
Abstract
Background: Lesser toe deformities are frequent and bothersome conditions. Many options exist for the treatment of hammertoes and clawtoes. The purpose of this study was to review our experience with the use of an intramedullary fusion device. Materials and Methods: An IRB approved retrospective review was performed to identify 38 toes in 27 patients treated with the StayFuse™ (Nexa Orthopaedics) device with a mean followup of 31 months. The indications for surgery were primary deformity in 12 toes and recurrent deformities in 26 toes. Results: Union occurred in 23 of 38 (60.5%). The union rate was nine of 12 for primary procedures and 53.8% (14/26) for revisions. Coronal PIP alignment demonstrated no change in 33 of 38 cases (86.8%) and changed in five of 38 (13.2%). Sagittal PIP alignment demonstrated no change in 36 of 38 cases (94.7%), and changed in 2/38 (5.3%). Including nonunion, the overall complication rate was 55.3% (21/38) (15 nonunions; three hardware failures (two (bent) not requiring intervention and one (broke) leading to a rotational deformity requiring revision), one intraoperative fracture (without sequelae), one requiring MP surgery, and one requiring a larger implant. The index surgery for all three of the patients that required a second surgery was for a recurrent deformity. All three patients requiring a second surgery occurred in the nonunion group. Conclusion: The StayFuse™ intramedullary fusion device was efficacious in maintaining PIP alignment in the treatment of lesser toe deformities with a relatively low reoperation rate at mid-term followup.
Level of Evidence: IV, Retrospective Case Series
Introduction
Lesser toe deformities are frequent and bothersome conditions which increase with age. Many options exist for the treatment of hammertoes and clawtoes, ranging from nonoperative to operative means. Surgical management of these deformities is one of the most common procedures performed on the forefoot. 7
Many operative options have been created in attempt to address some of the known short-comings, such as nonunion, displacement, hardware failures, and infections. These include resection arthroplasty, arthrodesis with pins, wires, screws, bone dowels, bioabsorbable pins, digital implants and tendon transfers.1,9,12,14–16,24,27,28 Proximal interphalangeal (PIP) joint arthrodesis has several advantages, including a decreased risk of recurrence and a more predictable toe posture. 16
Here we report on the use of a two-piece intramedullary fusion device. This device may be used to perform proximal interphalangeal joint arthrodesis for hammertoes or clawtoes, however, the efficacy and complications associated with this device have not been previously reported. The purpose of this study was to review our experience with the use of an intramedullary fusion device.
Materials and Methods
An IRB approved retrospective review was performed on 38 toes in 27 patients treated with the StayFuse™ (Nexa Orthopaedics, San Diego, CA) device between 2003 and 2007. Thirty-five patients (47 toes) were identified and five patients (six toes) declined to participate in the study, two patients died, and one patient was lost to followup. There were 23 females and four males with a mean age of 62 years. The indications for surgery were primary deformity in 12 toes (seven hammertoe and five claw toe) and recurrent lesser toe deformities in 26 toes (24 recurrent deformity after previous surgery and two symptomatic nonunions). Associated diagnoses included inflammatory arthritis (four), post-traumatic (two), neuromuscular (two). Surgeries were performed on the second toe in 25 cases and the third toe in 13. One patient had bilateral arthrodeses performed, while all others were unilateral. The mean duration of radiographic followup was 31 months (11 to 58 months).
Outcomes measured included union (presence of bridging bone across the PIP joint clearly visible on radiographs) and alignment (between proximal and middle phalanx axis). Alignment was graded as no change or change (greater than 10 degree change from intraoperative radiographs) on postoperative radiographs in both the AP and lateral plane. However, it should be noted, that measurement of alignment on lateral views was difficult due to adjacent toe overlap. We considered greater than 10 degrees change on final postoperative radiographs as unacceptable. We also reviewed the rate of implant failure and other complications.
