
Abstract
Level of Evidence: V, Expert Opinion
INTRODUCTION
Osteochondral lesions (OCLs) continue to present a challenge to orthopaedic surgeons. Their incidence, especially in young, sporting individuals, is rising. 5,16,17,27 It is known that such lesions have a limited repair capacity, 13,18 especially in the skeletally mature. 21 Persistent osteochondral defects can gradually lead to degeneration of the articular cartilage 11 and may eventually lead to osteoarthritis (OA). 6,21,25
A number of surgical options are available for patients with osteochondral defects. These include arthroscopic debridement and microfracture, autogenous osteochondral grafting (OATS procedure), Matrix—Induced Autologous Chondrocyte Implantation (MACI), Autologous Chondrocyte Implantation (ACI) and Periosteal suturing.
When an OCL presents with an associated cysic lesion, simple debridement and microfracture may not be sufficient and an attempt to restore the congruence of the weightbearing surface may yield superior results. 10,12,22,23 The ideal procedure would also restore hyaline cartilage to the joint surface.
Synthetic grafts offer a number of potential benefits over other treatment options. They require only a single procedure as opposed to two-staged treatment for MACI and ACI. There is no morbidity to healthy host tissue as seen in the OATS procedure and periosteal suturing. The surgery is also technically easier to perform with a small learning curve.
Tru-fit™ is a biphasic osteochondral biodegradable substitute currently available for the treatment of articular osteochondral defects. The osseous substitute consists of a matrix of calcium triphosphate. The cartilaginous substitute consists of poly DL-lactide-co-glycolide. Tru-fit™ is marketed as having the potential to induce hyaline-like cartilage and is used for “back-filling“ of autogenous cartilage-bone transplantation (mosaicplasty). It is licensed in the UK for use as an osteochondral graft for osteochondral lesions. A case report of its successful use for grafting of a greater tuberosity cyst prior to rotator cuff repair has been published. 1 Another study investigated a synthetic allograft analogous to Tru-fit™ in pigs as a conduit for ACI with some success. 14 In that study, at 6 months all of the 38 implanted sites were filled with firm bone which was covered with either fibrous or cartilaginous tissue. We are unaware of scientific literature supporting its use in osteochondral lesions in humans.
In this case report, we report early success in the treatment of a distal tibial osteochondral lesion using the Tru-fit™ synthetic graft.
CASE REPORT
A 41-year-old male presented with recurrent pain in his right ankle. He had a history of two significant inversion injuries to the ankle 10 and 5 years earlier. He had previously enjoyed recreational sports including soccer and badminton. He had been initially able to return to sports after the two injuries but, over the past few months, was no longer able to participate in these due to his ankle pain. On a day-to-day basis, however, he had no problems and no limitations in his activities of daily living. There was no history of rest or night pain. His AOFAS ankle score 15 on presentation was 66, his AOS score 9 for pain was 30% and his score for disability was 18%. His total SF-36 score 28 was 51 with a mental component score of 66 and a physical health score of 37. He had no significant past medical history other than mild hypertension and was a non-smoker.
On examination he had normal hindfoot and forefoot alignment with a normal arch. There was no evidence of swelling and no tenderness around the ankle or foot. He had a full range of motion of the ankle and foot and no instability on anterior drawer or talar tilt tests. All tendons appeared to function normally and there was no neurovascular abnormality.
Plain radiographs suggested a cystic lesion within the distal tibia. An MRI scan confirmed a 1.3 × 0.8 cm osteochondral lesion involving the anterior, middle third of the tibial plafond. There was a significant bone cyst deep to this lesion with surrounding bone marrow edema (Figure 1). The ankle ligaments and the remainder of the articular surfaces of the ankle joint were intact.
