
Abstract
Background: Controversy exists about the role of metatarsus primus elevatus (MPE) in the presence of hallux rigidus. Previous studies could neither confirm nor reject a causative relationship. Measurement of the true elevation of the first metatarsal according to current techniques lack either precision or accuracy or both. The purpose of this study was to assess MPE by means of a new radiographic measurement method and to analyze how the MPE-values differed among hallux rigidus, hallux valgus and control groups. Materials and Methods: A retrospective study was performed of standing AP and lateral radiographs of 295 feet (221 patients; average age 54 years) randomly selected from our databank. According to general radiographic and clinical criteria, 99 were defined as hallux rigidus. Ninety-nine feet had a hallux valgus deformity without severe arthritis. Ninety-seven radiographs with normal MP-I joints and no other forefoot deformity served as a control group. The elevation of the first metatarsal bone in relation to the second metatarsal (MPE), the first metatarsopahlangeal dorsiflexion angle (DFA), the hallux valgus angle (HVA), the intermetatarsal angle (IMA), the interphalangeal angle (IPA) and the degeneration of the first metatarsophalangeal joint were measured. Three independent raters were involved to assess the inter-rater reliability of a new MPE measurement method. For statistic analyses, ANOVA testing was used. Results: MPE was significantly greater in patients with hallux rigidus (+5.2 mm; 95% CI: 4.7 to 5.7) when compared with hallux valgus (+2.8 mm; 95% CI: 2.2 to 3.4) or the control group (+2.6; 95% CI: 2.0–3.2; p < 0.0001). The DFA was found to be significantly lower in the hallux rigidus group (9 degrees; 95% CI: 8 to 10) when compared with those measured in the hallux valgus (14 degrees; 95% CI: 13 to 16) and control groups (11 degrees; 95% CI: 10 to 12; p < 0.0001). There was a no correlation found between MPE and osteoarthritis at MP-I joint (r = 0.35; p < 0.0001). A moderate correlation was found between increasing MPE and decreasing DFA (r = 0.5; p < 0.0001). The inter-rater reliability of the MPE measurement method was found to be accurate and reproducible (r = 0.9; p < 0.0001). Conclusion: Based on the findings in this study, an MPE greater than 5 mm could be considered a predictive factor in the presence of hallux rigidus. However, the mechanism of MPE has yet to be determined.
Level of Evidence: III, Case Control Series
INTRODUCTION
Hallux rigidus describes a painful limitation of motion at the first metatarsophalangeal joint, usually associated with degeneration of the MP-I joint. Several causative factors for hallux rigidus have been reported including trauma, osteochondritis dissecans, hereditary factors and/or anatomical aberrations such as forefoot pronation, hallux valgus deformity, a long first ray or metatarsus primus elevatus. 1–3,11,16,17,22–24,26,28–30,32,37 The role of metatarsus primus elevatus in hallux rigidus remains enigmatic. Metatarsus primus elevatus describes a dorsal elevation of the first metatarsal bone in relation to the lesser metatarsals. First described by Lambrinudi in 1938 it was considered a hereditary causative force in the development of hallux rigidus. It was thought that correction of the elevated first metatarsal could positively affect range of motion at the MP-I joint and thus be used to treat hallux rigidus.2,4–6,13,15,22,27,33,34 While many investigators shared this opinion, there are others who confirmed MPE to be a nonspecific radiographic variation, which could also be found in healthy subjects.3,21,31 A thorough review of the literature reveals that there is no reliable threshold value to define “the” pathologic value of MPE. Additionally, current assessment methods to investigate MPE on conventional radiographs lack precision or accuracy or both. This is confirmed by several independent studies using the same method of measurement resulting in different threshold values of MPE.11–35 Based on those findings, the question whether an elevated first metatarsal bone relative to the second metatarsal is a causative and/or a pathognomonic factor in the presence of hallux rigidus remains unanswered.
