
Abstract
Background: Prone ankle and subtalar arthroscopy is challenging in part due to the limited working space in these joints. Materials and Methods: Fourteen patients undergoing prone posterior arthroscopy with a novel skeletal traction method were reviewed and the technique detailed. Results: No complications were observed in 14 patients treated with a minimally invasive skeletal traction technique for prone ankle and subtalar arthroscopy and 38 patients treated with the same traction device during supine ankle arthroscopy. Conclusion: Minimally invasive skeletal traction can be used safely for prone posterior ankle and subtalar arthroscopy.
Level of Evidence: IV, Retrospective Case Series
Introduction
Posterior ankle and subtalar arthroscopy with the patient in the prone position can be a challenging endeavor due to the limited amount of working space and the small joint space available. Several authors have detailed the technique for posterior ankle and subtalar arthroscopy.1,9 One limitation of this technique is the difficulty in obtaining joint distraction in the prone position. Traction facilitates entry into both the ankle and subtalar joints, and may allow for better visualization. Several methods of distraction have been described in the literature for supine ankle arthroscopy.2,4,5,8,10 To the author's knowledge there are no reports of using a distraction technique for prone posterior ankle and subtalar arthroscopy. We describe a minimally invasive technique for obtaining distraction across both the ankle and subtalar joints for use in prone posterior ankle and subtalar arthroscopy utilizing a transosseous calcaneal wire.
Technique
A majority of our patients receive a preoperative regional popliteal block and a general anesthetic for the procedure. A general anesthetic is likely to facilitate distraction due to muscular relaxation. A tourniquet is placed over the proximal thigh. We have found that intraoperative use of a tourniquet is rarely needed for either ankle or subtalar joint arthroscopy from a posterior approach, but one is placed in case arthroscopic visualization is impaired by bleeding that cannot be controlled by maintenance of adequate inflow pressure with similar pressures being used as for anterior arthroscopy. The use of a pressure/flow sensing arthroscopic pump is helpful to maintain good visualization. A standard operative table is utilized. The patient is positioned prone with the knees just proximal to the distal bed crease. The foot of the bed is lowered. The contralateral limb is flexed at the knee and held in this position with the use of a padded lateral post. Care is taken to pad the knees well (Figure 1). The patient is prepped and draped below the knee.

Intraoperative image shows the positioning of the contralateral limb in flexion and attached to a vertical post that stabilizes the limb and keeps it away from the surgical side.
The posterior tuberosity of the calcaneus is palpated and the appropriate wire insertion site is identified on the medial aspect of the calcaneus. 3 The 1.8-mm wire is positioned on the inferior aspect of the tuberosity so as to avoid the medial neurovascular structures. The wire should be drilled parallel to the plantar aspect of the foot and once the wire has breached the lateral calcaneal cortex a mallet is used to complete the advancement of the wire in order to avoid thermal necrosis or entrapment of local structures. The wire must be posterior and inferior to the medial neurovascular bundle and the use of a small diameter wire decreases the likelihood of injuring the medial calcaneal branch of the tibial nerve that can be encountered in this area of wire insertion. More posterior placement of the wire brings the ankle into a dorsiflexed position upon distraction and thereby further improves arthroscopic visualization of the central and anterior aspects of the talus.
The wire is attached to a reusable Taylor spatial frame foot plate. A half ring or Bohler's frame can also be utilized, however this leaves little room between the plantar aspect of the heel and the ring making manipulation of the foot difficult and leaving the surgeon with less working area about the hindfoot. The wire is tensioned to 90 pounds and a traction frame system is attached to the operative table with a “C” clamp and also attached to the foot plate with an “S” hook. Alternatively, a modified traction bale can be applied. Sterile drapes are applied around the distractor and the foot plate or traction bale (Figure 2). The typical time for placement of the pin and application of the foot plate and traction apparatus is roughly five minutes. A spring tension device was initially used to measure the amount of traction force applied, but that practice was discontinued as no ill effects of sustained high tension traction were observed in our patients. Traction is added relatively quickly and can be adjusted throughout the procedure.

A mini C-arm is typically utilized to optimize portal placement in order to assure proper visualization (Figure 3). The traction apparatus allows for easy positioning of the mini C-arm. By removing the bulk of the table around the operative limb, simultaneous arthroscopy and fluoroscopic visualization are achieved which facilitates efficient surgery (Figure 4).

Operative image demonstrates easy use of a mini C-arm around the freely suspended operative leg.
