
Abstract
Background: Fusion of the first metatarsophalangeal joint is considered a ‘gold standard’ procedure for arthritis and as a salvage procedure for previous failed surgeries. Recent biomechanical studies have shown that a combination of a plate and screw is the most stable construct. Only a few studies have evaluated this combination and they have small cohorts so we are presenting our larger series of patients. Materials and Methods: Forty-six consecutive cases of first metatarsophalangeal joint fusion performed between April 2006 and April 2008 were performed using a dorsal plate and a compression screw. We analyzed the outcome in terms of fusion rate, patient satisfaction and complication rates. The average followup period was 23 (range, 14 to 37) months. The most common indications were hallux rigidus and severe hallux valgus. Results: Ninety-eight percent of the cases fused uneventfully by four months. The average time to fusion was 3.1 months. There was one non-union, which remained asymptomatic after metal removal which was the only case requiring removal of metal. There was no hardware failure. The patient satisfaction was 100%. The average AOFAS score was 82.1 (maximum, 90). Conclusion: These results show that arthrodesis of the first MTP joint with spherical reamers and a low-profile contoured dorsal titanium plate and compression screw is highly successful, with excellent patient satisfaction and functional outcomes. We recommend the use of specially designed plates against improvised plates as bending leads to poor control over dorsiflexion and may increase the incidence of plate failure.
Level of Evidence: IV, Retrospective case series
INTRODUCTION
First metatarsophalangeal joint fusion is widely performed for a variety of conditions including osteoarthritis, rheumatoid arthritis and severe hallux valgus. It is also used for failed hallux valgus surgery and as a salvage procedure for failed MTP arthroplasty.13,22 It is considered a ‘gold standard’ procedure with very satisfactory results. 11 Many techniques have been described. An ideal fixation method should be reproducible, lead to a high fusion rate and have low incidence of complications. The techniques of joint surface preparation and fixation methods are crucial for successful fusion. 14 The surfaces may be prepared with simple debridement; cut flat or reamed using spherical or conical reamers. The published fixation methods vary widely and include parallel or crossed wires or screws, steinman pins, staples, cerclage wires, bio absorbable devices, dorsal plates and external fixators. Published rates of successful union vary from 80 to 100%.2–4,9,10,12,17,21 Biomechanical analysis of different fixation methods has shown that the combination of a lag screw with a dorsal plate is the most stable construct.6,7,18,20 We found few studies using this combination but the numbers were small. We present our series of 46 cases, using a dorsal plate and lag screw. We analyzed the outcome in terms of fusion rate, function, patient satisfaction and complication rates.
MATERIALS AND METHODS
This is a longitudinal study of 46 feet operated by or under the direct supervision of the senior author (P.F.R.) from April 2006 to April 2008. There were 36 females and 10 males, with an average age of 62 (range, 42 to 84) years (Table 1). The average followup period was 23 (range, 14 to 37) months. The most common indication was hallux rigidus. Five patients had this procedure as a revision for failed osteotomies or fusion.
Indications for operation.
The patients were assessed in the specialist foot & ankle clinics preoperatively. Weightbearing radiographs of the foot (AP and lateral views) were performed in addition to a detailed clinical assessment (Figure 1, A and B). All the patients had a trial of non-operative methods before proceeding with surgery. All fusions were performed using the same technique and postoperative regime.

Preoperative AP (A) and lateral (B) weightbearing radiographs of foot showing severe hallux valgus. Postoperative AP (C) and lateral (D) weightbearing radiographs at 3 months showing satisfactory fusion.
Operative technique
The operation was performed using a dorsal approach in primary cases or using previous incisions in revision cases. The capsule was divided longitudinally medial to the EHL and the tendon was retracted laterally. The capsule and collateral ligaments were reflected from the metatarsal head and the FHL mobilized inferiorly. Thirty-four percent of cases had additional lesser toe surgery, mainly sliding Weil's osteotomy, interphalangeal joint fusion, and tenotomies.
The joint surfaces were prepared using spherical reamers to create concentric concave-convex surfaces. These two surfaces were reduced and temporarily fixed with a Kirschner wire in an optimum position. The sagittal alignment was checked intraoperatively using a flat tray to simulate weight-bearing. The metatarsophalangeal joint was positioned to allow a heel clearance of approximately 1 in, with simulated weightbearing. Any dorsal prominences were removed and the plate bent when necessary to allow proper seating and to maintain dorsiflexion. Valgus alignment was determined by the opposite side if normal or set at neutral. Rotation was kept to neutral using the nail plate as a guide. Final visual checks were made to make sure that the dorsiflexion angle was within the range of 15 to 25 degrees. The reduction was secured with an interfragmentary compression screw. A precontoured titanium alloy low profile plate (MTP arthrodesis Hallu-Fix System, Integra Extremity Reconstruction) was applied dorsally using their standard screws. Any minor local defects or cysts were filled with bone graft taken from the reamers. Wounds were closed in layers and a compression bandage applied. The patients were allowed to fully weight bear immediately in a flat post operative shoe with crutches if needed. The bandage was removed at 2 weeks. No plaster immobilization was used. At 6 weeks normal shoes were permitted. The patients were reviewed clinically and radiographically at 2 weeks, 6 weeks, 3 months, and 6 months. The hallux valgus angle, dorsiflexion angle, and angle of inclination were measured on weightbearing radiographs at 3 months (Figure 1, C and D). Any complications were noted. Functional outcomes were recorded by a telephonic interview and a review of radiographs and patient notes. We used the AOFAS Hallux Metatarsophalangeal-Interphalangeal scale. Since ten points are allotted for MTP joint motion only a maximum of 90 points was possible Fusion was confirmed when patients were pain free and radiographs showed bridging trabeculae or filling of the gap between the surfaces.
