
Abstract
Background: Arthrodesis of the first metatarsophalangeal joint is an effective procedure for many foot pathologies. Many studies have focused on the moment at which joint fusion is carried out, or on the medium- and long-term outcomes. The aim of this study was to assess the clinical progression of patients, evaluating both pain and changes on the AOFAS scale at various points during the first postoperative year. Material and Methods: A prospective study with 49 patients was conducted. The AOFAS scale and pain was collect both preoperatively and at 3, 6, and 12 months after first metatarsophalangeal arthrodesis with 20-mm memory compression staples. The data obtained were analyzed for functional status and pain during the first year after surgery. Results: The mean preoperative AOFAS score was 39 compared with a mean postoperative score at 1-year followup of 85. The results of the AOFAS scale at 3- and 6-months post-surgery showed considerable variation. In contrast, at 12 months the mean results tended to converge, thus suggesting greater reliability in the prognosis. The change in pain over time differs from the AOFAS. Pain improved rapidly during the first 6 months; it peaked during the first 3 months, but the data suggests that it was from 6 months onward that prediction of pain levels begin to be more predictable and consistent. Conclusion: The present results show that scores on the AOFAS scale and for pain improve progressively throughout the first year following first MTPJ fusion. At 3 months the results for both pain and the AOFAS scale had a low predictive value due to the wide variation in scores. However, at 6 months, pain stabilized and scores showed greater precision, thus increasing the predictive value of the results. With the AOFAS scale, there continued to be considerable variation at 6 months, and it was not until 1-year post surgery that scores showed an acceptable degree of precision.
Level of Evidence: IV, Case Series
Introduction
Arthrodesis of the first metatarsophalangeal joint (MTPJ) is an effective procedure for many foot pathologies in which conservative treatment has failed.3,5,6,8,10,12,15,16–18 Indeed, it continues to be the procedure of choice for hallux rigidus with advanced joint destruction, 23 and has also been recommended as salvage for large deformities of the big toe or after the failure of previous surgery such as excisional arthroplasty of the MTPJ. It is also a technique that is widely used in the rheumatoid patient.5,6,15,18,19,22,24
Many studies have focused on the moment at which joint fusion is carried out, or on the medium- and long-term outcomes. However, we are not aware of any published study that has analyzed patients’ functional evolution and pain during the first postoperative year. In our view this information would be useful in order to offer patients more accurate information about the pace of surgical recovery.
The aim of this study was to assess the clinical evolution of patients undergoing an arthrodesis of the first metatarsophalangeal joint with 20-mm memory compression staples, evaluating both pain and changes on the AOFAS scale at various points during the first postoperative year.
Materials and Methods
A prospective study was conducted between February 2005 and February 2008. A total of 49 patients with various painful primary and secondary conditions involving the first MTPJ were evaluated and treated surgically in our institution. A first MTPJ arthrodesis using 20 mm memory compression staples was performed in all cases. There were 42 women (85.7%) and 7 men (14.3%), with a mean age of 61 (range, 57 to 68) years. The mean followup was 14 (range, 12 to 16) months.
Scores on the American Orthopedic Foot and Ankle Society (AOFAS) Hallux Metatarsophalangeal-Interphalangeal Scale were obtained prospectively, 13 while the patients’ pain was assessed using a visual analogue scale, both preoperatively and at 3, 6, and 12 months after surgery. The patients’ degree of satisfaction 1 year after the operation was also evaluated using the scale developed by Coughlin and Mann. 5 In the postoperative AOFAS scale for a solidly fused immobile first MTPJ, the maximum value is 90 points. This would represent a patient with no pain, solid fusion with good alignment and with no functional or shoewear limitations.
Patients must have had preoperative and postoperative anteroposterior (AP) weight bearing and lateral radiographs. The intermetatarsal (IM) and hallux valgus (HA) angles were measured and compared between the preoperative and postoperative AP views.
Postoperatively, patients were followed up in the outpatient department every week until wound healing, and then every 4 weeks until radiographic fusion and, finally, every 3 months up to 12 months.