The purpose of the present radiographic analysis was to determine MPE in feet with obvious MP-I pathology (hallux rigidus and hallux valgus) and in feet with a normal MP-I by means of a new, reliable and validated method of measurement and to define a threshold value. We hypothesized that MPE would be significantly greater in patients with hallux ridigus when compared with hallux valgus patients or in patients with morphologically normal feet.
MATERIALS AND METHODS
A retrospective analysis of the hospital's database was performed to identify patients who had hallux rigidus, hallux valgus or interdigital neuroma (Morton's neuroma). Patients were randomly retrieved and grouped according to their pathology (i.e., hallux rigidus and hallux valgus) or as control subjects. The study was approved by the local IRB of our institution. Exclusion criteria included diabetes, rheumatoid arthritis, other inflammatory or infectious arthritis, gout, pseudogout, poliomyelitis and other neuromuscular diseases, patients with multiple forefoot/hindfoot deformities and those who had previous surgeries of the foot and ankle.
Two hundred twenty-one adult patients (295 feet) were randomly enrolled for the study. The average age of the entire study population was 54 (range, 21 to 85) years. All patients were grouped according to their underlying pathology: Group 1 included 99 feet (83 patients; 57% male, 43% female) having hallux rigidus. The mean age in this group was 56 years (range 23 to 85). Group 2 comprised of 99 feet (66 patients; 12% male, 88% female) with hallux valgus deformity. The mean age was 54 years (range 26 to 85). Group 3 was defined as control group including 97 feet of 72 patients (19% male, 81% female) having Morton's neuroma. To be included in the control group, each patient had no skeletal forefoot aberration on conventional radiography. The mean age in this group was also 54 (range, 21 to 77) years. 9
A standardized technique was used to obtain the digital radiographs. The AP and lateral radiographic views were taken while having the patient stand in an upright, full weightbearing position. The film-focus distance measured 120 cm and the radiation exposure was 55 kV/5mAs. The AP views were performed while inclining the beam 20 degrees in the sagittal plane for optimal exposure of the mid- and forefoot joints. The lateral views were obtained with the beam oriented from lateral to medial with the film in direct contact to the medial malleolus. To get an exact overlap of the two malleoli, the whole foot was held in 20 degrees of internal rotation.
All angles and distances were digitally measured by means of the PACS image viewer (Cerner Corporation, Kansas City, MO). All measurements were done according to the guidelines of the American Orthopaedic Foot and Ankle Society (AOFAS) Committee on Angular Measurements. 9
Lateral radiographic measurements
MT-1-Declination angle: 21 Angle between longitudinal axis of the first metatarsal bone and the ground. The longitudinal axis of MT-1 was defined as centerline between the dorsal and plantar cortical bone (Figure 1).

The figure describes how the MT-1-Declination angle was measured. The MT-I-declination angle is mean angle between longitudinal axis of the first metatarsal bone and the ground. The longitudinal axis of MT-1 was defined as centerline between the dorsal and plantar cortical bone.
MT-2-Declination angle:21 Angle between longitudinal axis of the second metatarsal bone and the ground. The longitudinal axis of MT-2 was defined as centerline between the dorsal and plantar cortical bone (Figure 2).

MT-2-Declination angle: Angle between longitudinal axis of the second metatarsal bone and the ground. The longitudinal axis of MT-2 was defined as centerline between the dorsal and plantar cortical bone. Difference between MT-1 and MT-2 Declination: According to the measurements of Horton et al. in 1999 also the difference of the two mentioned declination angles were defined.
Difference between MT-1 and MT-2 Declination: According to the measurements of Horton et al. the difference of the two mentioned declination angles were defined.