RESULTS
Of the 46 feet, the union rate was 98%. The average fusion time was 3.1 months. The average AOFAS score was 82.1 (range, 72 to 90). There were no deep wound infections or implant failures. One patient had a superficial wound infection which resolved with oral antibiotics. The hardware was removed only in the single patient who had a nonunion at 5 months due to persistent pain. The pain settled with the removal of the plate. The patient satisfaction rate was 100%. The average valgus angle on weightbearing radiographs at 3 months after operation was 17 (range, 9 to 21; median value: 16.5) degrees. The average dorsiflexion angle was 22 (range, 18 to 27; median value: 23) degrees. The average angle of inclination was 7.5 degrees.
DISCUSSION
A stable, pain free and reasonably aligned first metatarsophalangeal joint is crucial during the toe-off phase of gait. Trnka states that normally 50% of the body weight is carried by the big toe. In conditions affecting the MTP joint of the big toe, this force can be transferred laterally causing metatarsalgia and keratosis leading to overload and instability of the lesser MTP joints. 22 Fusion of the first MTP is a gold standard for some conditions affecting it. It eliminates painful motion and maintains stability and therefore increases the load bearing ability of the first ray. 11 In a recently published randomized controlled trial, Gibson established that outcomes after arthrodesis were better than those after arthroplasty. Arthoplasty led to an unacceptable level of stiffness and loosening and subsequent removal of implants whereas arthrodesis was clearly preferred by most patients. 10 Brodsky et al., in a prospective gait analysis showed that the arthrodesis of this joint produced objective improvement in the propulsive power, weightbearing function of the foot, and stability during the gait. 5
The success rate of fusion varies widely between 80%–100%.2–4,9,10,12,17,21. The joint surface preparation techniques, optimal angles of fusion and fixation methods seem to be the important factors in achieving a good outcome. There are many techniques described to prepare the joint surfaces. They may be cut flat or taper shaped. Flat and tapered cut surfaces give a large surface area but severely restrict the choice of angle. Curtis et al. in a biomechanical study, reported greater stiffness with the cup and cone method of arthrodesis when compared with the planar excision. 7 The dome shaped reamers provide surfaces which allow versatility and precise positioning. 16 Movement at the IP joint also affects the functional outcome of the MTP arthrodesis. It is therefore important to use a fixation device which does not affect the IP joint. Kirschner wires and other longitudinal intramedullary devices may be easy to use but have poor control of rotation and may affect the IP joint. There are reports of first metatarsal fracture when penetrated by Steinman pins or intramedullary screws. Two parallel or crossed screws can provide good fixation but may be technically difficult due to a limited cortical surface on the proximal phalanx. Staples are easy to introduce but are much less strong biomechanically.
Politi et al. in a recent biomechanical study compared the strength of fixation of five commonly utilized techniques of the first MTP joint fusion. 20 He used synthetic bone models to test the rigidity of fixation by stressing the joints by creating micromotion in dorsiflexion and by simulating the forces produced during the gait cycle. His findings have been summarized in Table 2. He found that the most stable technique was the combination of machined conical reaming with an oblique lag screw and dorsal plate. A single compression screw alone was the next strongest technique. A dorsal plate alone or Kirschner wire fixation were the weakest techniques. He did not however, include the crossed-screw technique in his study although it is a common method of fixation. This was however subsequently tested in a separate biomechanical study by Molloy et al. which showed that a single intramedullary screw was stiffer and stronger and biomechanically advantageous compared to crossed screws. 17 Politi et al. postulated that the low resistance of a plate alone technique to micromotion can be explained by the fact that the plate is applied on the dorsal side which is the compression side of the joint and is therefore at a biomechanical disadvantage.