Results were expressed as frequencies and percentages for qualitative variables and as means (standard deviation) and medians [interquartile range: P25th; P75th] for quantitative variables. Univariate inferential analysis was performed using Fisher's exact test or the U-Mann-Whitney test. Inferential non-parametric tests for repeated measurements of AOFAS and pain were derived from a longitudinal general linear model, applying a rank transformation on the dependent variable and including diagnosis, type of surgical procedure and pre-surgical evaluation of the dependent variable. Least Square means (LSMEANS) and 95% confidence interval (95% CI) were estimated using the same model with no transformation for clinical discussion purposes. For a graphical evaluation of AOFAS and pain scales, we considered mean ± 2* standard error (m ± 2*SE) across time. P values 0.05 were considered statistically significant. Statistical analysis was performed with the SPSS 15.0 package (SPSS, Chicago, IL).
Results
The mean preoperative AOFAS score was 39 (range, 34 to 47), compared with a mean postoperative score at 1-year followup of 85 (range, 80 to 90) (p = 0.001). The preoperative hallux valgus angle (HVA) decreased significantly from 25.8 (range, 6 to 46) degrees to 10.7 (range: 4 to 20) degrees postoperatively (p >0.05). The mean preoperative intermetatarsal angle (IMA) was 11.5 (range, 6 to 18) degrees, compared with a postoperative angle of 10.0 (range, 4 to 16) degrees (p >0.05). The DFA is the angle between the long axis of the first metatarsal and the first toe in the lateral view. The AI is the angle between the long axis of the first toe and the floor, also in the lateral view. The mean dorsiflexion angle (DFA) of fusion was 25.7 (range, 15 to 36) degrees, while the mean angle of inclination (AI) was 21.7 (range, 10 to 28) degrees. Radiological union was obtained in 47 of the 49 feet (95.9%), with a mean time to union of 11 (range, 8 to 14) weeks.
One patient developed a nonunion that required reoperation, while another patient diagnosed with hallux rigidus developed nonunion, which was associated with failure of the dorsal staple and soft-tissue irritation. This patient was treated conservatively (partial weight bearing and shoe with rigid sole), which decreased the symptoms but failed to alter the radiographic nonunion. The patient wanted no further treatment and believed that the symptoms were tolerable.
One patient with severe osteoporosis required supplementary fixation with two Kirschner wires due to the poor stability provided by a loose dorsal staple. The Kirschner wires were removed 4 weeks after surgery and a successful union was observed at 16 weeks of followup.
Evolution of the AOFAS scale during the first year
The ANOVA model to assess differences in AOFAS scores compared to the pre-surgical procedure (Table 1) showed an effect for the pre-surgical AOFAS score (p = 0.002) but not for diagnosis (p = 0.451) or time of surgical procedure (p = 0.886).
Evolution AOFAS Score and Pain by Means of the Longitudinal Linear Model. Comparison of different groups depending on the diagnosis or surgical procedure. The numerical values showed in the intersections of the table represent differences of evolution measures.
The results of the AOFAS score at 3- and 6-months post-surgery showed considerable variation, evaluated as the mean ± 2* standard error (m ± 2*SE). In contrast, at 12 months the mean results tended to converge, thus suggesting greater reliability in the prognosis offered by this scale in this group of patients (Figure 1). In other words, regardless of the mean evolution over time, the estimates are rather imprecise at 3 and 6 months and this makes it difficult to offer a correct prediction of the patient's status at these points.
