
Abstract
Background: Ankle syndesmosis fixation is often employed with the utilization of many variable methods and implants. Complications secondary to trans-syndesmotic fixation have been described, yet the proximity of a single trans-syndesmotic screw to the perforating branch of the peroneal artery (PBPA) has not. Materials and Methods: Sixteen cadaveric legs received a single trans-syndesmotic screw using standard AO technique. The PBPA was identified and the following distances were measured using photographic images and morphometric software: the tip of lateral malleolus to the PBPA, the tibial plafond to the PBPA, tip of lateral malleolus to the screw, and the PBPA to the screw. Average distances were calculated and statistically compared. Results: The location of the trans-syndesmotic screw inserted 2 cm proximal to the tibial plafond was on average less than 1.3 cm proximal to the PBPA. In six out of the 16 specimens, the screw was less than 1 cm from the PBPA. In one specimen, the screw came within 0.22 cm of the PBPA. Conclusion/Clinical Relevance: The placement of trans-syndesmotic fixation places the PBPA at risk. In order to avoid injury to the PBPA with trans-syndesmotic fixation, fixation should be avoided 2.3 to 4.1 cm proximal to the tibial plafond, 4.5 to 6.2 cm proximal to the tip of the lateral malleolus in females and 2.8 to 5.9 cm proximal to the tibial plafond or 5.1 to 7.2 cm proximal to the tip of the lateral malleolus in males.
Introduction
Ankle fractures comprise one of the most common injuries treated by orthopedic surgeons.29,47 In up to 13% of all ankle fractures11,26 and in 20% of patients requiring internal fixation,22,38 an associated syndesmotic injury will be present. In managing an ankle fracture, anatomic reduction of the lateral malleolus and syndesmosis remains essential for maximizing patient outcome.9,25,29,47 Yet despite years of accumulated experience and several biomechanical and clinical reports, a lack of consensus on the indications and technical aspects of ankle syndesmotic screw insertion remains. 47 Currently, controversies involving ankle trans-syndesmotic fixation include: implant selection and position, position of the ankle joint during syndesmotic fixation, and the need for implant removal. 48 In spite of such debate, syndesmosis screw fixation is often employed 6 with many methods. 30 While the stabilization of syndesmotic ruptures at the time of fracture fixation remains the standard method of treatment in ankle injuries 20 and has yielded reports of satisfactory outcome,20,21 the complications of decreased range of motion, screw loosening or breakage, syndesmosis widening, syndesmosis malreduction, tibiofibular synostosis, osteolysis, and degenerative osteoarthrosis are real.29,31 To our knowledge, no study exists to support the safety of ankle trans-syndesmotic screw fixation in relationship to the perforating branch of the peroneal artery (PBPA). Therefore, the principal goal of this study was to assess the potential risk to the PBPA with ankle trans-syndesmotic screw placement.
Anatomy
After originating from the posterior tibial artery, the peroneal artery descends along the medial crest of the fibula in a fibrous canal between the tibialis posterior muscle and the flexor hallucis longus muscle or within the flexor hallucis muscle.1,37 The PBPA then arises within the flexor hallucis longus muscle and pierces the interosseous membrane between the tibia and fibula above the tibiofibular syndesmosis. 46 After its emergence into the extensor compartment, the PBPA gives a relatively constant skin perforator which supplies a large area on the lateral aspect of the distal one third of the leg 1 The PBPA then descends anterior to the lateral malleolus to be distributed to the anterolateral part of the ankle and the tarsal region. 44 The anastomosis of the PBPA and the lateral malleolar branch of the anterior tibial artery create the malleolar anastomosis. 44 Then the anastomosis between the PBPA and the lateral tarsal artery of the dorsalis pedis create the artery of the tarsal sinus, which merges with the artery of the tarsal canal to supply most of the talar neck and head. 32
Materials and Methods
After receiving appropriate institutional approval, 16 embalmed human cadaveric lower extremities were obtained. All specimens were right sided and had no observable leg, ankle, or foot pathology after thorough dissection. Of the 16 specimens, seven were female with a mean age of 83 (range, 74 to 100) years and nine were male with a mean age of 80 (range, 53 to 94) years. The anterior soft tissues were removed exposing the distal tibial and fibula while preserving all ligamentous structures. An anterolateral capsulotomy of the tibiotalar joint was performed with subsequent anterior capsulectomy to provide full visualization of the anterior tibiotalar joint orientation. In accordance with standard AO technique, 33 a metallic, 4.5-mm in diameter, and 45-mm in length, cortical screw (Synthes, Paoli, PA) was placed across the syndesmosis in all specimens in a randomized sequence by one examiner. The inserted screws were fully threaded and self-tapping. Prior to screw insertion with the second ray axis of each specimen perpendicular to the floor and the ankle in neutral position, a 3.2-mm drill-bit was centered on the lateral aspect of the fibula to avoid iatrogenic fracture of the bone. Then the drill was used to create drill holes in both fibular cortices and the lateral tibial cortex. Tricortical screw fixation was achieved by inserting the screw 2 cm proximal and parallel to the tibiotalar joint in the coronal plane. According to McBryde et al., 28 syndesmotic screw placement 2 cm proximal to the tibiotalar joint appears to be a biomechanically reasonable position. In the transverse plane, the screw was oriented to follow a 30-degree oblique direction from posterolateral to anteromedial using a custom fabricated apparatus that would allow reproducible insertion technique. Positional fixation was achieved and compression was avoided by tightening the screws to only firm, two-finger tightness. Once the screws were inserted, a 6-inch, portable c-arm (Fluoroscan, Northbrook, IL) was used to obtain anteroposterior, lateral, and mortise views of the ankle to ensure accurate screw placement (Figure 1). Throughout specimen preparation and experimentation, specimen moisture was maintained with towels soaked with saline and polyethylene wrap.

Ankle mortise fluoroscopic image of a trans-syndesmotic screw.
