
Abstract

INTRODUCTION
Triple arthrodesis has become a common surgical procedure to stabilize and correct a variety of pathological processes affecting the foot. The word triple arthrodesis is a blanket term describing many different procedures performed with the common element of fusing three joints in the hindfoot: the talocalcaneal, talonavicular, and calcaneocuboid. Differences between techniques generally consist of alternative osteotomies to correct deformities and a variety of surgical approaches. Edwin Ryerson 10 is given credit for first describing the triple arthrodesis in 1923. Review of his initial description gives credit to Gwilyn Davis of Philadelphia, who attempted fusion of the talocalcaneal and talonavicular joints in order to correct cavus foot deformities primarily in polio patients. Ryerson added lateral column fusion to assist in correcting severe varus deformities which were not corrected by Davis' technique.
These early techniques spawned the many operations designed to establish a plantigrade foot capable of painless weightbearing. Early procedures relied on well molded plaster casts to maintain correction. 13 Malunion and recurrence of the deformity were common. The addition of rigid internal fixation significantly decreased these complications, though adding a new collection of technical errors. 11
Many long term studies of primary triple arthrodesis exist. 1 –6,8,11,12,14 –16 These studies range from analysis of the procedure for conditions such as Charcot-Marie-Tooth disease and polio 4,12,15 to review of specific techniques. Poor results range as high as 47%. A literature review reveals recurrence rates of 9% to 20%; nonunion from 6% to 33% and incomplete correction of the deformity in as high as 70% of the patients. 1 –6,8,11,12,14 –16 It is this latter group that is the most intriguing, as this would seem to be a preventable complication in the era of rigid internal fixation.
Incomplete deformity correction can be assessed through a variety of anatomic planes. One such plane, the frontal plane, defines rotation of the foot. A common technical error (particularly in those undergoing triple arthrodesis for severe flatfoot) involves leaving the foot in residual fixed supination, as the surgeon's attempt to correct severe pronation associated with flatfoot deformity (Figures 1 and 2). Correction of the heel out of longstanding valgus creates supination of a fixed forefoot. 7 The surgeon may attempt to compensate for this supination by rotating the talonavicular joint plantarward, creating a cavus configuration in the sagittal plane. As is well known, patients with a cavus deformity have a tendency to load the lateral border of their foot during the stance phase of the gait cycle (Figure 3). This impaction force is concentrated at the fifth metatarsal base, creating the potential for stress fracture (Figure 4) and persistent pain. This force is magnified by the rigidity of the foot created by the triple arthrodesis. To compensate, the surgeon's next intraoperative maneuver is to place dorsal pressure on the cuboid bone, to “derotate“ the fixed supination and cavus.

Preoperative anteroposterior (A) and lateral (B) radiographs of a patient with a severe rigid flatfoot deformity. Note the sagittal radiograph demonstrates pre-existing lateral overload of the fifth metatarsal base. This patient accommodates this overload through maintenance of some flexibility through the lateral column.