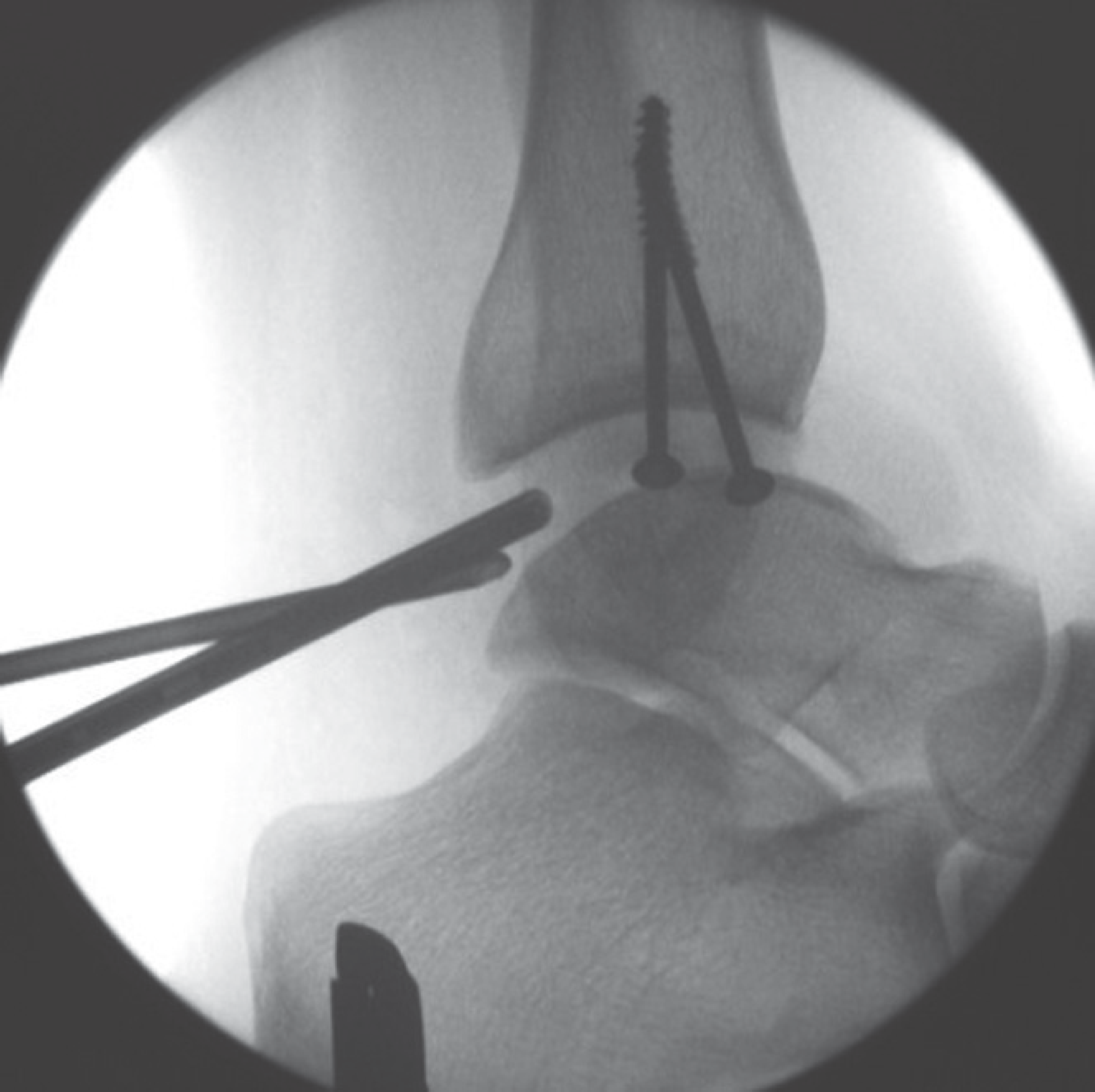
Lateral fluoroscopic image demonstrating the amount of distraction conferred by the traction device.
Results
Clinical results were reviewed after approval was obtained from the institutional review board. Fourteen patients undergoing posterior ankle or subtalar arthroscopy have been treated with this technique, and none have had complications related to the method of distraction. No wires have pulled out and no pin tract complications have been observed. No sural nerve injuries have occurred. Specifically, the authors have not identified problems with nerve dysfunction as a result of wire placement or the high tension traction. Visualization of the posterior aspect of the ankle joint has been excellent with a relatively large intra-articular working area (Figure 5).