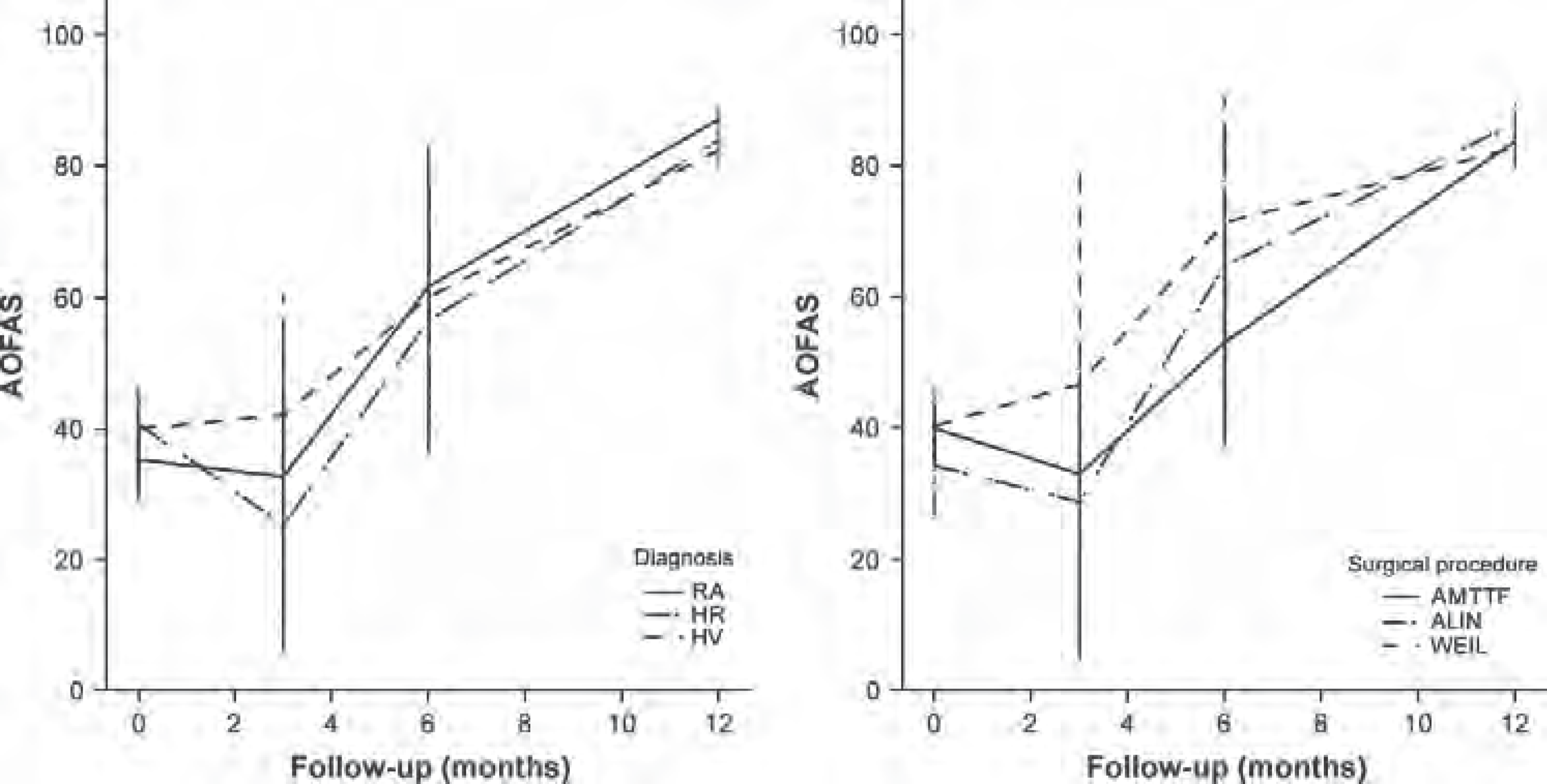
Evolution of AOFAS score during the first year.
When evaluating the AOFAS score by means of the longitudinal linear model (adjusted according to pre-surgical AOFAS score and time of surgical procedure) we observed that patients diagnosed with rheumatoid arthritis (RA) seemed to obtain a greater mean difference (weighted by time) in their AOFAS score compared to patients treated for HR or HV (p = 0.451) (Table 1).
We also found that patients whose arthrodesis was associated with a metatarsal head resection for lesser metatarsal alignment obtained a lower mean score on the AOFAS (longitudinal linear model, adjusted by pre-surgical score (p = 0.002) (Table 1).
No significant differences were observed with respect to age, sex or diagnosis according to the AOFAS group. We have divided the patients into two groups, using the median value (AOFAS = 85) as cut-off, from final AOFAS scores. The aim of this division was to study the profile of patients with the best AOFAS scores and search differences between the good and excellent results. For patients treated by means of metatarsophalangeal joint arthrodesis (MTPJA), with or without metatarsal realignment, the percentages were comparable in both AOFAS groups (Fisher's exact test, p = 0.016). At 1-year followup, two-thirds of patients with a postoperative AOFAS score below 85 required some kind of special shoe, whereas those with an AOFAS score above 85 experienced no pain (U-Mann-Whitney, p >0.001) (Table 2).
