
Abstract
Level of Evidence: V, Expert Opinion
Introduction
Dislocation of the metatarsophalangeal joint (MTPJ) of the toe is a rare injury. Irreducible dislocation of an MTPJ of the lesser toe is much rarer. In our review of the literature there were only three case reports. We are reporting a case of an irreducible traumatic dislocation of the MTPJ of two toes. A pathomechanics study was performed with an amputated lower extremity.
Case Report
A 21-year-old man was injured in a motor vehicle crash. The car hit a fence and his legs were crushed between the front and back seats. His left foot was swollen but no apparent deformity was noted (Figure 1). No neurovascular deficit was observed.

3D reconstructed CT view; left side is affected side.
X-rays of the left foot showed a nondisplaced fracture of the third metatarsal base and dorsal dislocation of the fourth and fifth MTPJ. The fourth and fifth metatarsal heads were displaced plantar-medially without fracture (Figure 2). Closed reduction was initially attempted under digital block by hyperextending the toes and applying pressure against the bases of the phalanges in the Emergency Department but failed. We performed a computer tomography (CT) to investigate possible causes of this failed reduction. The CT revealed that the metatarsal head was trapped between the lumbrical and flexor digitorum tendon (Figure 3). We decided to reduce the fourth and fifth metatarsophalangeal dislocations surgically.
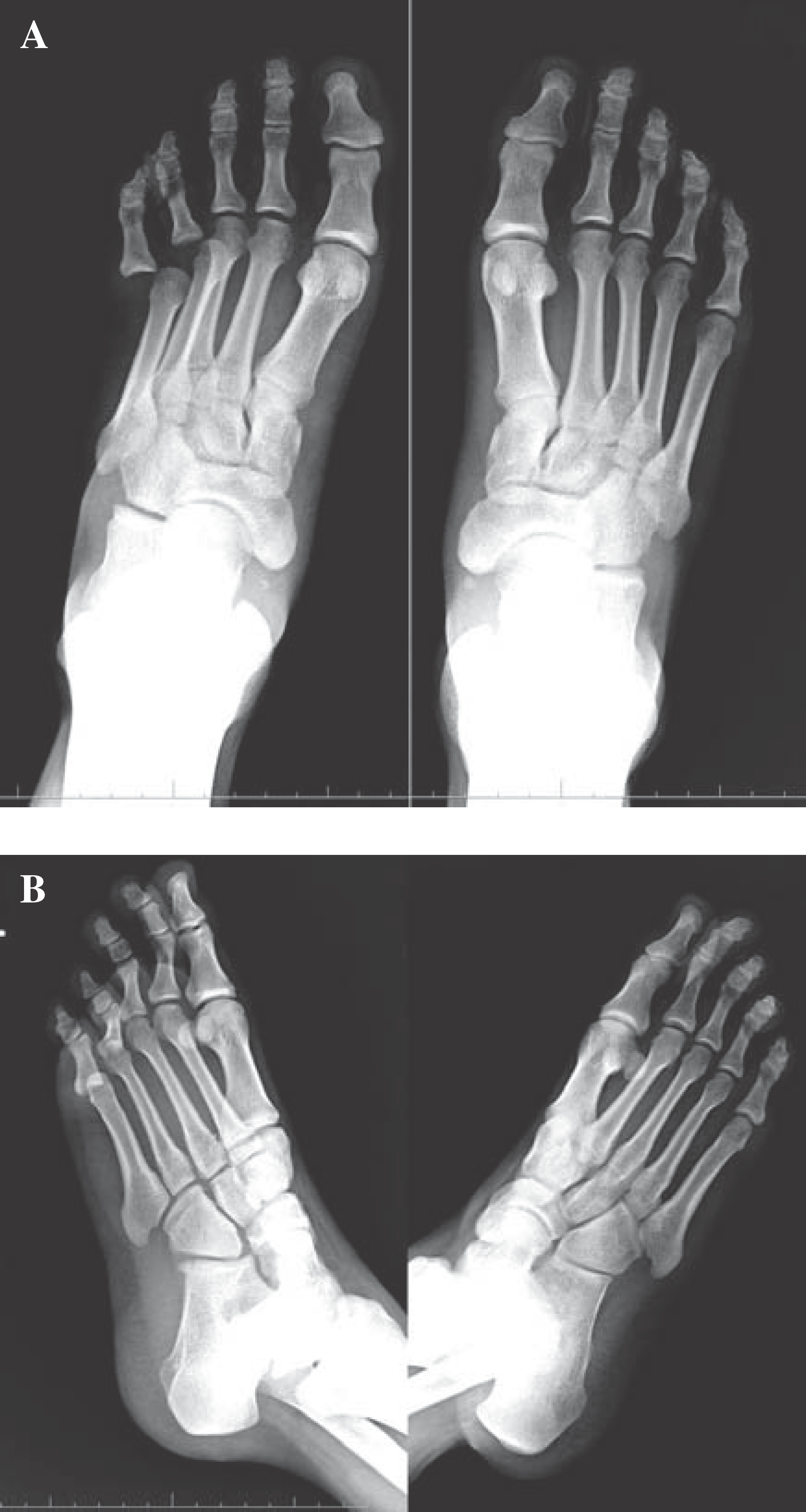
AP (A) and oblique (B) injury radiograph.