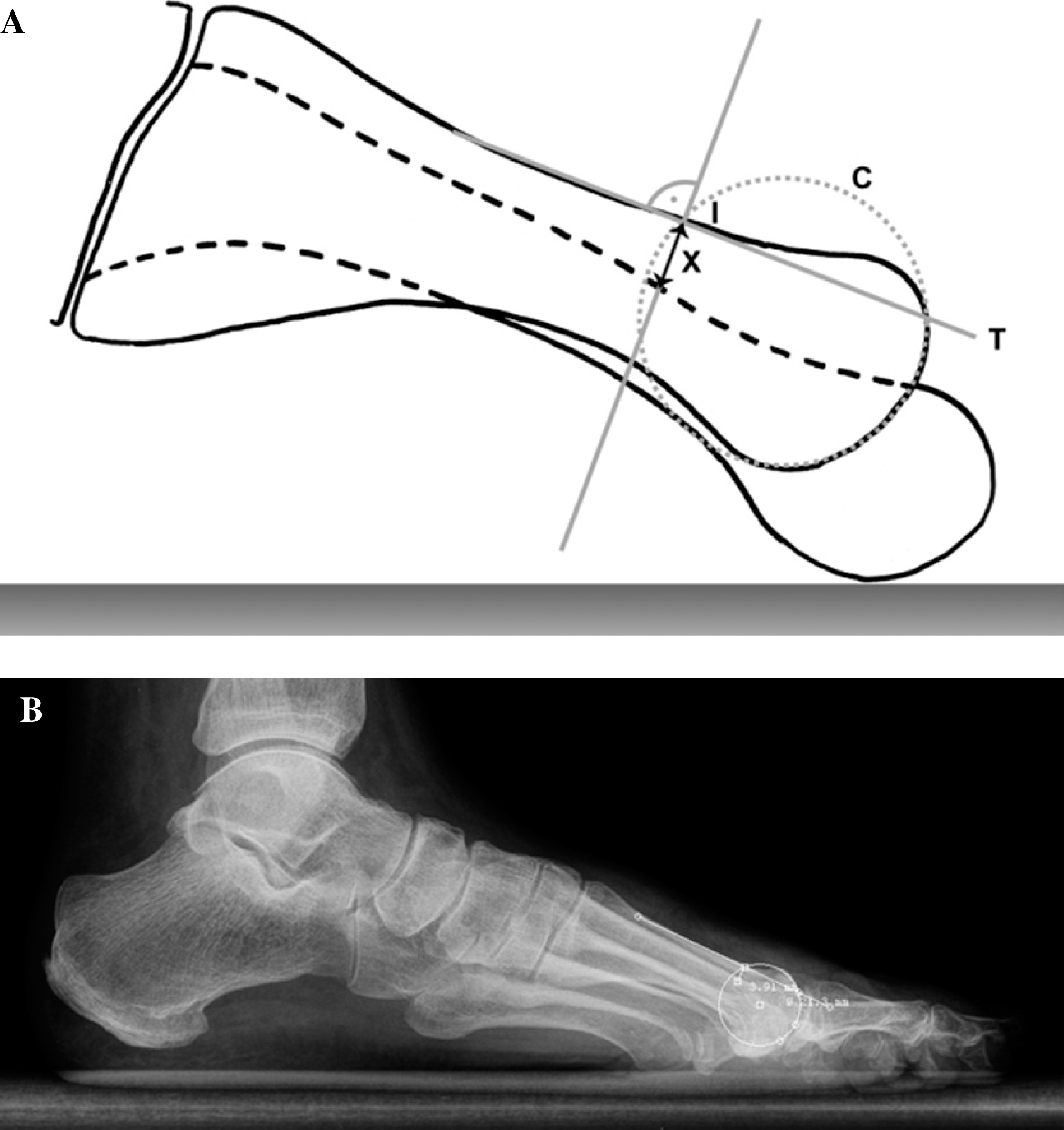
Metatarsus primus elevatus (MPE): To measure the elevation of the first in relation to the second meatatarsal bone a new method was used. First a circle was fit in the metatarsal head such that a congruency between circle and the joint surface could be achieved. Then a tangent line was drawn along the dorsal cortical bone of the first metatarsal shaft.