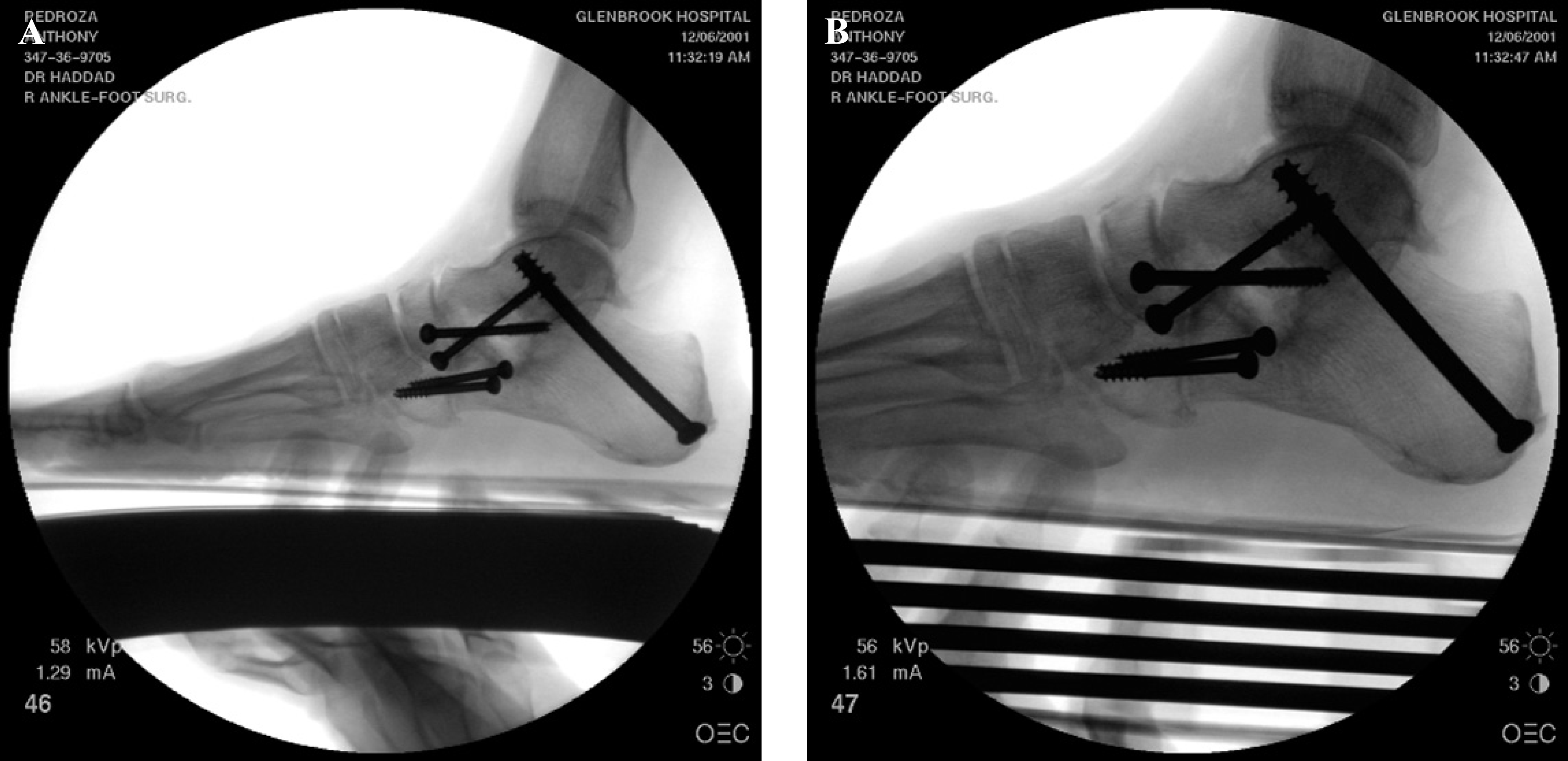
Intraoperative fluoroscopy demonstrating restoration of the talo-first metatarsal angle to zero degrees (A), completing the alignment of the medial column. Note in the magnified sagittal fluoro (B) that the fifth metatarsal remains in contact in the simulated weightbearing stance phase.

Three-month postoperative weightbearing radiograph demonstrating successful union of the triple arthrodesis. Note the lateral column remains in contact with the weightbearing surface.

At 9-months postoperative, the patient develops acute pain in his fifth metatarsal base without injury. Lateral radiograph (A) demonstrates maintenance of the talo-first metatarsal angle. A magnified lateral radiograph (B) reveals a fifth metatarsal fracture, confirmed on the oblique (C) foot radiograph.
Unfortunately, the calcaneocuboid joint has limited mobility, and follows the talonavicular joint due to its linkage at Chopart's articulation. As such, the concept of incomplete correction becomes less of the fault of the individual surgeon, and more of a response to the complex anatomy of the patient.
SOLUTION
To address the problem of lateral overload while maintaining the correction of both the hindfoot valgus and fixed supination of the forefoot, the author incorporates a cuboid osteotomy in addition to the calcaneocuboid arthrodesis component of the triple arthrodesis (Figure 5). This additional osteotomy adds sufficient power to eliminate lateral overload during stance phase, compensating for the need to rotate the talonavicular joint into significant plantarflexion.