Central to this investigation was the accurate measurement of the relationship of the PBPA to the trans-syndesmotic screw and other bony features, including the tibial plafond and the tip of the lateral malleolus. The measuring techniques were carried out by leaving the trans-syndesmotic screw in place and performing detailed dissection of the vasculature around the ankle. Once the PBPA was located, the vessel was traced proximally and distally to verify its identification. The PBPA was protected as a rongeur and curettes were used to remove part of the fibula anterior to the screw to facilitate visualization.
All the specimens were then photographed with a Fujifilm S1 Pro digital SLR camera (6.13 mega-pixels) (Fuji, Tokyo, Japan), outfitted with an AF Micro Nikkor 105 mm lens (Nicon, Tokyo, Japan). The photographs were taken with the camera mounted on a tripod and under normal fluorescent lighting. Each specimen was photographed multiple times in one lateral and two anterior views at the maximum distance possible from and perpendicular to the specimen to minimize distortion, while also capturing all anatomic landmarks of interest and a metric scale in the image.
The digital images (3040 × 2016 pixels) to be measured were selected on the basis of clarity in resolution and the inclusion of all anatomic landmarks of interest. Next, measurement guidelines were placed on the digital images using PowerPoint software (Microsoft, Redmond, WA) and subsequently exported as JPEG files. Then the measurement guidelines on the JPEG files were measured using the morphometric software ImageJ 1.41o (Wayne Rasband, NIH, USA). The scale was calibrated in pixels for each JPEG, and ImageJ calculated distances to the nearest 0.001 cm. The following relationships were measured with the ImageJ software:
the distance from where the most distal aspect of the PBPA perforates the interosseous membrane to the most proximal aspect of the threads along the screw shaft (ARTSCREW) measured parallel to the shaft of the fibula in anterior view (Figure 2). the distance from the tip of the lateral malleolus to the center of the head of the screw (FIBSCREW) measured parallel to the fibular shaft in lateral view (Figure 3). the distance from where the most distal aspect of the PBPA perforates the interosseous membrane to the anterolateral tibial plafond (ARTPLAF) measured parallel to the shaft of the fibula in anterior view (Figure 4). the distance from where the most distal aspect of the PBPA perforates the interosseous membrane to the tip of the lateral malleolus (ARTFIB) measured parallel to the fibular shaft in the anterior view (Figure 5).
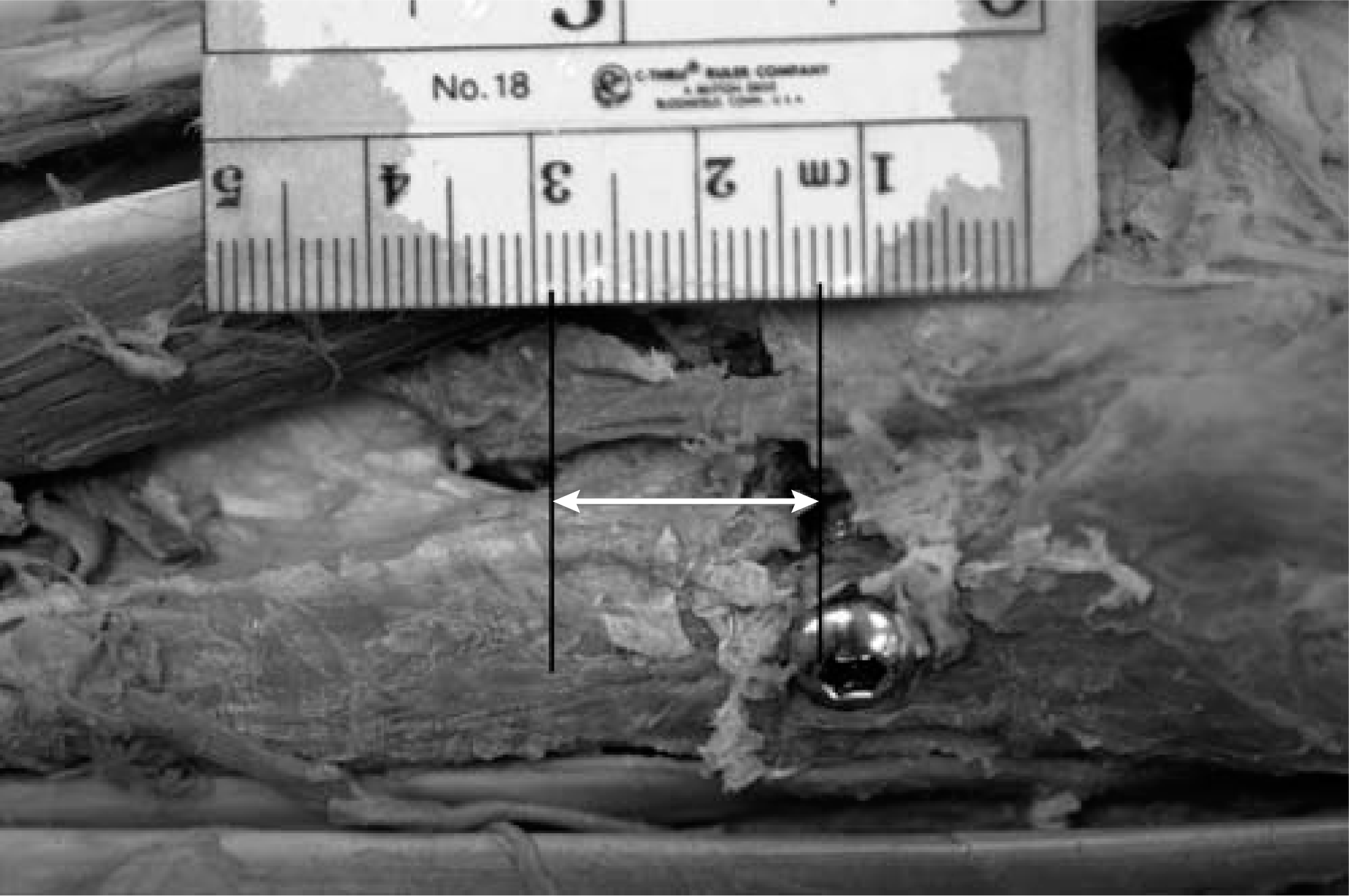
ARTSCREW: The distance from the distal most aspect of the PBPA where it perforates the interosseous membrane to the most proximal aspect of the threads along the screw shaft, measured parallel to the shaft of the fibula in anterior view.