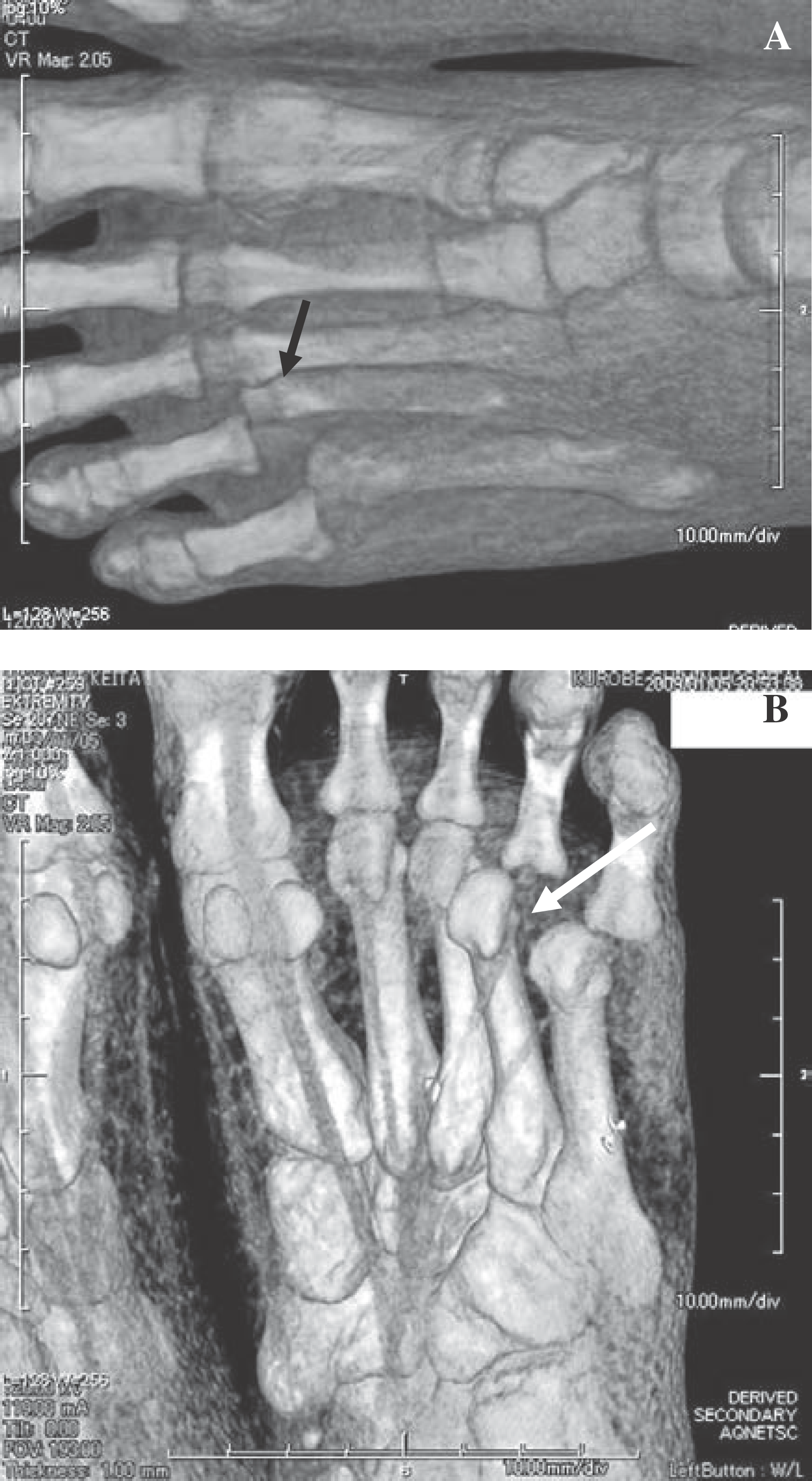
3D reconstructed CT view.