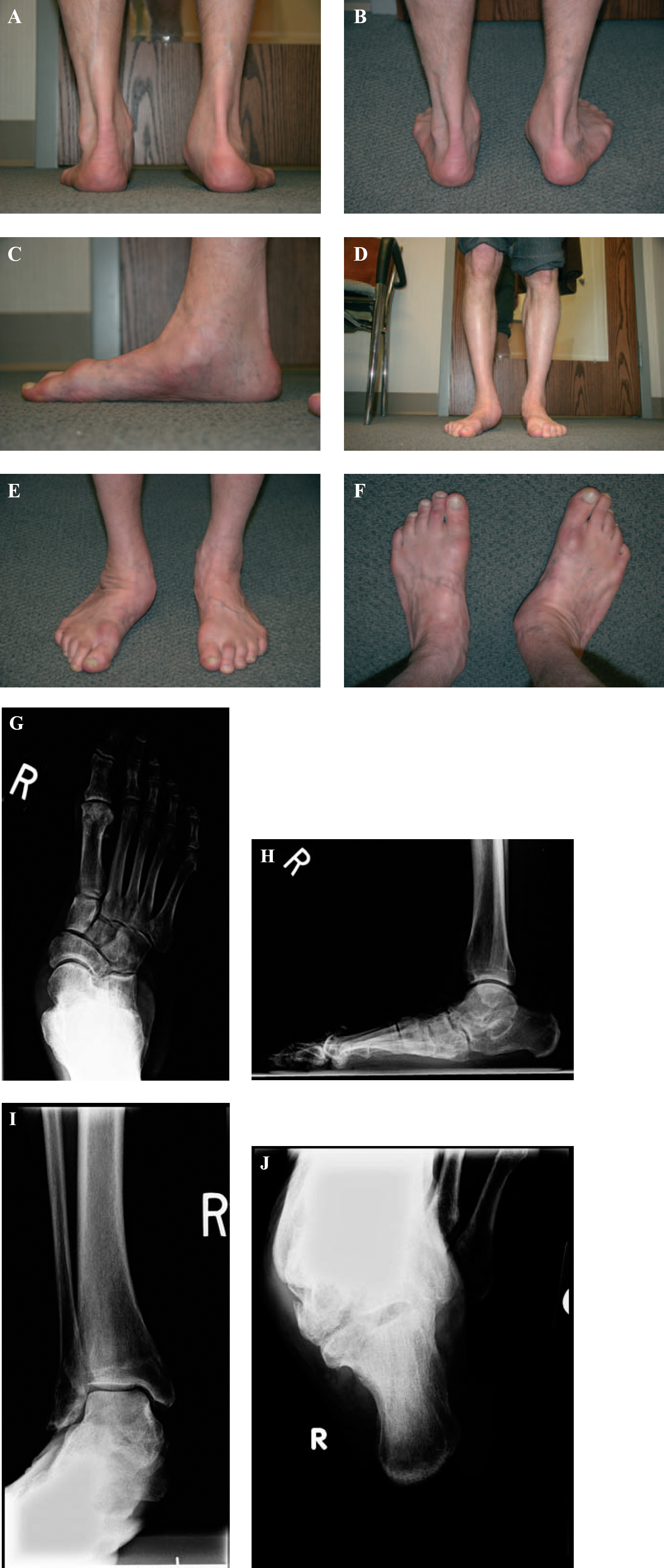
Multiple clinical views (heels (A); oblique heels (B); medial foot (C); anterior legs (D); oblique ankles (E) and anterior feet (F)) of a patient with a severe rigid flatfoot. Radiographs demonstrate significant peri-talar subluxation on the anteroposterior foot (G), lateral column overload with an increased talo-first metatarsal angle on the sagittal view (H), subfibular impingement on the anteroposterior ankle view (I) and hindfoot valgus on the axial calcaneal view (J). This patient's deformity requires a triple arthrodesis due to the rigidity and painful arthritis.