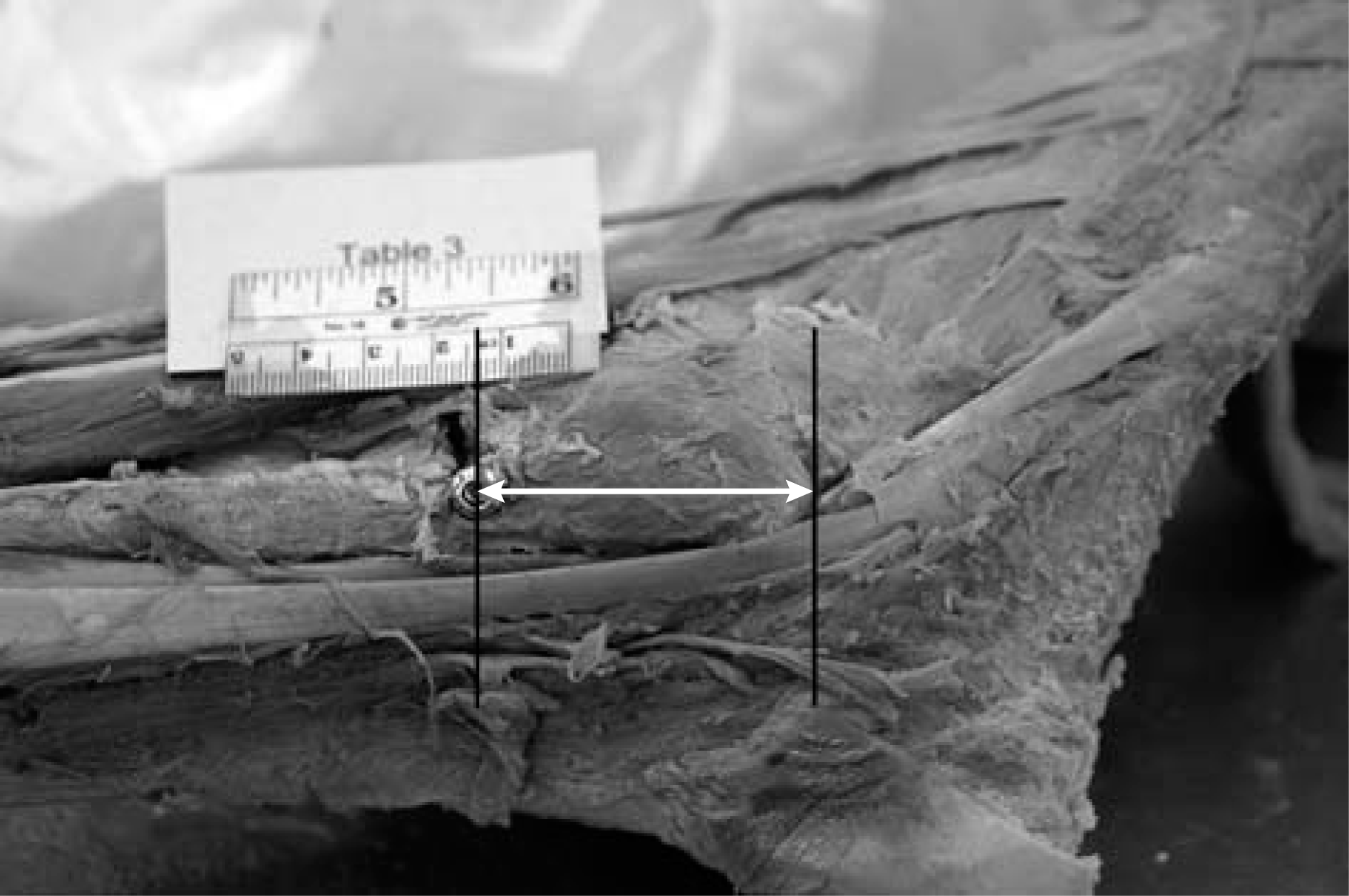
FIBSCREW: The distance from the distal tip of the lateral malleolus to the center of the head of the screw, measured parallel to the shaft of the fibula in lateral view.