AOFAS Groups Adjusted by the Pre-surgery Median Score. Groups were made from median cut-off (AOFAS = 85) of final AOFAS results.
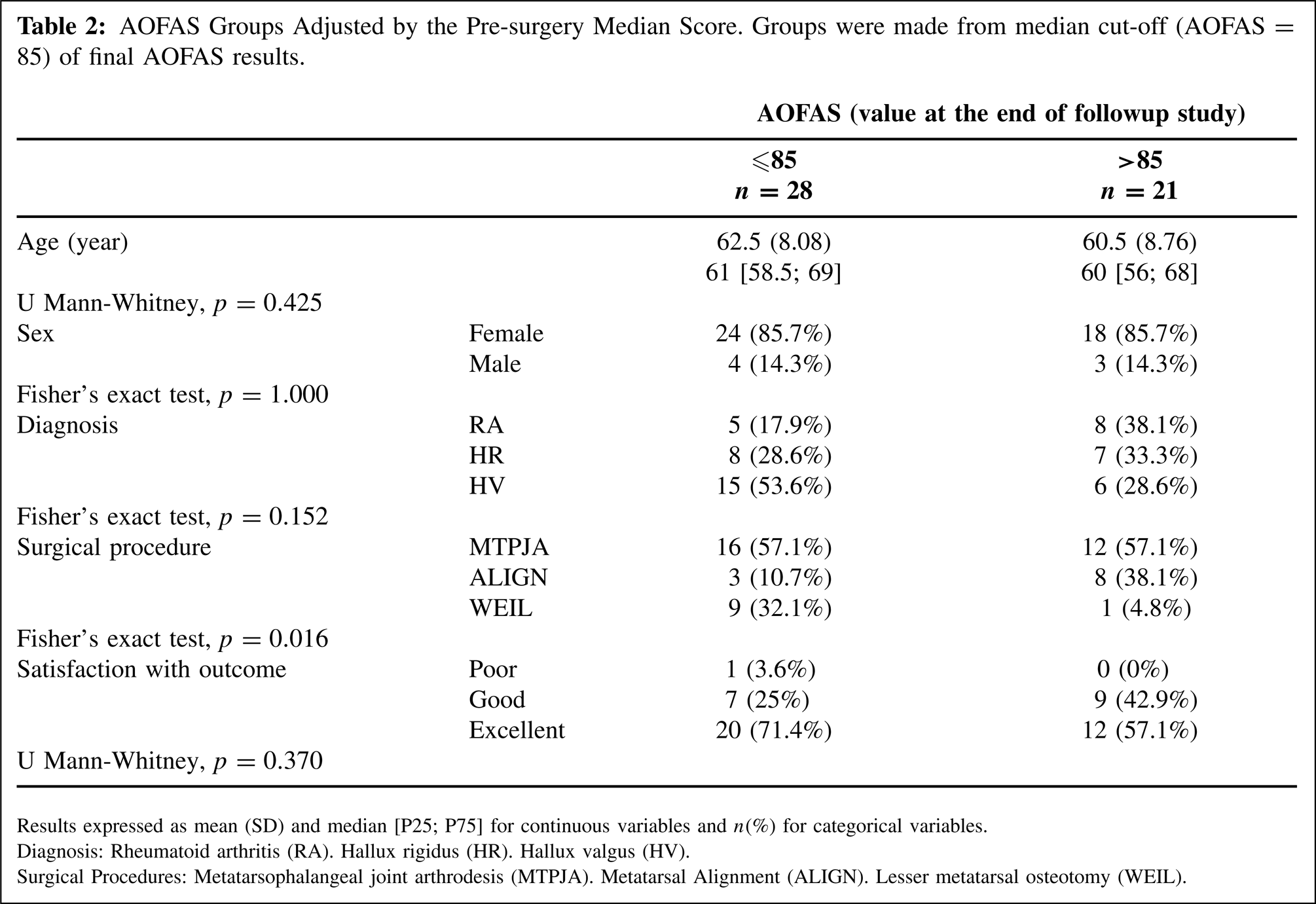
Results expressed as mean (SD) and median [P25; P75] for continuous variables and n(%) for categorical variables.