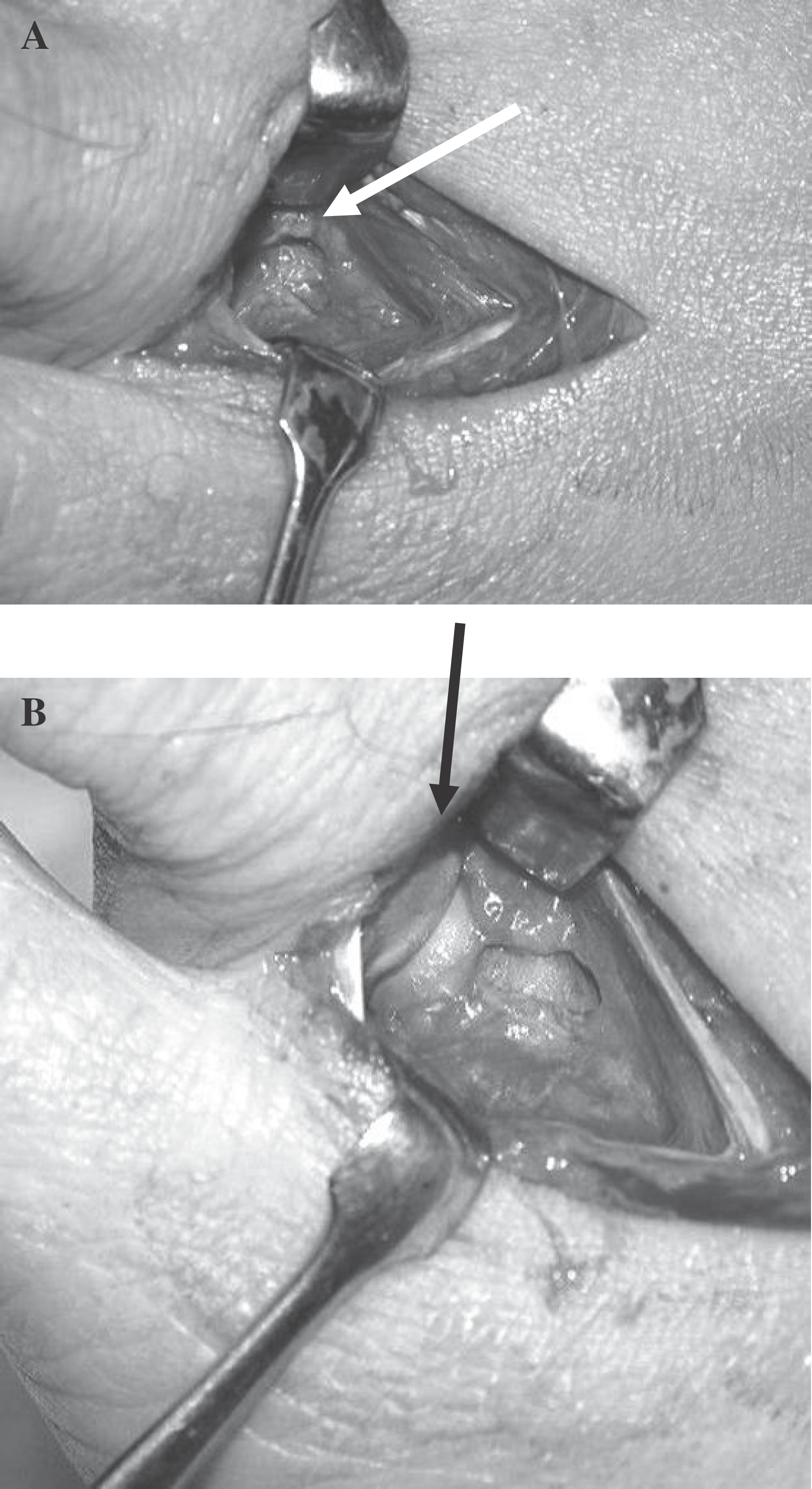
Under general anesthesia the MTPJ were exposed by making a dorsal longitudinal incision between the fourth and fifth metatarsals. The fourth extensor digitorum longus tendon was split. The lacerated fibrocartilagious plate and fourth lumbrical tendon were found to be coursing over the fourth metatarsal head from the medial side (Figure 4). The dorsal capsule was divided on the lateral side of the dislocated lumbrical tendon. By forcibly pulling the fibrocartilagious plate and lumbrical tendon medially, the MTPJ was anatomically reduced with ease (Figure 5). The fifth MTPJ was then reduced via closed manipulation (Figure 6).

Pre-reduction: white arrow is lumbrical tendon and fibrocartilaginous plate.
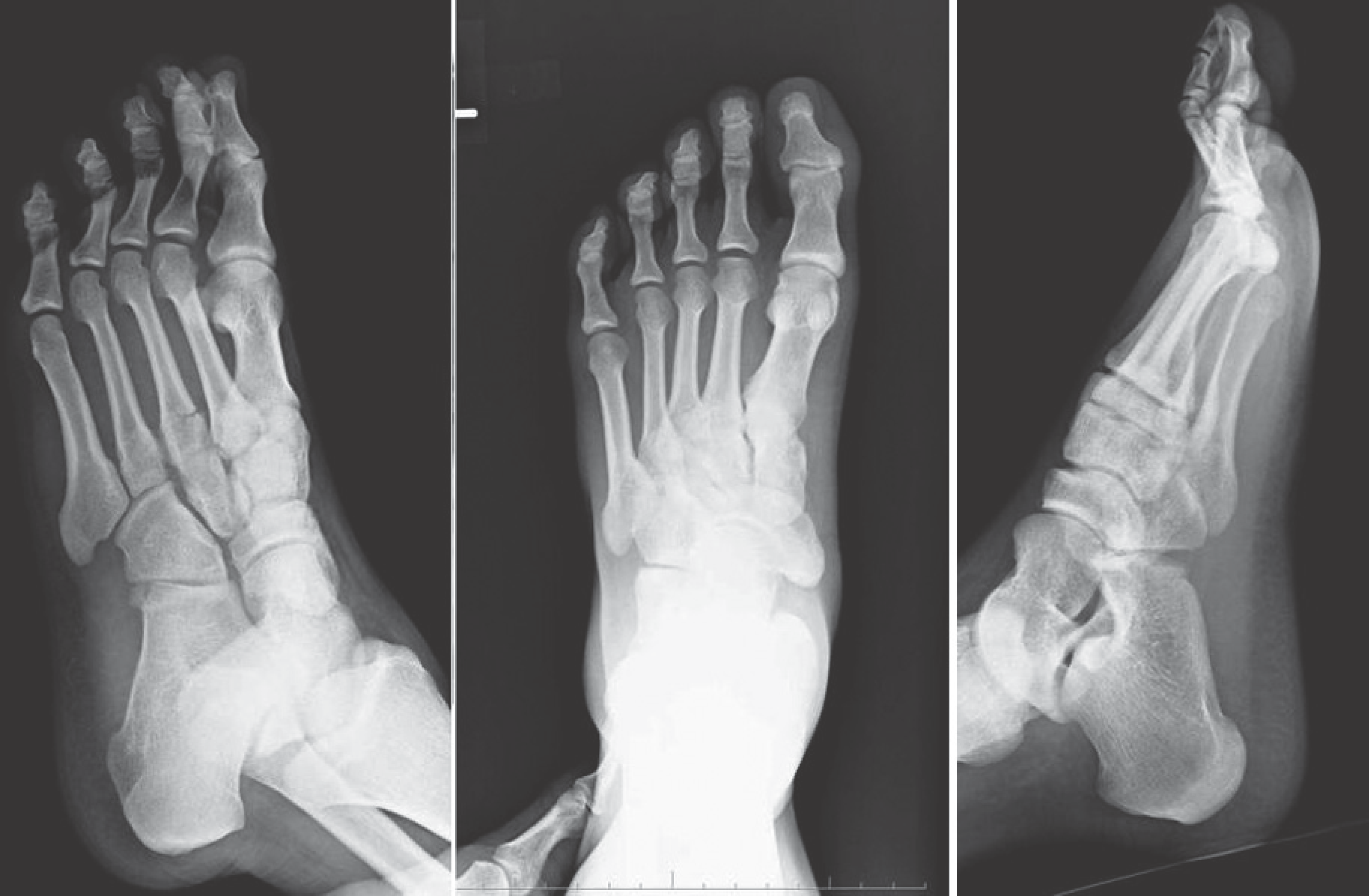
Postoperative X-ray.
Anatomical study of pathomechanics
We performed an anatomical study of the pathomecanics of an MTPJ with an irreducible dislocation by using the amputated lower leg of an 84-year-old woman. We