Surgical technique
A 1.5-cm longitudinal incision was made over the dorsum of the PIP joint. A longitudinal incision was preferred to obtain adequate exposure for bone preparation and placement of the implant. In the event of a revision situation where a transverse incision had been created, the surgeon used either the prior incision or created a new longitudinal one. It was our preference in this scenario, however, to use a new longitudinal incision. The extensor tendon was split and reflected. A transverse capsulotomy was performed with release of the collateral ligaments. The head of the proximal phalanx and base of the middle phalanx was resected creating two parallel planes, each perpendicular to the axis of the canal. The total amount of bone removed was approximately 6 to 8 mm but this was variable and often determined by the length of the adjacent toe, prior surgical procedures or extent of the fixed deformity. The majority of patients in this series were revision situations in which substantial bone had already been removed. In these instances, fibrous tissue was removed and the bone ends were freshened with a ronguer.
The device utilized in this hammertoe surgery consisted of two parts which were linked together. Both the proximal phalanx and middle phalanx sections have a screw-in side for purchase into bone. The other end of the part has either a “female” receptacle (proximal phalanx) or “male” prong (middle phalanx) to engage. The location of the intramedullary canal on both sides of the arthroplasty was determined, often using a 1.25-mm pin directed under fluoroscopic imaging. Next, the appropriate size pilot drill was chosen for the targeted phalanx. The pilot drill was manually placed at a 90-degree angle to the resected surface and kept within the central part of the canal as confirmed by imaging. The drill was advanced until the shoulder stop. Proper toe length and alignment was verified. The parts were placed into their respective sides after first tapping and making certain the tap was appropriately aligned on fluoroscopic imaging. The part was advanced into bone until the screwdriver disengaged such that the locking mechanism was at the level of the joint line. The implants came in three different diameters for both the proximal and middle phalanx. The most common size used was the 2.8-mm proximal and 3.8-mm middle. The size determination was based on tapping. The middle phalanx had a minimal length of 6 mm, thus the need for at least that much remaining bone in revision situations. The two sides were then engaged until the components snapped into place and the bones were approximated. Proper engagement was verified with probing of the osteotomy site and inspection with intraoperative fluoroscopy. An average cost for the implant was $225 per set.
Postoperative management consisted of immediate weight-bearing in a hard-soled sandal and suture removal at 2 weeks. Thereafter, activity and shoe wear was advanced as tolerated by the patient.
Results
Overall, union occurred in 23 of 38 toes with a union rate of 60.5% (Figure 1). PIP alignment demonstrated no change in either the coronal or sagittal plane in 31 of 38 cases (81.6%). Coronal PIP alignment demonstrated no change in 33 of 38 cases (86.8%) (Figure 1) and changed in five of 38 (13.2%), two in the primary group and three in the revision group. Sagittal PIP alignment demonstrated no change in 36 of 38 cases (94.7%), and changed in two of 38 (5.3%), both in the revision group. Neither of these two patients with changes in the sagittal plane required further intervention. The average sagittal metatarsal-fused phalangeal angle was 17.3 degrees (range, 0 to 31).

Postoperative radiograph demonstrating fusion and maintenance of alignment.
For the primary procedures, union occurred in 9 of 12 toes (75%). The coronal alignment changes that occurred in the primary procedure group (2/12) (16.7%) did not require further intervention, even though one did not demonstrate radiographic union (Figure 2, second toe), while the other was not associated with displacement of the fusion (Figure 3).