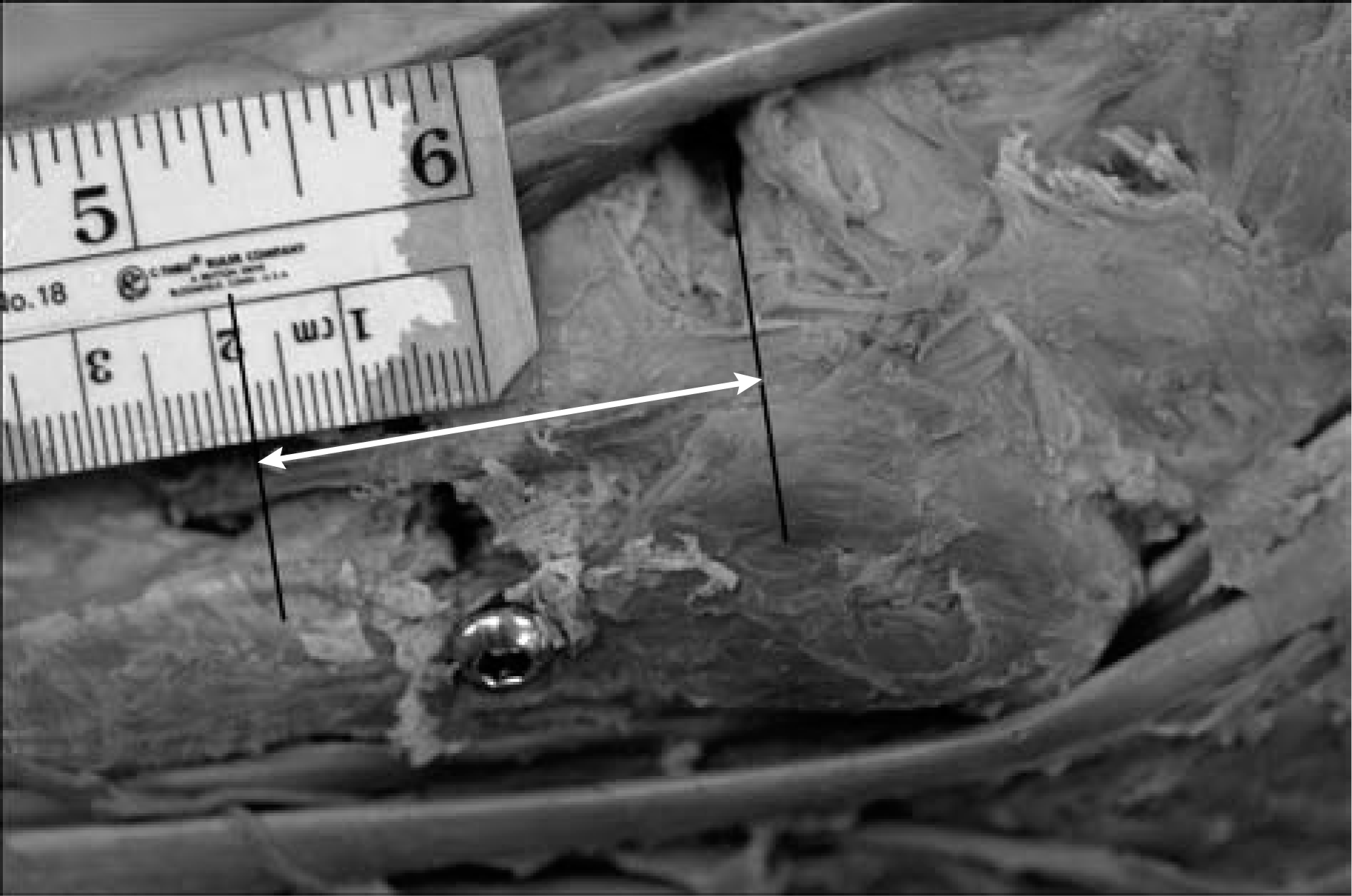
ARTPLAF: The distance from where the distal most aspect of the w PBPA perforates the interosseous membrane to the tibial plafond, measured parallel to the shaft of the fibula in anterior view.
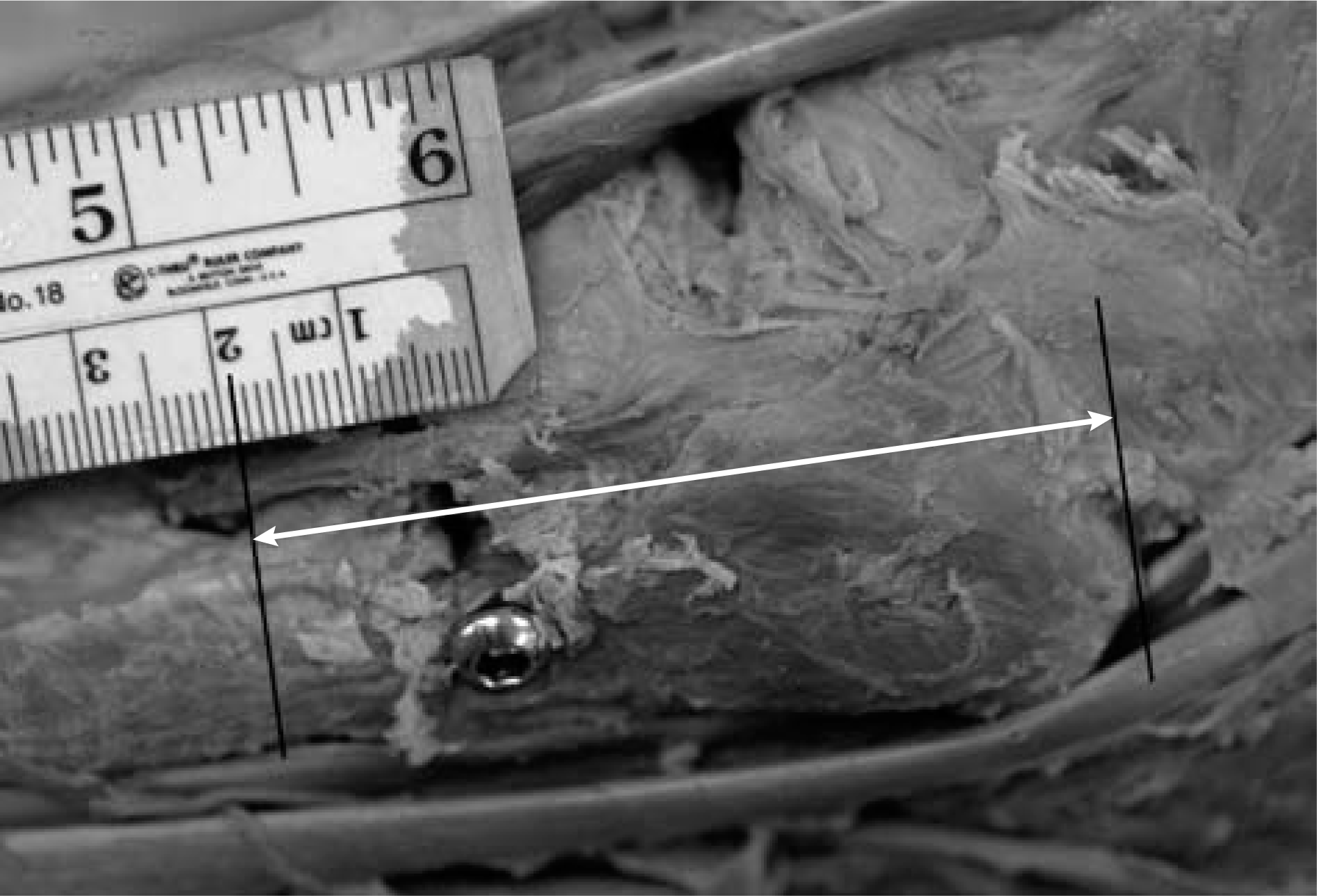
ARTFIB: The distance from where the distal most aspect of the PBPA perforates the interosseous membrane to the distal tip of the lateral malleolus, measured parallel to the shaft of the fibula in the anterior view.