At the proximal point where the circle cut the tangent line, a vertical 90 degrees angle-line was drawn down to the dorsal cortical bone of the second metatarsal shaft. The distance between the two intersection points of the two dorsal cortical bones along the vertical line determined the MPE (Figure 3).
Lateral TMT-1-Version:9 Angle between the proximal joint surface of the medial cuneiform and a perpendicular line to the ground (Figure 4).

Lateral TMT-1-Version: Angle between the proximal joint surface of the medial cuneiform and a perpendicular line to the ground.
MT-1 Dorsiflexion-angle (DFA): Angle between the longitudinal axis of the MT-1 shaft and the longitudinal axis of the proximal phalanx (Figure 5).

MT-1-Dorsiflexion-angle (DFA): Angle between the longitudinal axis of the MT-1-shaft and the longitudinal axis of the proximal phalanx.
AP radiographic measurements
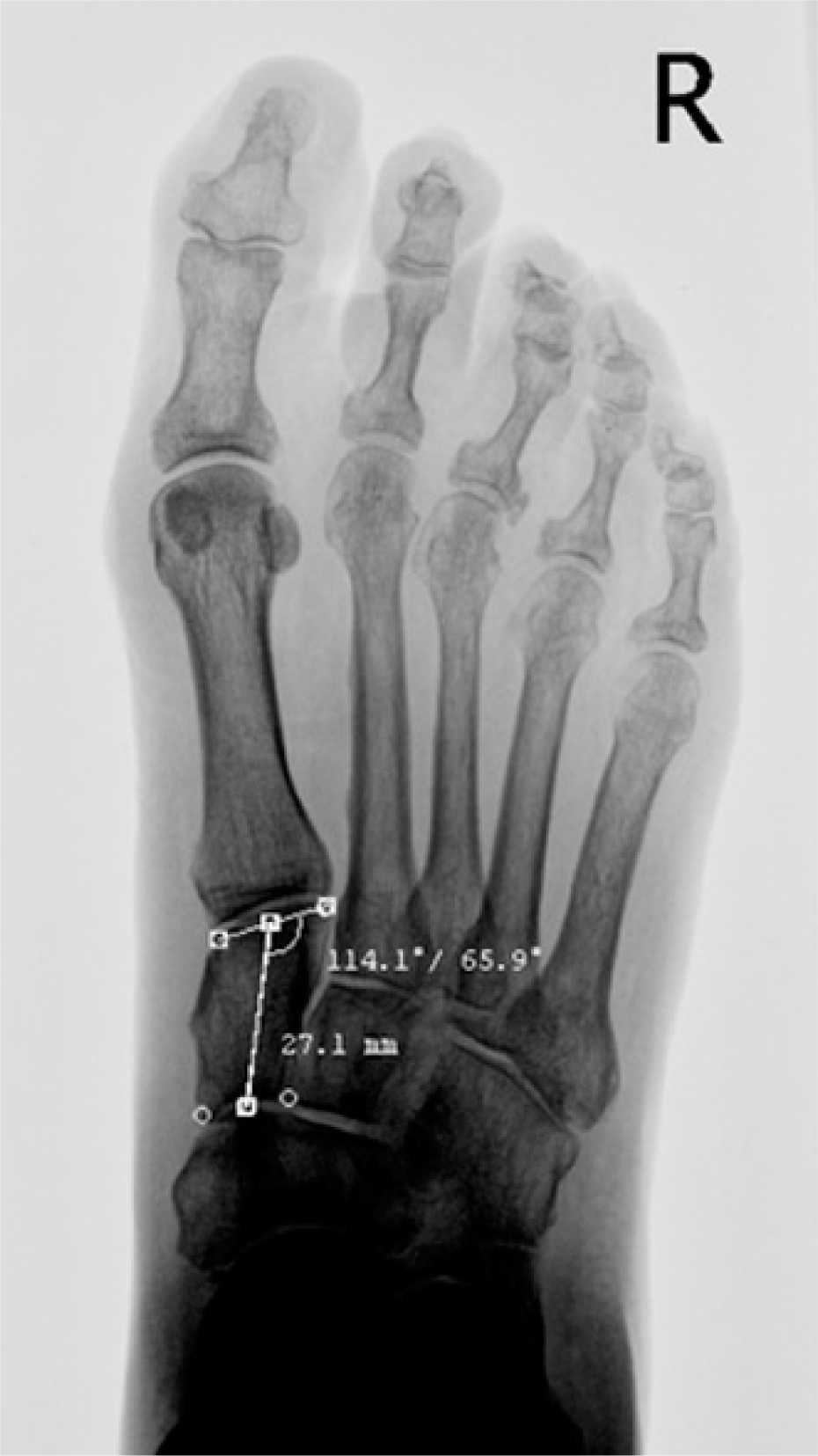
Hallux valgus-angle (HVA): Angle between the longitudinal axis of the MT-1 shaft and the longitudinal axis of the proximal phalanx (Figure 6). 9

Hallux valgus-angle (HVA): Angle between the longitudinal axis of the MT-1-shaft and the longitudinal axis of the proximal phalanx according to the guidelines of the American Orthopaedic Foot and Ankle Society (AOFAS) Committee on Angular measurements.
Intermetatarsal-angle (IMA): Angle between the longitudinal axis of the MT-1 shaft and MT-2 shaft (Figure 7). 9

Intermetatarsal-angle (IMA): Angle between the longitudinal axis of the MT-1-shaft and MT-2-shaft according to the guidelines of the American Orthopaedic Foot and Ankle Society (AOFAS) Committee on Angular Measurements.