OPERATIVE TECHNIQUE
The subtalar joint is prepared and fused in 5 degrees of hindfoot valgus in a routine fashion. This is then followed by preparation of the talonavicular joint and calcaneocuboid joint with congruent surfaces. The talonavicular joint is rotated to compensate for the fixed forefoot supination and provisionally pinned with one guide wire. The use of one guide wire (rather than multiple) allows dorsal pressure to be applied to the cuboid. It is important not to maximize this pressure, as the surgeon will then create incongruency about the talonavicular articulation (as it is not a perfect sphere). After placing Chopart's joints in the best practical rotation to compensate for fixed supination, the joints are rigidly fixed.
Now, the surgeon assesses the position of the foot via simulated weightbearing with a flat plate and via direct visualization (Figure 6). If the fifth metatarsal is demonstrating overload in the sagittal plane, the patient is a candidate for a cuboid osteotomy. The standard lateral approach is extended to allow visualization of the entire cuboid bone. The mid-portion of the cuboid is marked, and a microsagittal saw or straight osteotome is used to create an osteotomy in the sagittal plane (Figure 7A). The surgeon must insure that this osteotomy traverses the entire bone of the cuboid, as the shape of this bone does not lend itself to simple sectioning (Figure 7B). In addition, the surgeon must not pry the osteotome (Figure 7C) strongly within the osteotomy, as the density of the cuboid is less than the adjacent bones, which may lead to crushing the cuboid and creating incongruency in the osteotomy. Use of an external distractor (Figure 7D) not applied within the osteotomy site is helpful to allow rotation of this cut.