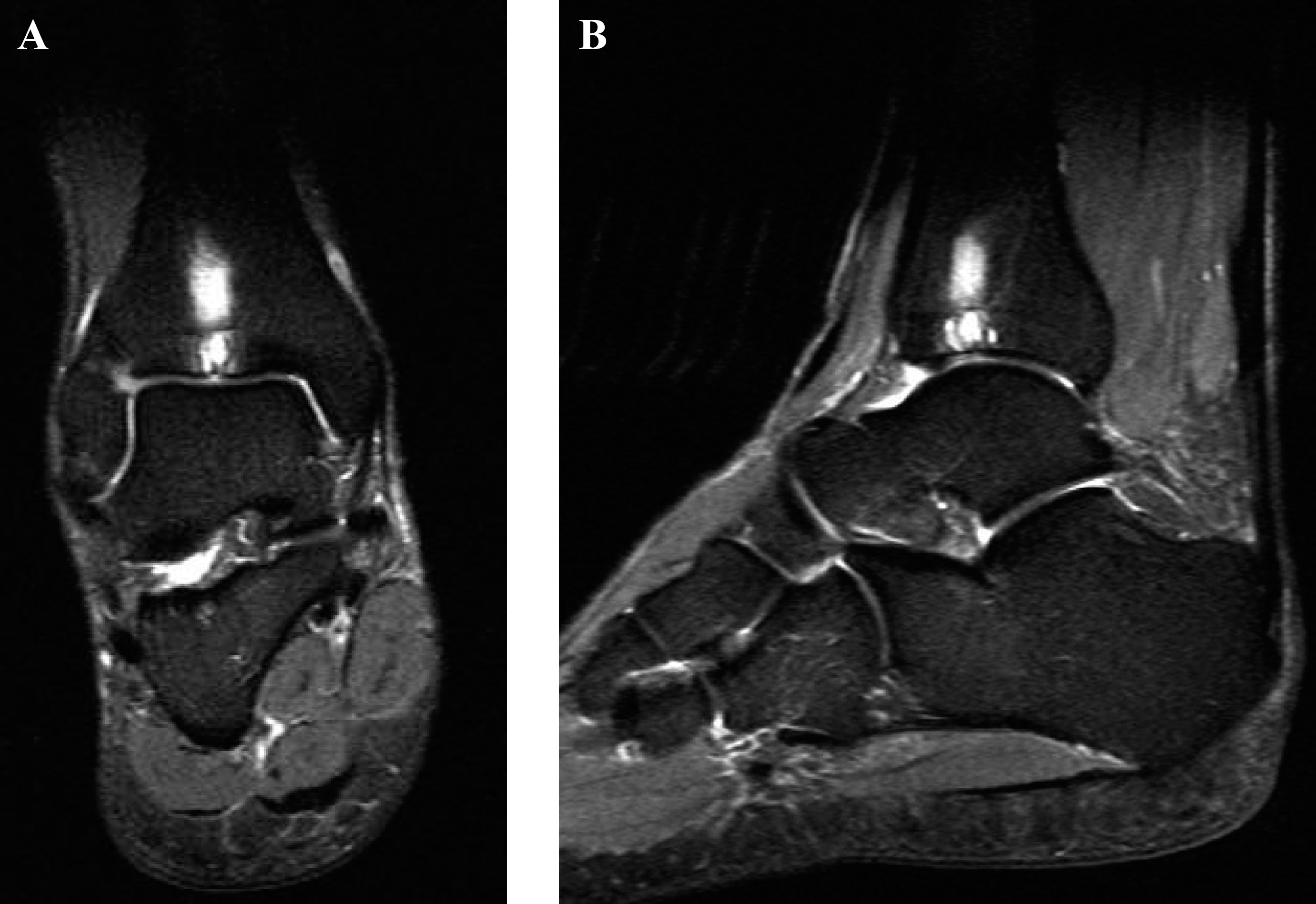
Preoperative coronal (A) and saggital (B) MRI scan images demonstrating the OCL of the distal tibia with an underlying cyst and surrounding bone marrow oedema.
After appropriate pre operative counselling and informed consent, the patient underwent surgery. Examination under anesthetic (EUA) confirmed that the ankle was stable. An arthroscopy was performed via anterolateral and anteromedial portals. A Grade I/IV lesion was noted on the central region of the talus opposite a Grade II/IV 20 lesion of the tibia with unstable cartilage overlying a large cyst. The osteochondral lesion was thoroughly debrided and the cyst curetted leaving a substantial cavity. An ACL drill guide (ACUFEX™, Smith & Nephew, Andover, MA) was used to used to pass a guide wire from the anterior tibia into the center of the tibial lesion as near as possible to the perpendicular axis of the tibial curved articular surface. This was then reamed with the 7 mm ACL tibial tunnel drill to create a tibial window. A size 7 Tru-fit™ graft was inserted in an antegrade manner into the defect, using a similar method to that described by Ueblacker et al. 26 Postoperatively the patient was kept partially weight bearing on crutches for 6 weeks. Physiotherapy commenced with range of motion at 10 days and proprioceptive work at 6 weeks.