Diagnosis: Rheumatoid arthritis (RA). Hallux rigidus (HR). Hallux valgus (HV).
Surgical Procedures: Metatarsophalangeal joint arthrodesis (MTPJA). Metatarsal Alignment (ALIGN). Lesser metatarsal osteotomy (WEIL).
Pain scale evolution during the first year
The evolution of pain over time differs from that of scores on the AOFAS scale. Pain improved rapidly during the first 6 months; improvement peaked during the first 3 months before stabilizing. Thus, although patients vary in terms of how quickly they improve, the variation in scores began to lessen at 6 months, the precision (measured as m ± 2*SE) being practically identical to that attained at 12 months. This suggests that it is from 6 months onwards that prediction of pain levels begin to be more reliable (Figure 2).
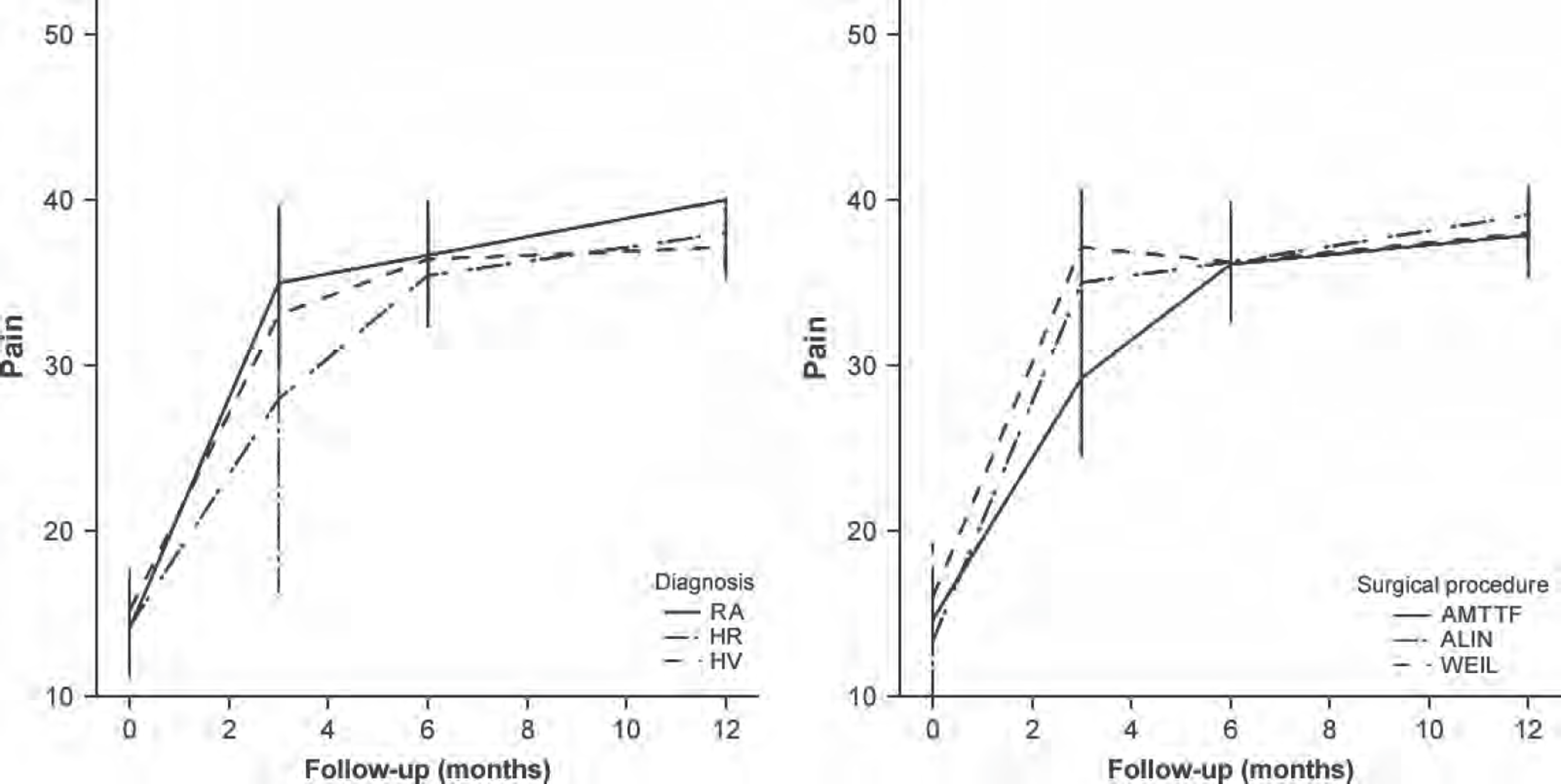
Evolution of pain during the first year.