Interphalangeal-angle (IPA): Angle between the longitudinal axis of the proximal and distal phalanx of the great toe (Figure 8). 9

Interphalangeal-angle (IPA): Angle between the longitudinal axis of the proximal and distal phalanx of the first ray according to the guidelines of the American Orthopaedic Foot and Ankle Society (AOFAS) Committee on Angular Measurements.
Dorsoplantar TMT-1 Version: Angle between the longitudinal centerline of the medial cuneiform and the tangent line to the distal joint surface of the medial cuneiform (Figure 9).
Dorsoplantar TMT-1-Version: Angle between the longitudinal centreline of the medial cuneiform and the tangent line to the distal joint surface of the medial cuneiform.
Hallux rigidus and MP-1 osteoarthritis: The degree of degenerative joint disease in the first metatarsophalangeal joint was measured according to the radiographic classification of Hattrup and Johnson from 1988. Grade I was defined as mild to moderate osteophyte formation but preservation of joint space, Grade II moderate osteophyte formation, joint narrowing and subchondral sclerosis and Grade III with marked osteophyte formation, loss of the visible joint space ± subchondral cyst formation. 19
Three independent raters assessed the MPE according to the new measurement method and the inter-rater-reliability was calculated to assess the reliability. A oneway analysis of variance (ANOVA) multiple comparison test was used for statistical analysis. Statistical significance was defined as p < 0.01. For all results confidence interval (CI) ranges were calculated. In order to assess the inter-reliability of the proposed measurement method, the Spearman correlation coefficient was calculated.