Summary of absolute and relative strengths of different methods of fixation (Adapted from Politi J et al, FAI. 24, 2003)
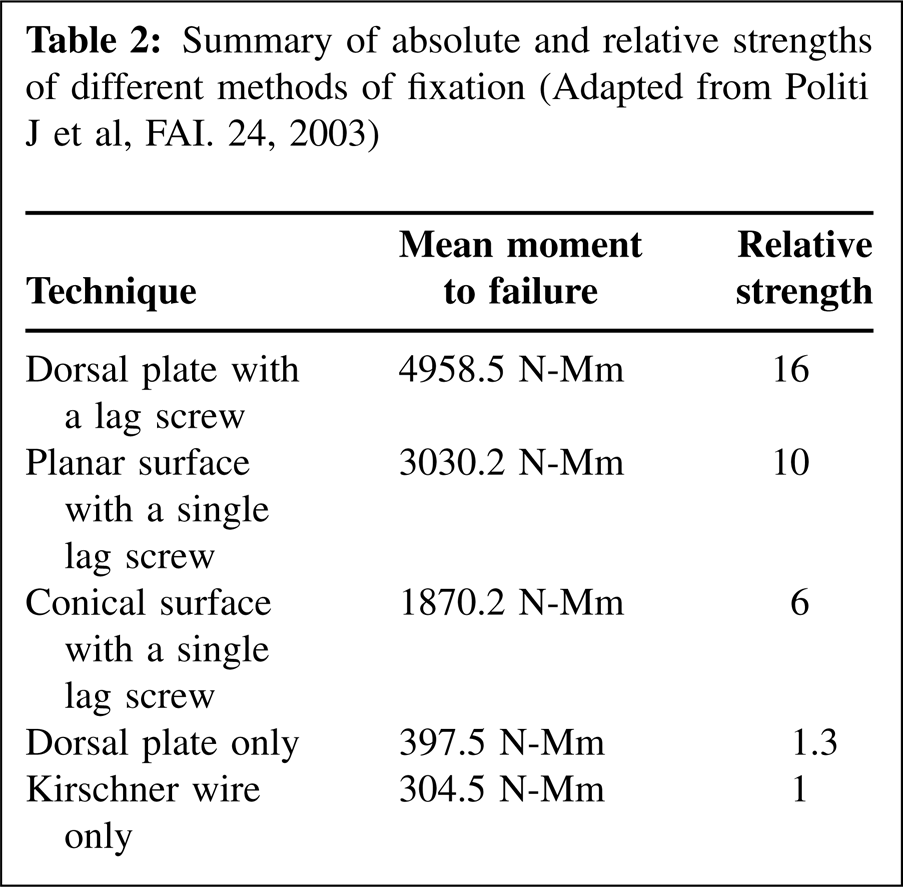
Plate design in itself is also very important. Bennett et al. published a series of 107 cases where ball and a cup surfaces were fashioned. 2 These were fixed using a compression screw and a plate from a hand set. There was high rate (13%) of metal fracture probably due to weakening of the plate by bending. This finding emphasizes the need for the right implant to preserve the anatomy and the kinematics of the joint. Specially designed plates also prevent an excessive dorsiflexion angle which is a common complication of the first MTP arthrodesis. 8 DeOrio stated that excessive dorsiflexion can occur either due to fixation without the use of a plate or when the non-specialty plates have been bent.
Various arthrodesis plates are now manufactured with contoured dorsiflexion angles of 9 to 10 degrees.1,19,23 Rigid fixation with the combination of these precontoured dorsal plates and a screw also allowed immediate full weight-bearing without a cast. Berlet et al. 3 in a recent series had a complication rate of 19% which included non-union in three (8.1%) and delayed union in two (5.4%) patients. The joint preparation techniques were variable and included those prepared with curettes and rongeurs. This technique is likely to have created poor bony apposition and stability, which would promote non-union. The fusion was also poorly stabilized by using a dorsal plate in isolation. On the contrary, Goucher and Coughlin have reported a 92% union rate along with 96% satisfaction rate in 49 patients by using a combination of a dorsal titanium plate and compression screw with surface preparation using concentric reamers. 12 There may be concerns about increased hardware related complications with an increase in the amount of metal but only one in 46 patients needed removal of hardware in our series. Goucher and Coughlin in their series of 49 patients also had a very low complication rate related to hardware.
We acknowledge that the study is not a controlled trial and provides only level IV evidence. The findings are nonetheless valuable to the practicing orthopaedic surgeon as randomized clinical trials are not always possible and Level I evidence may not be available for all clinical situations. 24 The main aim of this study was to evaluate the rate of fusion using this technique. A successful fusion does not always equate to a successful result and therefore we have included the post operative alignment and functional scores. The study was not designed to assess the functional improvement from this operation, as this has previously been very well established and therefore pre-operative scoring has not been included.2,4,10,12,22
The question of cost is an important factor in choosing the appropriate operation and fixation device. Hyer and Lee published work showing a significant cost difference with two techniques: Mean implant costs for crossed screws was $374 whereas for a dorsal plate it was $603.15 Our cost analysis prices the crossed screws at £54 and the dorsal plate and lag screw at £450. There is a large difference in implant costs, but this needs to be weighed against the significantly higher fusion rate, better control over position of the fused joint, better patient satisfaction and earlier mobilization possible which indirectly means earlier return to work. Non union, delayed union and delayed weightbearing can pose far more costs in addition to causing emotional distress. These costs are even higher in patients with comorbidites like diabetes and neuroarthropathy and this group has been excluded in an analysis by Hyer et al. 15
CONCLUSION
First MTP joint fusion with spherical reamers and a low-profile contoured dorsal titanium plate and lag screw was highly successful, with excellent patient satisfaction and functional outcomes.