
Abstract
Background: The purpose of this study was to identify the rates of readmission to the hospital for pulmonary embolism following open reduction and internal fixation of metatarsal fractures using observational, population-based data from all inpatient admissions in California over an 11-year period. Materials and Methods: We identified patients undergoing open reduction and internal fixation of a metatarsal fracture in the years 1995 to 2005 as inpatients using California's discharge database. The outcomes analyzed included readmission within 90 days of surgery for pulmonary embolism. Logistic regression models were used to estimate the impact of patient factors such as age, race/ethnicity and gender in predicting the rates of thromboembolic disease. Results: A total of 1,477 metatarsal ORIF procedures were performed as inpatients during the study period. We identified four patients (0.27%) readmitted with pulmonary embolism within 90 days of their initial ORIF procedure. There were three (0.20%) cases of mortality, none of which occurred in the four patients readmitted with pulmonary embolism. Given the low incidence, we did not identify age, gender, or race/ethnicity as statistically significant predictors of a higher risk of thromboembolic disease. Conclusion: The rate of readmission for pulmonary embolism was low. This suggests that the routine use of thromboprophylaxis may not be necessary for isolated metatarsal fractures to prevent pulmonary embolism.
Level of Evidence: II, Prognostic Study
Introduction
The incidence and risk factors for thromboembolic disease associated with operative treatment of isolated metatarsal fractures have not been definitively documented. Several authors have reported rates of thromboembolic disease but most of these studies are from single centers or include a wide variety of foot and ankle pathology.3,4 The purpose of this study was to identify the rates and patient factors that predict readmission to the hospital for pulmonary embolism following open reduction and internal fixation of isolated metatarsal fractures using observational, population-based data from all inpatient admissions in California over an 11-year period. Our hypothesis was that the incidence of pulmonary embolism requiring readmission would be low.
Materials and Methods
Data source
Data for all hospital discharges in California in the years 1995 to 2005 were obtained from California's Office of Statewide Health Planning and Development (OSHPD) through the patient discharge database. This database is compiled annually by OSHPD and includes discharge abstracts from all non-federal hospitals in California. Each discharge abstract includes codes for up to 20 inpatient procedures and 24 diagnoses per hospitalization. All procedures and diagnoses are coded using the International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM). Also included are patient demographic information (race, Hispanic ethnicity, gender, expected source of payment, age, and ZIP code of residence), outcomes (in-hospital mortality), and site of hospitalization (unique hospital identifier and ZIP code). 7 Deaths were identified from the state death file. 7 The study protocol was reviewed and approved by the UCLA institutional review board. Due to the nature of these secondary data analyses, waiver of patient consent was granted.
Inclusion and exclusion criteria
The patient sample consisted of patients undergoing inpatient surgical management of a isolated, closed metatarsal fracture during the study period. Patients with a diagnosis code for a closed metatarsal fracture and a procedure code for open reduction with internal fixation of metatarsal or tarsal bone were identified. Patients with prior or concominant diagnosis of other foot injuries, including fractures, dislocations, infections, or malignancy were excluded. Patient with concomitant fractures of the foot, ankle, tibia or femur were excluded. Patients with a non-California ZIP code were excluded, as they are less likely to be captured for followup in a California-only database.
Outcomes studied (dependent variables)
For patients meeting the inclusion and exclusion criteria, all subsequent hospitalizations within the state of California during the study period were identified. Any readmission with a diagnosis for pulmonary embolus (PE) within 90 days were identified. In addition, linkage to the California state vital statistics data identified mortality within 90 days. The specific ICD-9-CM codes used to identify inclusion, exclusion, and outcome criteria are included in Table 1.
Coding Algorithm Used in Identifying Inclusion Criteria, Exclusion Criteria, Diagnosis, and Complications

Predictors (independent variables)
Independent variables of interest included patient characteristics. Their inclusion in the statistical models allowed us to adjust for their effect on outcome. Patient characteristics used as independent predictor variables included age, gender, and race/ethnicity (white, black, asian, Hispanic, and other).
Statistical analysis
All statistical analyses were performed using Stata/SE 8.0. (StataCorp, College Station, TX). Descriptive statistics for included cases were calculated, and raw rates of complications were identified. We used multivariable logistic regression to identify the independent effect of the predictor variables on the probability of readmission for pulmonary embolism. We modeled the risk of pulmonary embolism within 90 days as a function of our predictor variables. The strength of association between the 90-day rate of pulmonary embolism and the predictor variables was expressed as an odds ratio with respect to a reference group.