Also, the distal femoral biepicondylar width (FEMBIEPI-CONWD) and proximal tibial bicondylar width (TIBBI-CONWD) were measured directly using electronic digital calipers accurate to 0.001 cm. These direct measurements were used as a proxy for body size in regression analyses.
Basic statistics, including mean distances and standard deviations, were then calculated separately for both male and female specimens. A non-paired t-test was utilized to evaluate differences between male and female specimens for each measurement (significance level, p < 0.05). The raw measurements were log-transformed (Log 10) and ordinary least-squares (OLS) regressions were calculated for each measurement against the proxy measurements of body size to assess whether or not there was any relationship between variation in the measurements with changing body size within adult populations of each sex. All statistical analyses were performed with Systat 10.0 statistical software (Systat Software, Inc., Chicago, IL).
Results
The mean, standard deviation, and range of variation for each measurement were calculated and recorded (Table 1). The mean distance of the PBPA to the tibial plafond was 3.97 cm in males and 2.92 cm in females. Similarly, the mean distance between the tip of the lateral malleolus to the PBPA was 6.17 cm in males and 5.28 cm in females. With the numbers available, T-tests revealed that the means of adult males were significantly greater than the means of adult females for these dimensions (Table 2), likely due to the greater overall average body size of adult males compared to adult females.
Mean, SD, and Range of Variation for Each Measurement
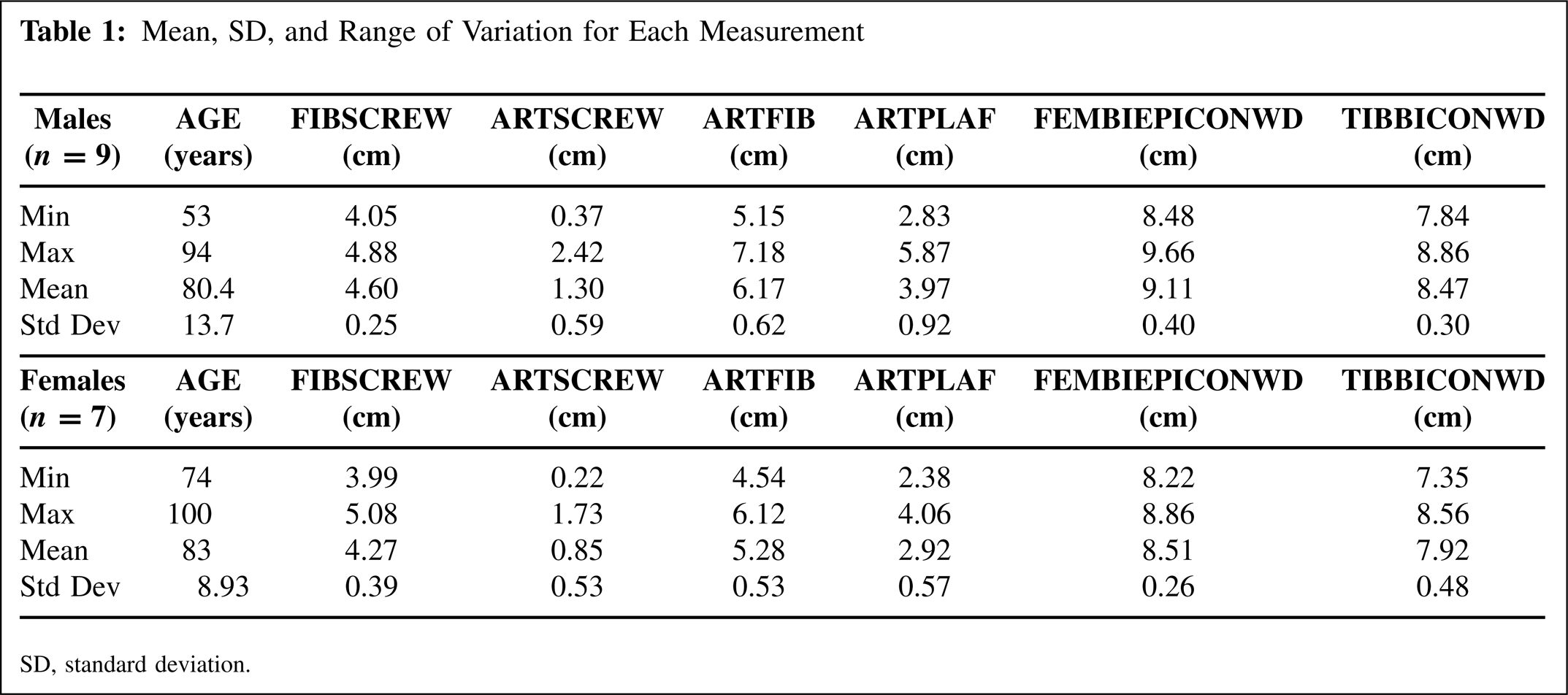
SD, standard deviation.