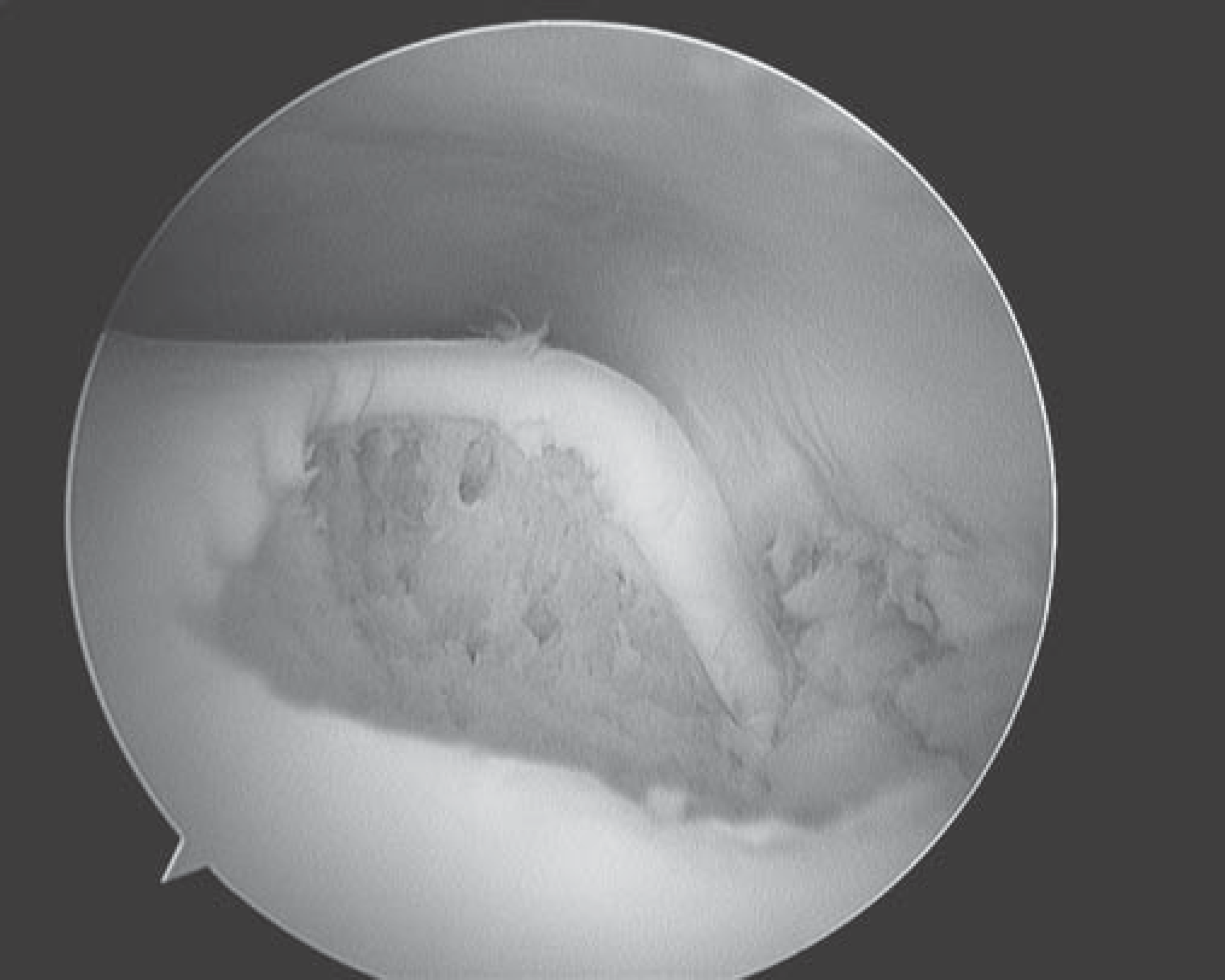
View of posteromedial talus defect with skeletal distraction.
The posterior facet of the subtalar joint was well visualized but there exists a smaller actual working area within the joint (Figure 6). In addition to the 14 treated with this traction technique, an additional 38 patients have had this technique utilized while undergoing ankle arthroscopy in the supine position. Visualization subjectively is improved over cases done without skeletal traction and no complications have been encountered in this group of patients. The authors do not claim to have increased the distraction of either joint in comparison to other techniques but do find this method of limb control under traction facilitates safe and effective visualization of both the posterior subtalar and ankle joints.

View of posterior facet of subtalar joint with burr in place during subtalar debridement for fusion.
Discussion
Posterior ankle and subtalar arthroscopy is a challenging but useful technique with the potential to treat intra-articular pathology that has historically been treated with use of larger open approaches. The main advantage of our minimally invasive distraction technique is the relatively larger working area provided to the surgeon within the ankle joint as a result of the traction created and thereby achieving the ability to address posterior talar lesions often difficult to visualize completely due to the architecture of the dome of the talus. Additionally, when correctly applied, the surgeon is able not only to perform arthroscopic procedures but also has the freedom to obtain fluoroscopic imaging and place internal fixation without manipulating the leg.
One published report describes the working area in prone arthroscopy of the subtalar joint without distraction to be 43% of the posterior facet. 9 To address the difficulty with visualization of the posterior facet of the subtalar joint, different portal options have been studied. 7 It is possible that this new technique increases the visualized area as well as the area available to work, however this has not been fully evaluated and no quantitative measurements were made. In some cases, particularly in patients with prior calcaneal fractures and loss of hindfoot height, subtalar joint distraction appears increased in comparison to non-traction methods of visualization. One concern raised in the literature is the effect of traction on nerve function for an extended period of time. We have applied our technique for procedures lasting 2 hours and have not observed any transient or long-term effects on peripheral nerve function. Transient nerve disturbances potentially may also be caused by direct nerve compression created by the straps utilized for noninvasive traction techniques; the potential for this is well documented. 6
Conclusion
The authors present a method of minimally invasive distraction that can be applied to both the ankle and subtalar joints from the posterior approach. The method has been used in fourteen patients and no complications have been encountered.