At 6-weeks followup he had regained full range of motion of the ankle. At 4 months he was free from any day to day discomfort in the ankle and had commenced sports including running but had not returned to playing soccer. At 8 months after surgery he suffered an unrelated health problem (transient ischemic attack) which has affected his recreational activities. However, at the latest followup, 1 year after surgery, he classed himself as ‘very satisfied’ with his ankle. He continues to subjectively say that he has no pain in the ankle. At 1 year, his AOFAS score was 90 his AOS score for pain was 38% and for disability was 12%. His SF-36 score was 84 with a mental health component score of 81 and a physical health component of 80.
A followup MRI (Figure 2) scan at 1 year demonstrates good incorporation of the plug with resolution of the surrounding bone marrow edema. There continues to be high signal within the plug itself however. Qualitative T2 mapping (Figure 3) revealed a disorganized pattern of T2 signal from the deep to superficial zones of the cartilage portion of the plug, suggesting a fibrous rather than hyaline cartilage composition. 29
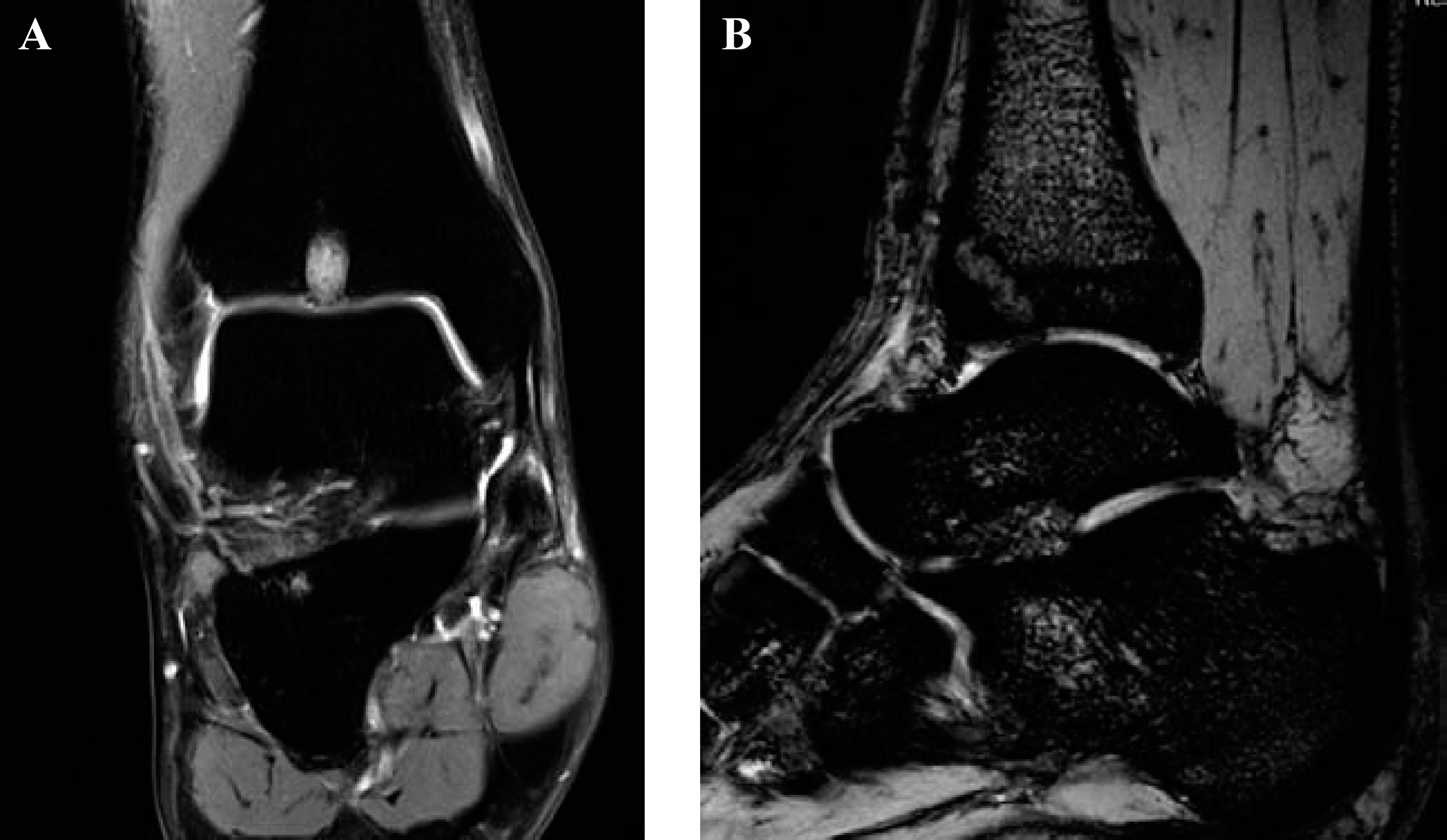
Postoperative coronal (A) and saggital (B) MRI images showing integration of the plug and resolution of the bone marrow oedema but continued high signal within the plug itself.