Non-Paired T-Tests of Adult Male and Female Means
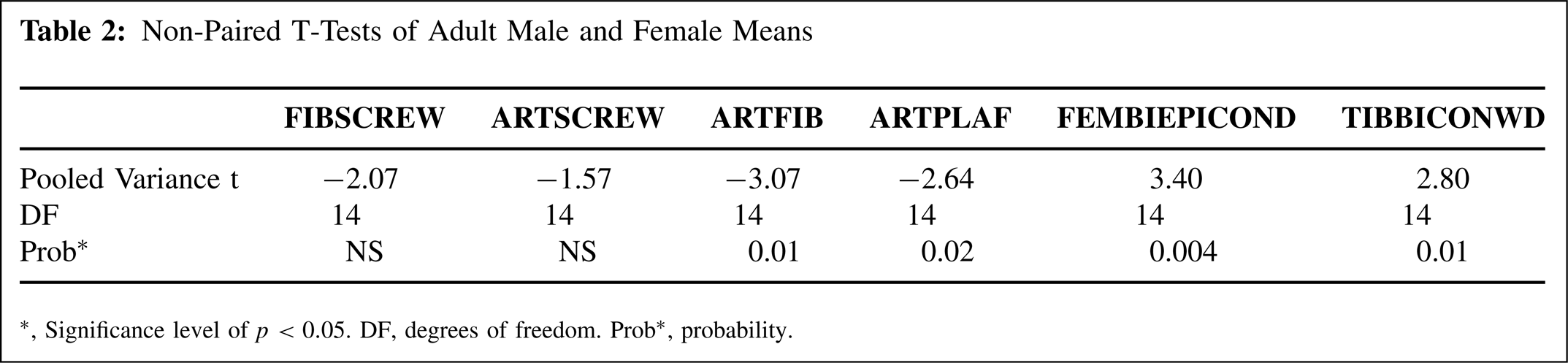
Significance level of p < 0.05. DF, degrees of freedom. Prob∗, probability.
The mean distance from the PBPA to the screw was 1.30 cm in males and 0.85 cm in females, and the mean distance between the tip of the lateral malleolus and trans-syndesmotic screw was 4.60 cm in males and 4.27 cm in females. However with the numbers available, t-tests revealed that there was no significant difference between the sexes for these measurements, probably due to the large range and standard deviation in the male sample. In six (four female, two male) out of the 16 total specimens, the screw was less than 1 cm from the PBPA. In one specimen, the screw came within 0.22 cm of the PBPA (Figure 6). While the trans-syndesmotic screw came within less than 1 cm to the PBPA in multiple specimens, none of the specimens demonstrated direct vessel penetration by the trans-syndesmotic screw.

Specimen demonstrating the trans-syndesmotic screw 0.22 cm distal to the PBPA.
Of the measurements that were significantly different between the sexes, the distance from the PBPA to the tibial plafond had the greatest average discrepancy of 1.05 cm between males and females, and the distance from the tip of the lateral malleolus to the head of the screw had the least average discrepancy of 0.33 cm. These data suggest that the PBPA perforates the interosseous membrane more proximally in adult males, compared to females, relative to the tip of lateral malleolus and tibial plafond. Also in a mixed-sex sample, OLS regressions revealed a significant size relationship between femoral biepicondylar width and both the distance of the PBPA to the tibial plafond and the PBPA to the distal lateral malleolus (Table 3). However, within each same-sex sample, OLS regressions of the variables revealed no significant size relationships with either femoral biepicondylar width or tibial bicondylar width (p < 0.05). All of the within-sex comparisons yielded low correlations and insignificant regressions, which may be due to the small samples sizes and limited size range of the samples studied. Therefore, we were unable to compare the male and female regression patterns to determine whether the differences between the means of adult males and females in PBPA location may simply be a matter of the larger average size of males or due to different patterns of variation between males and females. This issue would need to be further investigated with larger samples in order to clarify the size relationships between these dimensions.
Ordinary Least-Squares (OLS) Regressions of Dimensions
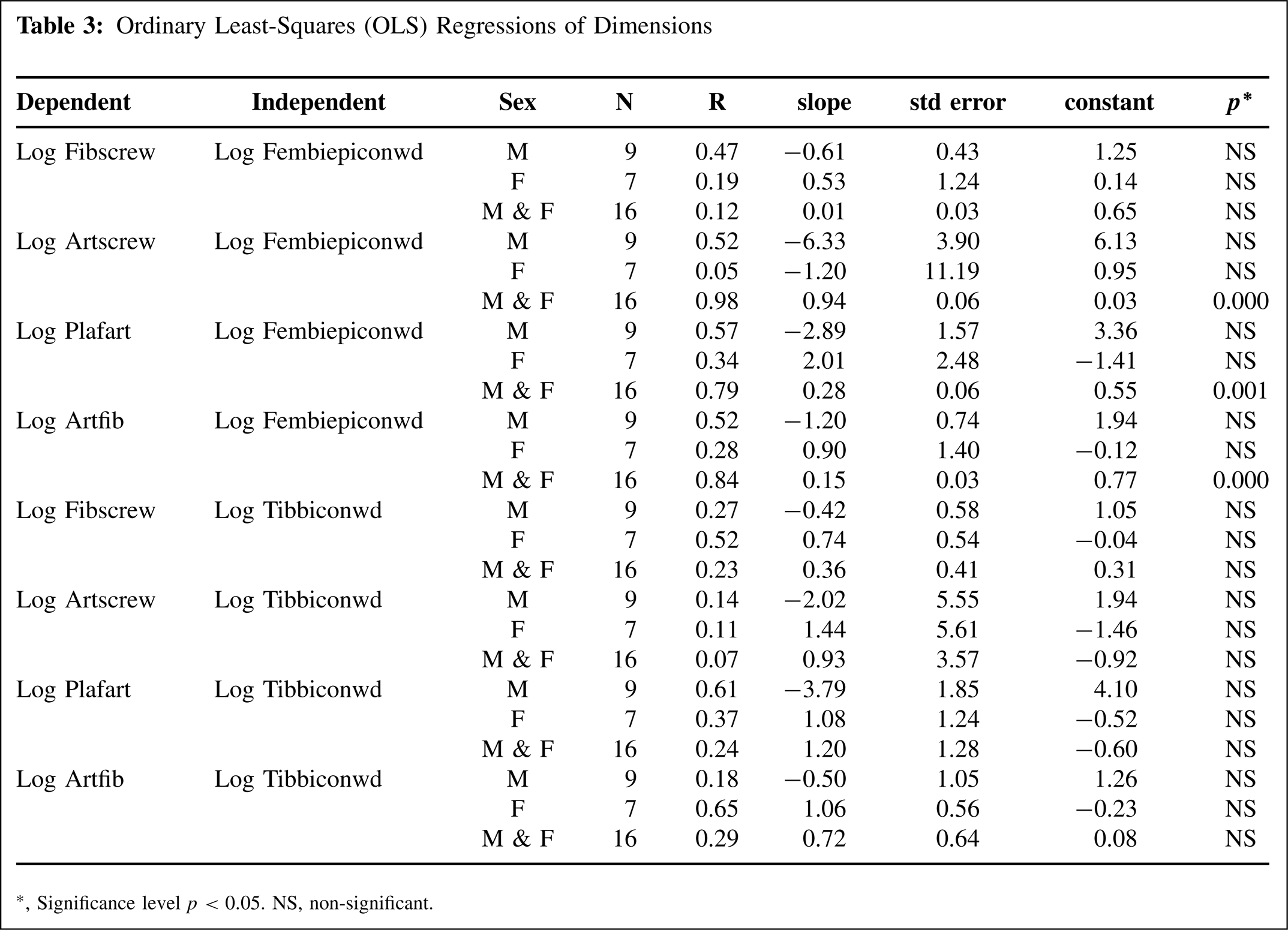
Significance level p < 0.05. NS, non-significant.