attempted to create a closed dorsal dislocation of the MTPJ but failed. After a dorsal skin incision was made and the fourth extensor digitorum tendon split, a very thin dorsal capsule was exposed (Figure 7A). The dorsal capsule was split but forced dorsiflexion would not cause an MTPJ dislocation. Therefore, we performed a plantar approach where the flexor tendon sheath was split and the fibrocartilaginous plate was exposed (Figure 7C). After the medial side of the fibrocartilaginous plate was split, the MTPJ was dislocated dorsally and the metatarsal head was trapped between the lumbrical and flexor digitorum longus tendon (Figure 7, B and C).
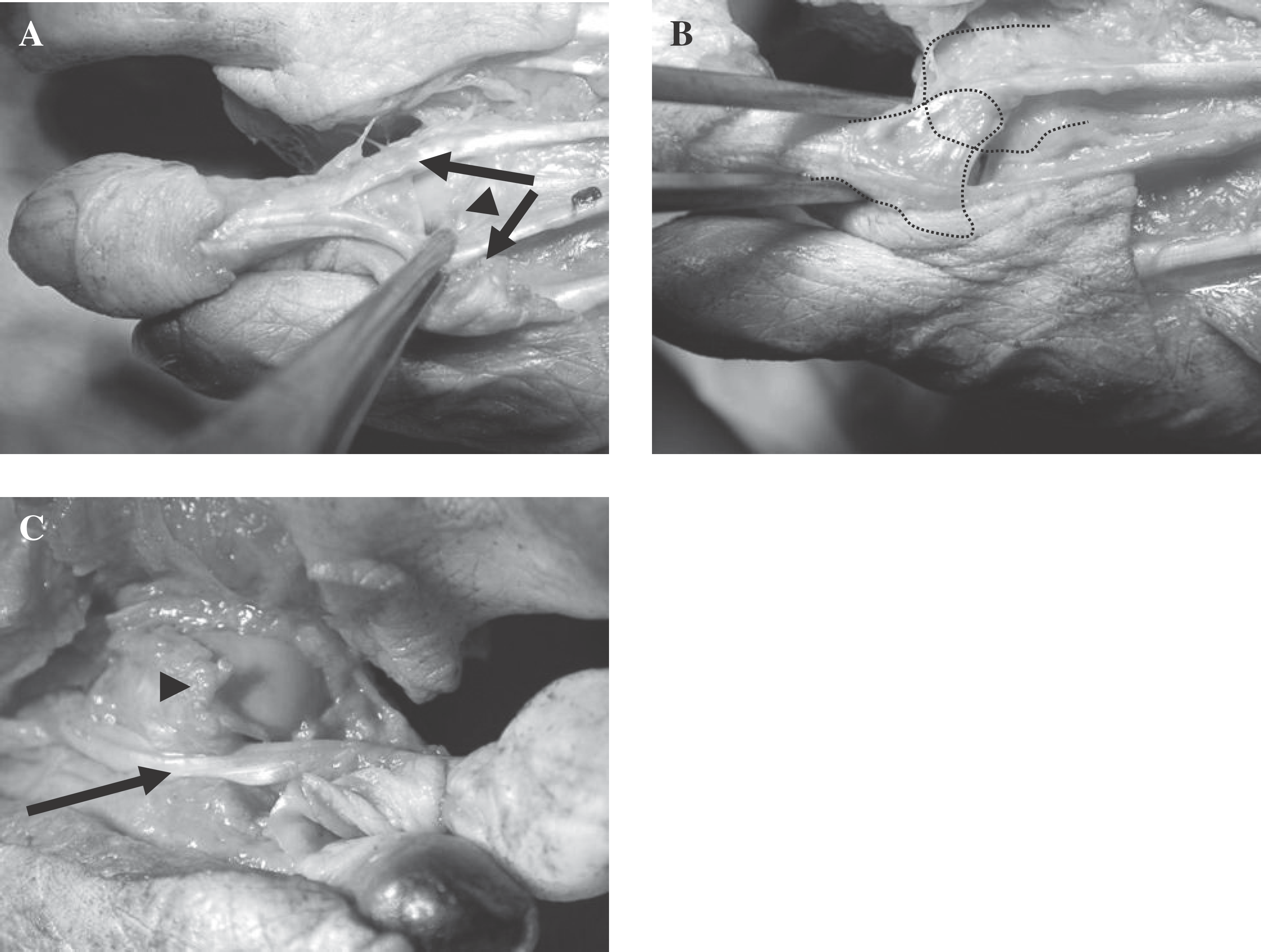
Anatomical study.
Discussion
The majority of dislocations of MTPJ's can be reduced by closed manipulation. There are various causes of irreducibility. Rao and Banzon found in their case report that the fibrocartilaginous plate was the main obstacle to closed reduction. 