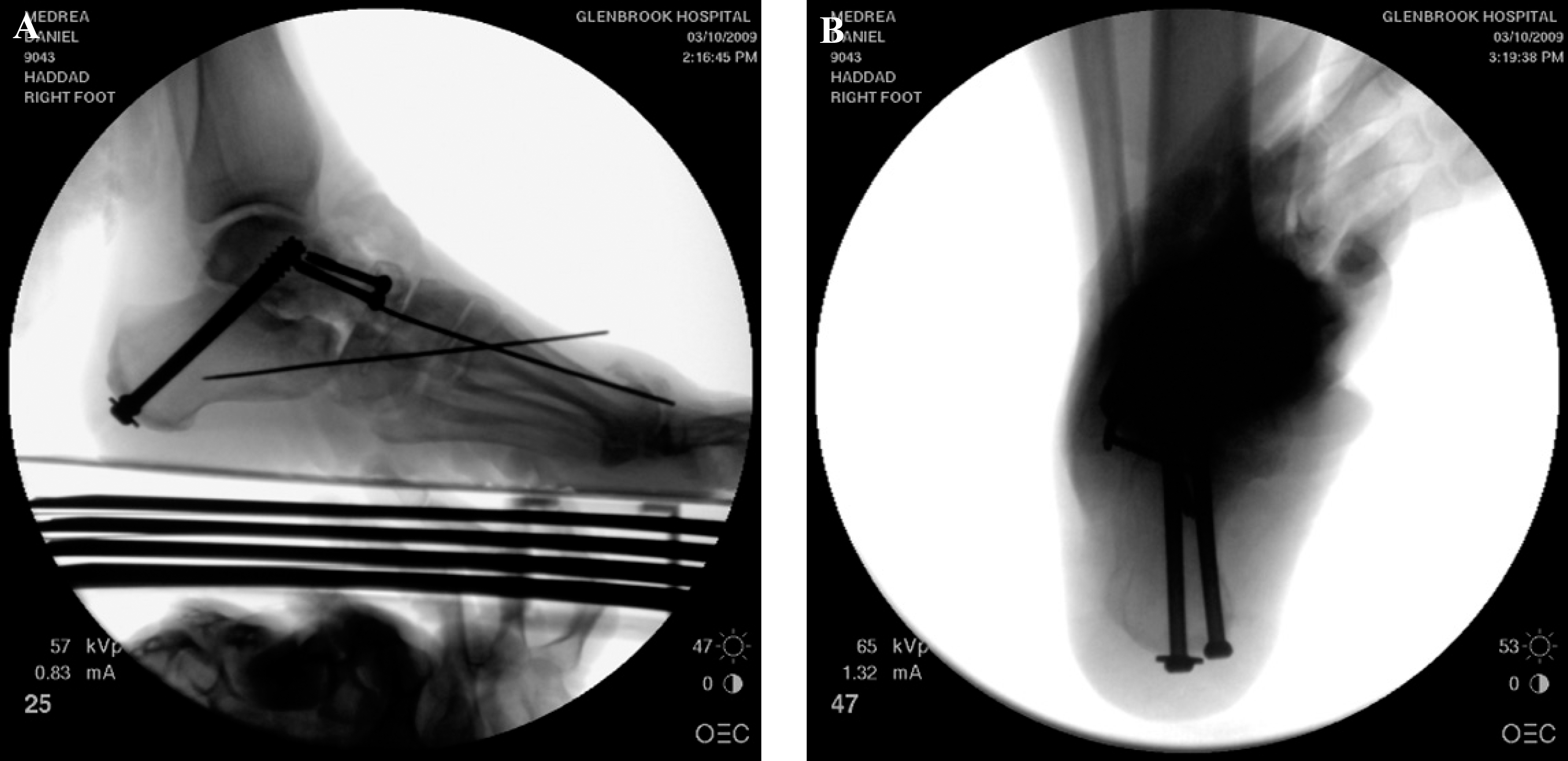
Intraoperative fluoroscopy demonstrates initial correction of the talo-first metatarsal angle in the sagittal plane (A) with residual lateral column overload. The axial calcaneal view (B) demonstrates appropriate hindfoot valgus.
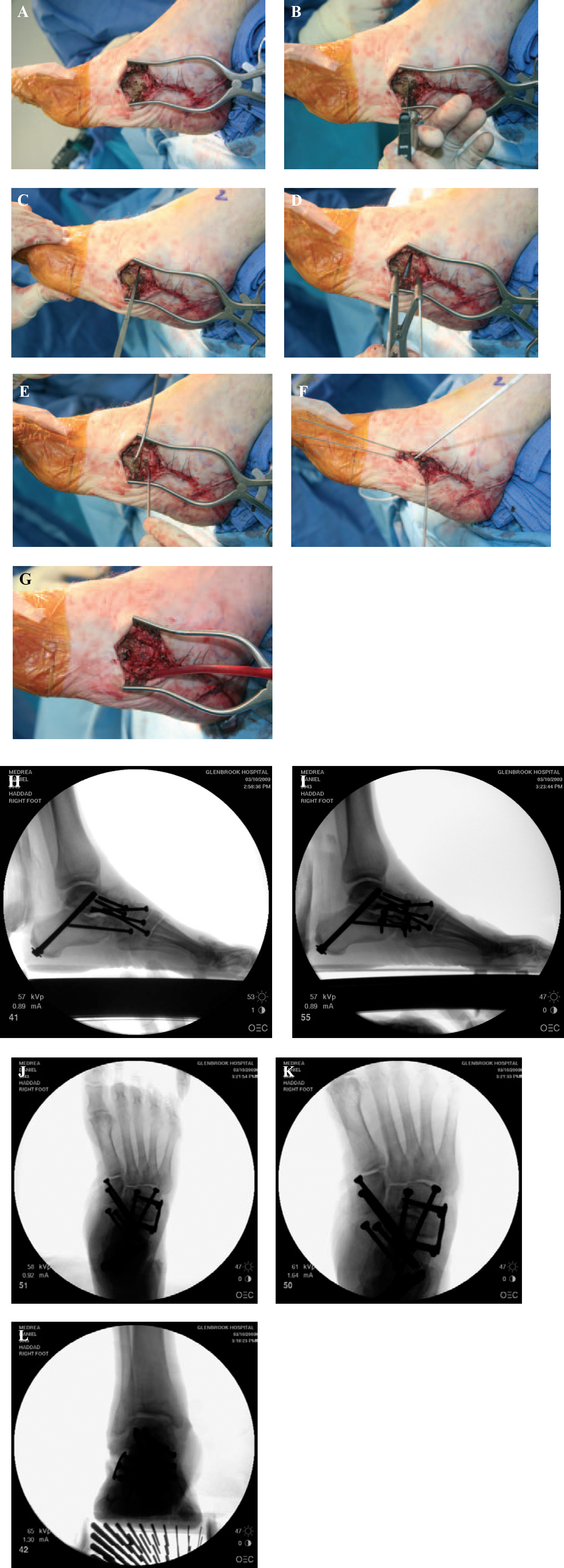
Intraoperative visualization of the cuboid osteotomy. The cuboid is a broad bone (A) which allows ample room for the osteotomy with a microsagittal saw (B). An osteotome is used to complete the osteotomy (C), followed by distraction of the proximal and distal fragments (D). The proximal and distal segments are pinned with parallel “joysticks“ to assist with the derotation (E), and the osteotomy is provisionally pinned with guide wires after the bone is rotated at the osteotomy (F). Note the change in position of the initially parallel “joysticks.“ Screw fixation is rigid (G) preventing recurrence. Fortunately, the bone is cancellous and heals rapidly. Correction may be initially maintained with a lag screw from the cuboid into the calcaneus (H). It is then secured with a compression staple (I), maintaining the talo-first metatarsal angle while offloading the lateral column. Note the height of the fifth metatarsal base off the simulated weightbearing axis. Final anteroposterior fluoroscopy (J and K) demonstrates correction of the talo-first metatarsal angle in this plane, and a magnified view reveals how the staple crosses both the osteotomy and the calcaneocuboid joint arthrodesis (L). Anteroposterior ankle fluoroscopy reveals elimination of the subfibular impingement.