Patients diagnosed with RA obtained a greater mean difference (weighted by time) in their pain scores compared to those treated for HR or HV, the values for the latter two groups being 3.1 (CI 95% 1.2; 5.1, p = 0.004) and 2.4 (CI 95% 0.5; 4.3, p = 0.019), respectively (Table 1).
Discussion
Numerous techniques have been described for arthrodesis of the first MTPJ, although the published results are inconsistent (fusion rates from 40 to 100%). 4 The more recent literature focuses on the use of rigid internal fixation systems, and several biomechanical studies have been conducted to compare the different fixation methods.14,20 However, clinical series published over the last 10 years have reported similar results regardless of the fixation system used (fusion rates from 86 to 100%), in spite of experimental studies describing them as having different biomechanical behavior.1,2,7,9,21
One interpretation of these findings is that surgical technique, the position of arthrodesis and joint preparation are more important than the fixation system itself, the latter having greatly benefited from the wider use of cup and cone reamer systems. 11
Many studies have focused on the moment at which joint fusion is carried out, or on the medium- and long-term outcomes. However, we are not aware of any published study that has analyzed the evolution in patients’ functional status and pain during the first postoperative year. In our view this information would be useful in the context of postoperative care and for offering patients a more detailed opinion regarding their progression after surgery.
We observed that our patients’ AOFAS scores after a MTPJ arthrodesis with 20-mm memory compression staples at 3 months showed wide variability and this prevented reliable predictions from being made. However, the sample continued to show improvement over the first year and at 12 months there was much less variation in AOFAS scores, thus enabling us to offer patients a firmer opinion as to when they would recover acceptable levels of functioning.
The data suggest that obtaining a joint fusion (mean time of 11 weeks in this series) does not always lead to a high AOFAS score, at least not immediately. Thus, a patient with a solid joint fusion at 3 months may still score low on the AOFAS scale.
Moreover, in the event of a pseudoarthrosis this may be fibrous and painless. 7 Therefore, in our opinion the attainment of joint fusion should be evaluated as a relatively successful outcome of surgery that requires confirmation by a maximum score on the AOFAS scale, which appears to be reliably obtained one year after the intervention.
In this series we observed that pain stabilized in most of our patients at 3 months, although at this stage the data were less precise. At 6 months this stabilization was more reliable as the results showed less variation.
Conclusion
The present results show that scores on the AOFAS scale and for pain improve progressively throughout the first year of followup after a MTPJ arthrodesis with 20-mm memory compression staples. At 3 months the results for both pain and the AOFAS score had a low predictive value due to the wide variation in scores. However, at 6 months, pain stabilized and scores showed greater precision, thus increasing the predictive value of the results. With regard to the AOFAS scale, there continued to be considerable variation at 6 months, and it was not until 1-year post surgery that scores showed an acceptable degree of precision.
It should also be noted that joint fusion does not, in itself, lead to immediate improvements in AOFAS and pain scores, although there is a trend toward improvement on the AOFAS scale once fusion has been achieved. With respect to the pain reported by patients, it stabilized at around 6 months, considerably later than the mean time required to achieve radiographic joint fusion. In terms of pain, patients with RA showed a better evolution than do those treated for HR or HV.