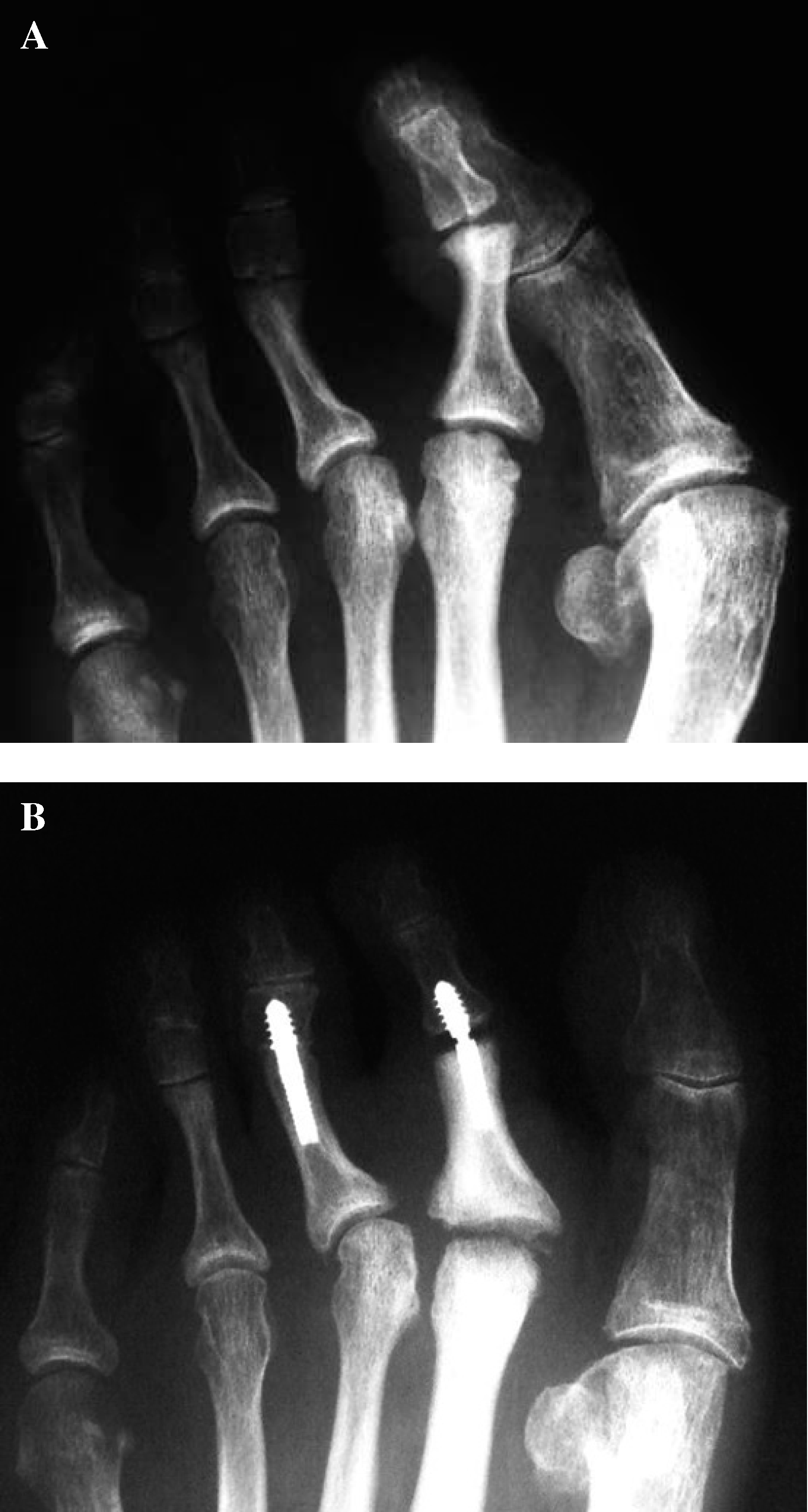
Preoperative (A) and postoperative (B) radiographs. The postoperative radiograph demonstrates change in alignment and nonunion of the second toe which did not require intervention.

Postoperative radiograph demonstrating hardware failure and loss of alignment requiring revision surgery.
For the revision procedures, union occurred in 14 of 26 toes (53.8%; p = 0.12 when compared to the primary group). Of the alignment changes that occurred in the revision group (three coronal; two sagittal), three of 26 (11.5%) required a second surgery to obtain correction. The first patient required a surgery on postoperative day 16 due to the components becoming loose within the canal. This was revised by switching to a larger component. The second patient required a second surgery due to hardware failure resulting in a rotational deformity, and was returned to surgery 7 weeks postoperatively to correct the rotational malalignment (Figure 4). The third patient had a cock-up deformity and proceeded to have a metatarsophalangeal release and Weil osteotomy to obtain satisfactory results.

Postoperative radiograph demonstrating hardware failure, loss of alignment, but eventual fusion.