Once complete, the surgeon may apply strong dorsal pressure against the base of the fifth metatarsal, creating a pronation force that offloads the fifth metatarsal base. Assistance with rigid “joysticks“ (Figures 7E) provides excellent control of rotation. The segment of the cuboid distal to the osteotomy site moves superior easily, and the cuboid is provisionally pinned in this corrected position (Figure 7F). A flat plate is once again used to ensure adequate derotation of the fixed supination (Figures 7G). If sufficient, fixation is achieved most commonly with a dynamic compression staple that maintains correction. Isolated compression screw fixation is challenging given the width of the cuboid bone (eliminating proximal-to-distal fixation through the calcaneus into the cuboid), and the width of the calcaneus in the transverse plane (eliminating distal-to-proximal screw fixation from the cuboid into the calcaneus). Of course, these are not absolute technical challenges, but should be considered in advance of the osteotomy to allow surgeon preparation for adequate hardware. If the cuboid sagittal distance is insufficient, the author suggests either crossing the calcaneocuboid joint arthrodesis with the compression staple (allowing its permanent implantation) (Figure 7, H to L), or crossing into the fourth or fifth metatarsal base as a bridge plate (requiring later removal).
POSTOPERATIVE PROTOCOL
The patient undergoes standard immobilization under the surgeon's protocol for a triple arthrodesis. This osteotomy does not add to the recovery time with respect to immobilization and/or weightbearing. In our hands, this osteotomy has successfully healed in a routine 6-week time interval (Figure 8).