Discussion
Despite controversy surrounding the use of ankle trans-syndesmotic fixation, trans-syndesmotic screw placement remains a popular technique. 34 The literature provides numerous descriptions of variable implant choice and technique. Other forms of trans-syndesmotic fixation described in the literature besides conventional, metallic screws include hooks, 14 cerclage wires, 15 Kirschner wires, 25 bioabsorbable screws, 17 and semi-rigid dynamic stabilization. 10 Technical variation often hinges upon the number of implants utilized and the proximal positioning of the implants in reference to the tip of the lateral malleolus or the tibial plafond. Of particular interest to this study, authors have made recommendations for the placement of trans-syndesmotic fixation as low as 1 cm proximal to the tibial plafond 17 to as high as 5 cm proximal to the plafond. 42
Our results indicate that the placement of a single trans-syndesmotic screw using AO technique may place the PBPA at risk. While authors have acknowledged that knowingly jeopardizing any component of an injured lower extremity's vasculature is unwise, 4 recent data suggest that if a major arterial supplier of the foot is sacrificed, the remaining arterial supply has the compensatory ability to allow the resting blood supply of the foot to be unaltered by increasing luminal cross-sectional area and flow velocity in the uninjured vessel. 43 While considering such physiologic vascular capabilities of the lower extremity, the actual clinical result of disruption of the PBPA may be minimal in individuals with a competent distal anastomotic blood supply. Yet in spite of this recent evidence that the compensatory ability of the lower extremity's arterial supply in patients without arterial trauma, diabetes mellitus, or peripheral vascular disease is similar to the vascular compensation demonstrated in the upper extremity, 43 several important considerations should be acknowledged when the PBPA is potentially at risk from trans-syndesmotic fixation.
First due to developmental diversity and the fact that any one of the major embryonic arteries of the foot may either disappear or remain and unite abnormally, many types of arterial variations can occur in the foot and ankle. 24 Specifically, the proximal segments of the anterior and posterior tibial artery can be congenitally aplastic or hypoplastic individually or in combination. 24 Such a vascular variation often results in the PBPA supplying a substantial portion of the blood supply to the foot. 24 Of the different types of foot and ankle arterial variations, proximal attenuation of the anterior tibial artery with the PBPA assuming the expected course of the dorsalis pedis artery is one of the more commonly described in the literature.2,19,45 One of the 16 specimens included in this investigation demonstrated this arterial variation (Figure 7). Previous studies have reported an incidence of this arterial variation to be present in 1.95% to 12% of individuals.3,40 Therefore if a patient with such a vascular variation, in which the PBPA provides a substantial amount of flow to the foot, sustains a syndesmotic injury, the arterial circulation of the foot may be jeopardized by the placement of ankle trans-syndesmotic fixation.

Specimen demonstrating arterial variation with proximal attenuation of the anterior tibial artery with the PBPA assuming the expected course of the dorsalis pedis artery.
Mulfinger and Trueta 32 demonstrated that the talar blood supply is provided by a periosteal network created by the PBPA, dorsalis pedis, and the posterior tibial artery. Meanwhile others have acknowledged the talus' predisposition to avascular necrosis and that the lack of vascular redundancy makes each vascular contribution vitally important. 13 When managing traumatic talar injuries, minimization of damage to the talar blood supply is paramount. 27 Specific to the PBPA, the anterior tibial artery and PBPA contribute branches to the tarsal sinus region and the lateral portion of the talar body. 5 Also, the artery of the tarsal sinus, formed by branches of the anterior tibial artery and the PBPA, merges with the artery of the tarsal canal to supply most of the talar neck and head. 32 Consequently in a patient with concomitant injuries to both the syndesmosis and the talus, damage to PBPA with trans-syndesmotic fixation could potentially disrupt the delicate talar blood supply. The magnitude of the disruption to the talar blood supply could be exaggerated in the presence of a vascular variation. For example, iatrogenic injury to the PBPA variation involving the PBPA supplying the course of both the PBPA and the dorsalis pedis2,19,45 would result in a vascular insult to two of the three major arterial contributions to the talus. Such vascular interruption in the face of traumatic talar processes could disturb necessary revascularization of the bone and result in suboptimal outcomes in the management of these injuries.
