controversy on the effect of fibrin glue on MACI is, as yet, unresolved it was our policy to apply fibrin glue sparingly.
The disadvantages of the MACI procedure are the requirement for two procedures and a the need for an osteotomy to approach most lesions. The osteotomies include the risk of nonunion, symptomatic hardware, and injury to a previously uninjured articular surface. In our study all osteotomies healed without sequelae. Four cases required hardware removal. Arthroscopic examination of some of the osteotomies (six cases: one patient was examined arthroscopically by another surgeon and no comment was made on the osteotomy) found the articular surface to have healed well.
There have been anecdotal discussions about performing the implantation arthroscopically. Accurate seating of the graft is critical so that it is protected in a ‘recessed space’ while it matures and stabilizes. We did not feel confident that we could reliably position and seat the graft arthroscopically to ensure that it would not shear off with loaded ankle movement, so all implants were performed as an open procedure.
There were several shortcomings in our study. Our study group was relatively small, an average followup period of only 21 months, and there was no control group. Our results compare well, however, with results obtained by other authors using other procedures with similar followup.
MACI grafting of talar dome lesions seems to be a promising treatment method, although at this stage it is quite resource intense, requiring two surgical procedures and expensive laboratory input. The results of this technique in the treatment of OCD of the talus should be investigated in a larger number of patients with longer followup to draw more definitive conclusions on its long-term effectiveness.
Footnotes
EDITOR'S NOTE
This technique could make an autologous chondrocyte procedure more reliable since there would not be a risk of the cells leaking from under a periosteal graft as used in the ACI treatment. It is concerning that six of 20 patients reported no improvement in pain.