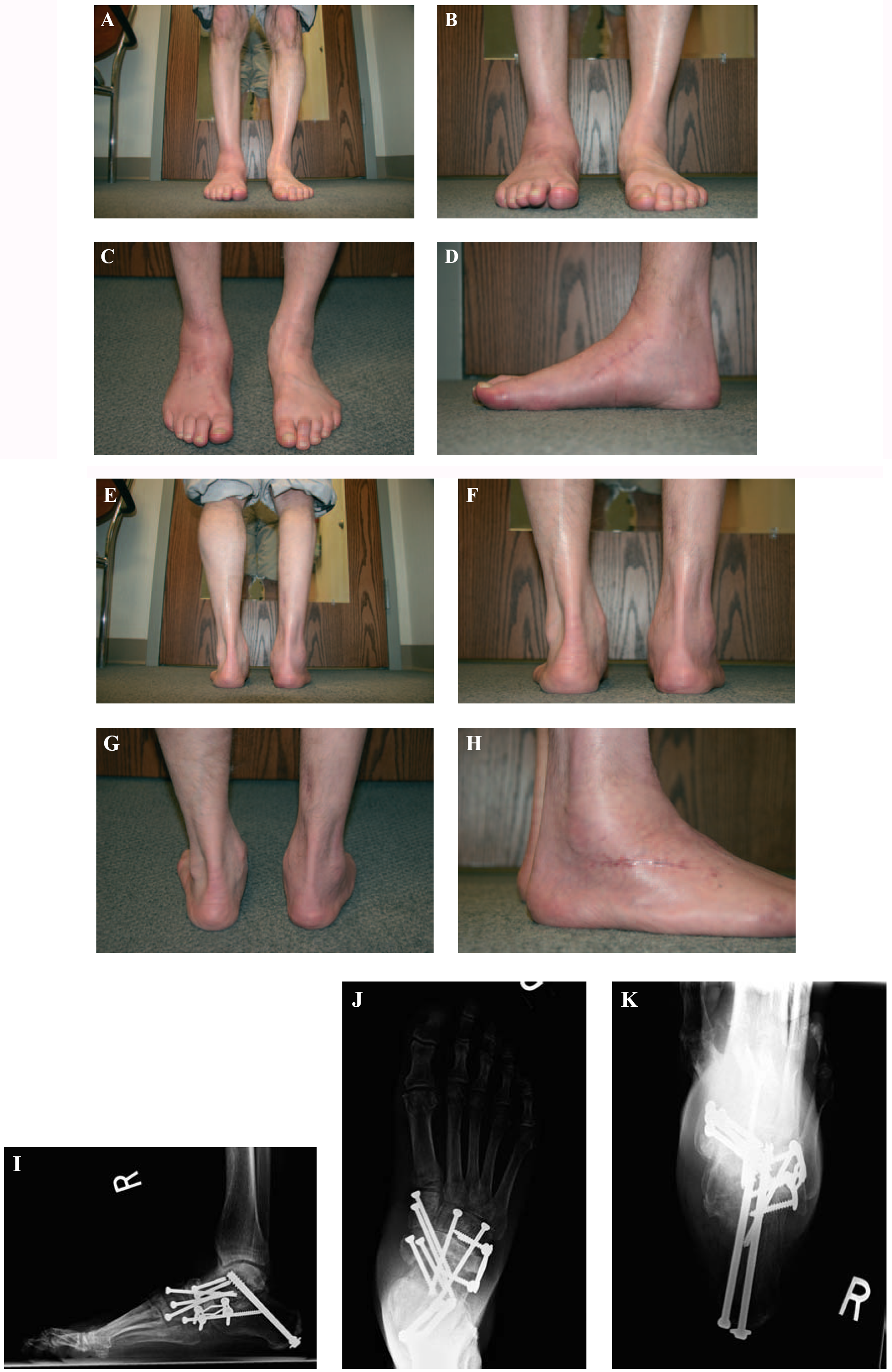
Clinical photographs of this same patient at 4 months postoperatively (anterior legs (A), anterior ankles (B), oblique ankles (C), medial foot (D), posterior legs (E), heels (F) and oblique heels (G)) all demonstrate significant correction of the pre-operative deformity. The lateral incision (H) is noted to extend distal to the standard lateral approach for a triple arthrodesis. Radiographs confirm maintenance of correction in the sagittal plane (I) with lack of lateral overload. The anteroposterior weightbearing radiograph (J) reveals maintenance of the talo-first metatarsal angle, and the axial radiograph (K) demonstrates appropriate hindfoot valgus. This correction would not have been achievable without the addition of the cuboid osteotomy to offload the lateral column.
CONCLUSION
The value in cuboid osteotomy is its ability to provide additional powerful correction, with predictability of union. The cuboid bone is primarily cancellous and vascular, and has a high propensity to heal uneventfully. Thus, it is the surgeon's duty to place the osteotomy into the appropriate position and provide rigid internal fixation. In doing so, he or she subsequently minimizes the potential for incomplete correction seen following a standard triple arthrodesis.