3 They needed to divide the deep transverse metatarsal ligament and the fibrocartilaginous plate by a dorsal approach. Hynes et al. reported that the obstacle to reduction was the flexor digitorum longus tendon. 1 At open reduction, the flexor digitorum longus tendon was reduced by a dorsal approach. Nakano et al. reported that the deep transverse metatarsal ligament interfered with the manipulative reduction. A plantar approach was used to suture repair the deep transverse metatarsal ligament. 2 However, in our case, the fibrocartilaginous plate and lumbrical tendon were the main obstacles to successful closed reduction. By forcibly retracting the fibrocartilaginous plate and lumbrical tendon medially through a dorsal approach, the metatarsal head was reduced. Although with a dorsal approach we could not suture the torn fibrocartilaginous plate, the MTPJ did not have gross instability.
The pathomechanics of this injury were evaluated by an anatomic dissection of an amputated lower extremity. Without laceration of the fibrocartilaginous plate, an MTPJ dislocation could not be induced. Forced dorsiflexion of the proximal phalanx over the metatarsal head caused a tear of the fibrocartilaginous plate. The metatarsal head was forced through the fibrocartilaginous plate, trapping it between the fibrocartilaginous plate medially and the flexor digitorum longus laterally. We believe this is why the closed reduction of the MTPJ was not successful and deviation of the fourth and fifth metatarsal head occurred in the absence of fracture. This case and anatomic study suggest it would be difficult to reduce by closed manipulation a trapped fibrocartilaginous plate which is forcing the malalignment of the metatarsal bone in the absence of fracture.
Conclusion
The trapped metatarsal head between the fibrocartilaginous plate and lumbrical and flexor digitorum longus tendon prevented the MTPJ from undergoing successful closed reduction.
Dislocation of an MTPJ with malaligned metatarsal bone(s) needs an open reduction of a trapped metatarsal head.