Qualitative T2 mapping showing a disorganised pattern within the cartilage portion of the plug, suggesting that it is composed of fibrocartilage.
DISCUSSION
Osteochondral lesions of the talus account for around 4% of all osteochondral lesions 2 and their incidence is rising as our awareness of them increases and modern imaging techniques aid in their diagnosis. Tibial plafond lesions are rare and were first reported in the series by Bauer et al. in 1987 4 which investigated the natural history of OCL around the ankle. Two tibial plafond lesions were identified over a 20-year period, compared with 82 talar lesions. The reason for the difference in frequency between talar and tibial lesions may be due to stiffer cartilage in the distal tibia 3,8 as well as the fact that osteochondral injuries in general are more common on the convex surface of a joint.
Mostly case reports have been published describing the treatment of tibial OCL. 7,8,24,26 Mologne and Ferkel recently published a retrospective analysis of their series of osteochondral lesions of the distal tibia. 19 This confirmed the infrequent presentation of these lesions, even in a complex foot and ankle referral practice where only 23 tibial OCLs were encountered in a series of 880 ankle arthroscopies (2.6%). The results of the arthroscopic treatment of 17 of these were reported in that paper with two patients who underwent iliac crest bone grafting of an associated cyst one of whom had a poor result. Fourteen of the 17 patients had excellent or good results at a mean followup of 44 months.
A ‘mirror image’ lesion of the tibial plafond opposite a talar osteochondral lesion has been described. 7 This was treated with curettage and grafting of the subchondral cysts and replacement of the cartilaginous flaps. The patient was asymptomatic after 3 months. Bilateral symptomatic distal tibial osteochondral lesions have been reported in a military recruit with no history of trauma. 24 These lesions were treated conservatively as the patient refused surgical treatment and at 3 years there was no pain during daily activities but continued anterior ankle pain on intense physical activity.
Ueblacker et al. 26 described two distal tibial lesions which were treated with single, 11 mm osteochondral plugs taken from the patients' femoral trochlea. Both had good results. Chapman and Mann 8 reported the case of a traumatic anterocentral OCL of the distal tibia. This was initially treated with debridement and microfracture; however, 9 months after this procedure the patient's symptoms had worsened. An osteochondral allograft procedure was undertaken with further arthroscopic debridement of synovitits and fraying tissue around the allograft some months later. This patient continued to have constant, mild pain. While he was able to stand for long periods, he had not returned to his previous occupation at 2 years after the grafting procedure.
Our patient is very satisfied with the outcome of his surgery and has stated that he would have the procedure again. Clinically, his function has improved after the surgery and radiographically, his cystic lesion improved although the cartilage over the plug appears to be of fibrous rather than hyaline morphology. We believe that much of the symptomatic improvement is due to the filling of the cystic lesion beneath the OCL allowing a stable scaffold for the hyaline-like or fibro-cartilage. We advocate standard arthroscopic debridement and microfracture/drilling techniques for OCLs of the tibia where there is no cystic formation. We describe an alternative to autogenous osteochondral grafting of a tibial sub-cortical cyst which eliminated the risks of harvesting from the knee.
CONCLUSION
The clinical and radiological results of this novel procedure at 1 year in this case are encouraging, but more patients and longer followup are required before firm conclusions can be drawn.
Footnotes
EDITOR'S NOTE
Both reviewers had some concerns regarding this paper. One felt it important to emphasize that the synthetic plug used in this study is not approved by the FDA in the US. The other was concerned that no biomechanical data exists regarding the strength of this implant and thus it may not be durable enough to withstand the forces it would experience at the joint surface in all cases.