Including nonunion, the overall complication rate was 55.3% (21/38) (15 nonunions; three hardware failures (two bent not requiring intervention and one broke leading to a rotational deformity requiring revision), one intraoperative fracture (without sequelae), one requiring MP surgery, and one requiring a larger implant. The index surgery for all three of the patients that required a second surgery was for a recurrent deformity. There was one intraoperative complication (middle phalanx fracture) that healed uneventfully. In summary, four of five of the complications and all three (7.9%) patients requiring a second surgery occurred in the nonunion group.
Discussion
PIP joint arthrodesis is a reliable method to correct lesser toe deformities. There are a multitude of techniques available to achieve deformity correction, each with its advantages and disadvantages. Kirschner wires, screws, implants, pegs, and bioabsorbable pins have been used to maintain stability until a solid arthrodesis occurs.1,9,12,14–16,24,27,28 Complications after PIP joint arthrodesis are not uncommon. Baig et al. has described DIP joint instability or deformity in 21% of toes 6 months after surgery, resulting in a 50% reoperation rate. 2 Coughlin demonstrated that 13% of patients developed a hyperextension deformity of the PIP joint 5 years after arthrodesis and 23% of the toes were noted not to have ground contact with the toe pulp. 8 Although the purpose of this study was to report radiographic outcomes of this device, in an effort to evaluate toe position, we measured the sagittal axis as well and noted only a 5% change (two patients), both in minor flexion at the PIP joint which did not require further 5 intervention.
The use of an intramedullary fusion device has several advantages. First, there is no exposed instrumentation, such as a Kirschner wire. This is more convenient and less painful for the patient since it cannot become caught or stubbed. In addition, the surgeon does not have to worry about a Kirschner wire becoming loose. Most importantly, the absence of a Kirschner wire may reduce the risk of infection as no hardware is exposed. The technique utilized in the current study may reduce these above risks. Another potential benefit is that there is no violation of a healthy joint surface. However, this device is more costly, especially when compared to a Kirschner wire, which at our institution costs approximately $9.
Malalignment is another factor associated with unsuccessful results, reported by many authors at rates up to 50%.5,7,9,10,16,19 In our series, radiographic PIP alignment was maintained in 81.6% of patients, and 4 of 7 patients that experienced mild changes were unaware clinically. Thus, three of the seven patients with PIP alignment changes (all in the coronal plane) required further surgical intervention.
Hardware issues and removal are also common following PIP arthrodesis. Intramedullary instrumentation, such as a screw, has been reported; however, seven out of 51 (14%) had to be removed because of screw head prominence. 22 In our series, no patients required or requested hardware removal.
Our union rate was 61%, but our PIP malalignment rate was only 18.4% at an average of 31 months, demonstrating the importance of stable and durable fixation. Although the revision group had a lower overall union rate of 58%, PIP alignment was maintained in 21 of 26 (80.8%) toes. Only 3 patients (8% of the study group) had a second surgery, which is considered low in the literature. All 3 of these patients were undergoing a revision PIP arthrodesis at the time of the StayFuse™ placement. As a technical tip, we recommend the use of intra-operative fluoroscopy to insure proper positioning and seating of the device.
The implant bent in two patients, requiring surgical intervention in only one of them. The implant broke in one patient also requiring revision. The majority of the complications and all three patients requiring a second surgery occurred in the nonunion group. One possible theory is that these patients did not have the implant fully seated and thus had a greater degree of distraction between bone ends. However, longer-term followup, especially in the nonunion group and pseudoarthrosis group is necessary, as patients may become more symptomatic in the future.
Limitations of our study are that it is retrospective and only includes radiographic outcomes. However, the purpose of this study was to review our experience with the use of an intramedullary fusion device, which has not yet been reported.
The StayFuse™ intramedullary fusion device is efficacious in maintaining PIP alignment in the treatment of lesser toe deformities with a relatively low reoperation rate at mid-term followup. Overall alignment was maintained in 82% of patients while coronal and sagittal alignment was maintained in 87% and 95% of patients, respectively. No patients required a second surgery due to hardware pain, which is an advantage with this device. Long-term followup studies will be necessary to further evaluate the final outcome of PIP arthrodesis utilizing this technique.
Footnotes
Acknowledgments
The authors would like to recognize Amy Eshelman, BS and Susan Odum, MEd for their assistance in preparation of the manuscript and statistical analysis.