Orthopaedic and reconstructive surgeons continue to face the clinical challenges presented by the reconstruction of complex wounds and soft tissue defects of the distal third of the tibia, ankle, and foot. 8 As acknowledged by Pirwani et al., 39 appropriate coverage of exposed soft tissue defects, bone, joint, or tendon in a timely manner is mandatory and essential for the prevention of complications. The literature has presented reconstructive options for the management of such complex lower extremity soft tissue defects that rely on the PBPA.7,39 These described techniques that depend on the PBPA have been utilized to gain soft tissue coverage over the distal third of the tibia, Achilles tendon, malleoli, dorsum of the foot, and heel. 39 Hence, the unplanned insertion of trans-syndesmotic fixation, without regard for the risk of iatrogenic damage to the PBPA in a patient with an ankle syndesmotic injury and concomitant soft tissue embarrassment, could potentially jeopardize the utilization of certain reconstructive techniques reliant on the PBPA.
Iatrogenic injury to the PBPA with trans-syndesmotic fixation could lead to local tissue and wound disturbances and even potentially limb threatening situations. Pseudoaneurysm formation of the PBPA following damage to the arterial wall due to both traumatic and iatrogenic injury has been described.16,23,36 PBPA pseudoaneurysm can lead to local symptoms from compression, such as severe throbbing pain of the lateral ankle, episodes of red flushing of the foot, and compressive neuropathy.16,41 Additional complications due to lower extremity arterial pseudoaneurysm include infection, hemorrhage from rupture, thrombosis, and peripheral embolization.16,23 Also, Ozasa et al. 35 described the formation of a lateral ankle lesion resembling pigmented villonodular synovitis secondary to a PBPA pseudoaneurysm following traumatic tearing of the artery. The natural progression of arterial pseudoaneurysm is to enlarge and frequently require further medical and operative intervention, yet proper diagnosis and treatment is often delayed.16,41 Consequently, patient morbidity can occur if the clinician is not cognizant that trans-syndesmotic fixation may inflict iatrogenic damage to the PBPA, which can lead to pseudoaneurysm formation.
Compartment syndrome of the lower extremity following an ankle sprain involving injury to the PBPA has been described. 46 In addition, Imade et al. 18 reported a case of lower extremity compartment syndrome after treating a Maisonneuve fracture with syndesmosis and interosseous membrane disruption utilizing ankle arthroscopy and syndesmosis screw fixation. In their report, Imade et al. 18 reasoned that the compartment syndrome developed due to a synergistic effect related to the local post traumatic tissue conditions and the operative intervention. Therefore due to the marked swelling and increased intracompartmental pressures that can be associated with ankle syndesmosis injuries, one must be aware that either a traumatic or iatrogenic injury to the PBPA secondary to trans-syndesmotic fixation could potentiate lower extremity compartment syndrome.
According to the results of the current study, the placement of trans-syndesmotic fixation 2 cm proximal to the tibial plafond will result in the PBPA being on average less than 1.3 cm proximal to the screw. Therefore in order to avoid injury to the PBPA with trans-syndesmotic fixation in the female patient, avoiding fixation insertion 2.3 to 4.1 cm proximal to the tibial plafond or 4.5 to 6.2 cm proximal to the tip of the lateral malleolus may provide the best chance of avoiding the PBPA. Similarly in the male patient, avoiding insertion 2.8 to 5.9 cm proximal to the tibial plafond or 5.1 to 7.2 cm proximal to the tip of the lateral malleolus may provide the best chance of avoiding the PBPA. If the surgeon is faced with a situation in which syndesmotic fixation must be placed within these zones or faced with a complex foot and ankle injury that may include a dysvascular limb, one may consider further characterizing the vascular integrity and distribution of the lower extremity with vascular studies, such as angiography, to better assess the risk versus benefit of syndesmotic fixation placement in the proposed area.
Strengths of the present study include a relatively large sized cadaveric sample with even distribution of male and female specimens and the utilization of a reproducible technique for trans-syndesmotic screw insertion. Also in addition to generating information about the surgical technique of syndesmosis fixation, this investigation provides specific anatomical data which detail relationships of the PBPA to the tip of the lateral malleolus and the tibial plafond, which are readily identifiable anatomic structures. Such anatomical information provides the clinician with the ability to estimate the location of the PBPA in reference to anatomical landmarks that are consistent and simple to palpate. Conversely, limitations of the present study include the utilization of an indirect measuring technique using photographic images and morphometric software. Since the PBPA and the trans-syndesmotic screw often existed in very close proximity to each other, trial measurement gathering with calipers generated difficulty positioning the calipers and less precise data. Therefore, the investigators felt the selected indirect measuring technique would provide the most accurate and precise measuring method, while also being the least invasive anatomically in order to maximally preserve the anatomical relationships of interest. Also, the use of embalmed cadaveric specimens with an average age older than the typical patient requiring trans-syndesmotic fixation could be considered a limitation. Despite these limitations, one may draw several conclusions that are clinically applicable and that may be applied to other surgical procedures involving instrumentation across the syndesmosis, such as the modified fibula-protibia procedure for treatment of periplafond tibia fractures. 12 Future research efforts could investigate the placement of more than one screw, the use of different implants, and careful prospective examination of vascular integrity before and after trans-syndesmotic fixation.
Conclusion
This study confirmed that the placement of ankle trans-syndesmotic fixation poses a risk to the PBPA. Such risk could lead to both local and catastrophic consequences in certain clinical situations. Despite variability in technique and indications, anatomic reduction of the syndesmosis that is stable has been emphasized9,25,29,47 and is associated with improved functional outcomes.9,25,47 Therefore during operative decision making, the clinician must evaluate the risk of trans-syndesmotic screw placement in each clinical situation versus the established benefit of screw placement. Armed with this knowledge, physicians treating syndesmosis injuries will be better prepared to possibly prevent and identify complications associated with ankle trans-syndesmotic fixation.