Results
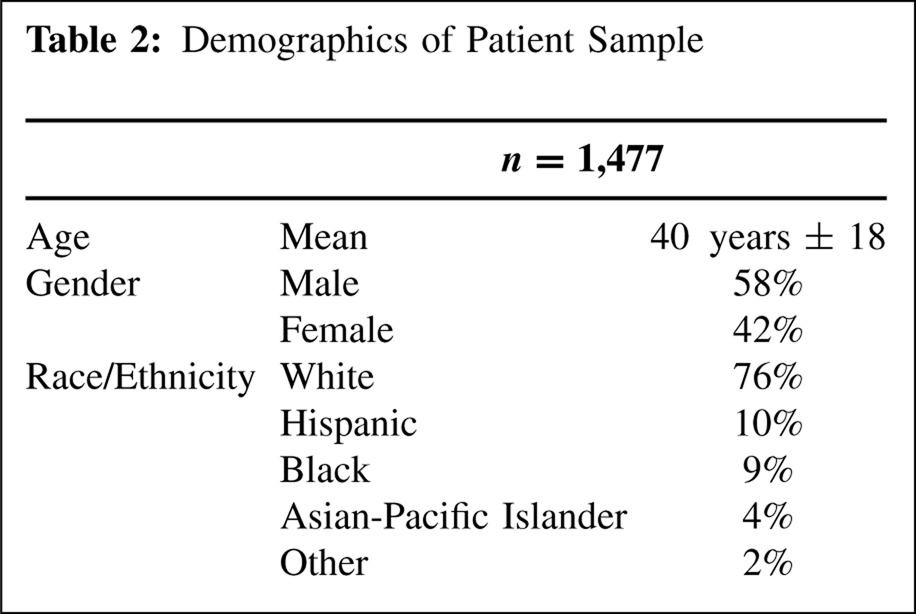
A total of 1,477 patients undergoing open reduction and internal fixation for isolated closed metatarsal fractures were identified. The mean age of the patient sample was 40 years with male gender being more common (58%). Patients of White race comprised 76% of the patients, with 10% Hispanic, 9% Black, 4% Asian, and 2% of other race (Table 2).
Demographics of Patient Sample
There were four cases of readmission for pulmonary embolism within 90 days, yielding a rate of 0.27%. There were three deaths within 90 days (0.20%) with none of the cases of mortality occurring in the group that were readmitted for pulmonary embolism (Table 3). Logistic regression analysis did not identify patient age, race/ethnicity, or gender as statistically significant predictors of either pulmonary embolism or mortality.
Ninety-day Rates of Complications

Discussion
There remains uncertainty regarding the incidence of thromboembolic disease following surgery of the foot. The current study reports low rates of readmission for pulmonary embolism following open reduction and internal fixation of isolated metatarsal fractures. The low rate of readmission for pulmonary embolism (0.27%) in this large cohort, combined with the fact that none of these cases were fatal, indicates that routine chemical thromboprophylaxis is probably not indicated.
Due to the nature of the study, it was not possible to review medication records following surgery, and the nature of thromboprophylaxis, if any, is unknown. There have been reports that the use of thromboprophylaxis is not widespread among foot and ankle surgeons. Gadgil and Thomas reported that 19% of surveyed foot and ankle surgeons in England and the United States routinely use prophylaxis. 1 Wolf and DiGiovanni surveyed members of two orthopaedic societies and 44% of surgeons reported using thromboprophylaxis in foot and ankle trauma cases. 8 These survey findings suggest that the low rate of thromboembolic disease observed in our study occurred despite the fact that it is likely that the majority of the patients did not receive thromboprophylaxis.
There are a number of limitations inherent to this administrative database that should be mentioned. First, there is a limited amount of clinical information available for analysis. While we can exclude patients diagnosed with other fractures in the foot and ankle, the severity and pattern of injury is unknown. Patients who received treatment outside the state of California are not captured; this effect is minimized by excluding patients whose home ZIP code is outside the state. Finally, isolated emergency room visits and outpatient procedures are not captured. Therefore, the rate of complications from deep venous thrombosis was not analyzed given that most cases of DVT do not require admission.
Despite these limitations, our study was able to capture all patients treated as inpatients over an 11-year period in the state of California, representing a diverse, heterogenous population. With this large population, even rare and infrequent events are seen in enough numbers to be analyzed. Furthermore, any followup within the state of California, even at a different hospital with a different provider, is available. As a result, our study presents data that confirms prior reports of low rates of thromboembolic disease seen in patients with foot and ankle disorders.3,4,6,7 The widely cited American College of Chest Physicians guidelines for thromboembolic prophylaxis do not directly address the need for thrombrophylaxis in patients undergoing minor orthopaedic surgery. 2 However, even for total hip and knee arthroplasty, there is concern that the guidelines do not adequately balance the added morbidity of postoperative hematoma and subsequent guidelines from the American Academy of Orthopaedic Surgeons have less strict recommendations for the use of chemoprophylaxis. 5 The findings of our study suggest that routine thromboprophylaxis may not be necessary for operative treatment of metatarsal fractures.
These results may also have applicability to other types of foot procedures that have a similar level of invasiveness. Most elective forefoot and midfoot procedures are performed on an outpatient basis and are not likely to be amenable to study using patient discharge databases. However, patients undergoing those types of procedures are likely to have a similar or lower level of acuity to that seen in the population of this study. The coding in the current study is sufficiently broad that procedures such as tarsometatarsal injuries are likely to have been included in the patient population. Similarly, the patients in the current study are likely to tend towards higher acuity as a large percentage of healthy patients with isolated metatarsal fractures are treated in outpatient settings not captured in the patient discharge database. Despite these factors, the observed rate of thromboembolic disease remained low even though the probable inclusion of more significant injuries would have been expected to increase the risk of thromboembolic disease.
Footnotes
Editor's Note
The authors are to be commended for performing a large database study. They readily acknowledge the limitations of this database study, primarily that only inpatient data is available. There were definitely a large number of patients with metatarsal fractures treated as outpatients that were not part of the study. Also, DVT occurrence, which would be more common, was not captured since it is usually treated as an outpatient. It is helpful that the study supports not using thromboprophylaxis regularly following minor fracture care of the foot.