RESULTS
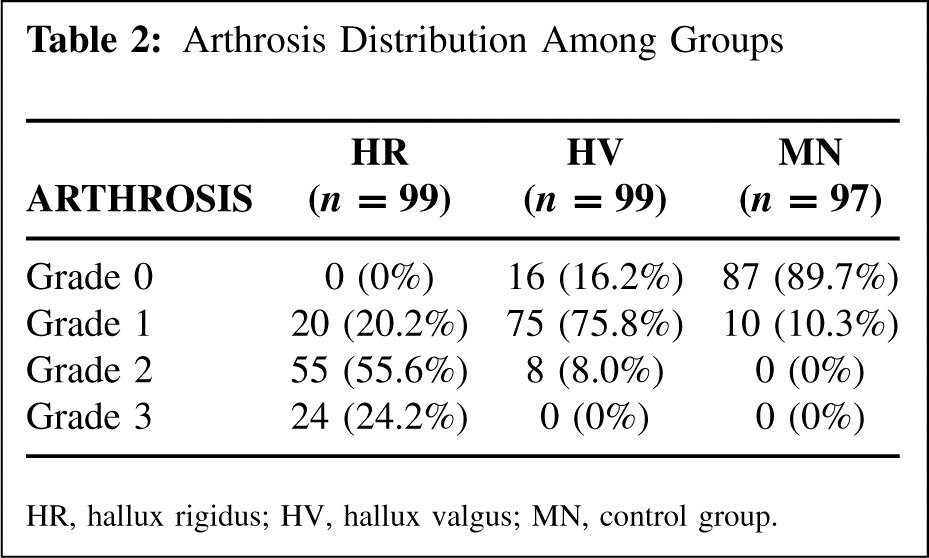
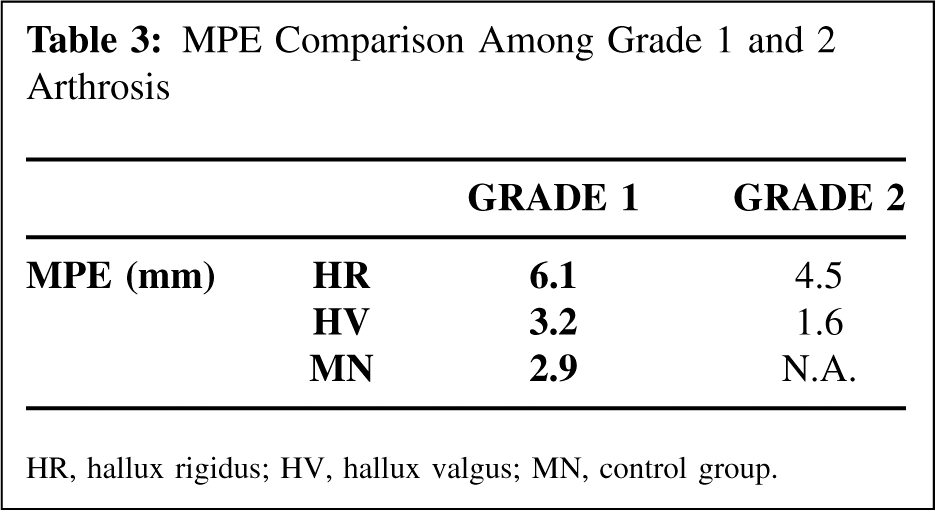
A synopsis of the entire dataset is given in Table 1. Table 2 demonstrates the distribution of arthrosis among all three groups. Patients with hallux rigidus had a statistically significant (p < 0.0001) greater MPE value (MPE: +5.2 mm; 95% CI: 4.7 to 5.7 mm) when compared with those having hallux valgus (MPE: +2.8 mm; 95% CI: 2.2 to 3.4 mm) and those of the control group (MPE: +2.6 mm; 95% CI: 2.0 to 2.3 mm). A separate analysis of MPE for grade 1 and grade 2 arthrosis was done (Table 3) and revealed greater MPE values in the hallux rigidus group. Additionally, the DFA was found to be significantly lower (DFA: 9 degrees; 95% CI: 8 to 10 degrees; p < 0.0001) in the hallux rigidus group compared with the hallux valgus group (DFA: 14 degrees; 95% CI: 13 to 16 degrees) and control group (DFA: 11 degrees; 95% CI: 10 to 12 degrees). Only a small positive correlation between stage of osteoarthrosis and the amount of MPE was found (r = 0.35; p < 0.0001). There was a positive correlation between amount of DFA and MPE (r = 0.5; p < 0.0001). The new MPE measurement method was reliable and reproducible with an inter-rater reliability of 92% (p < 0.0001). The other data (Table 1) showed no significant differences between the three groups.
Parameter Synopsis
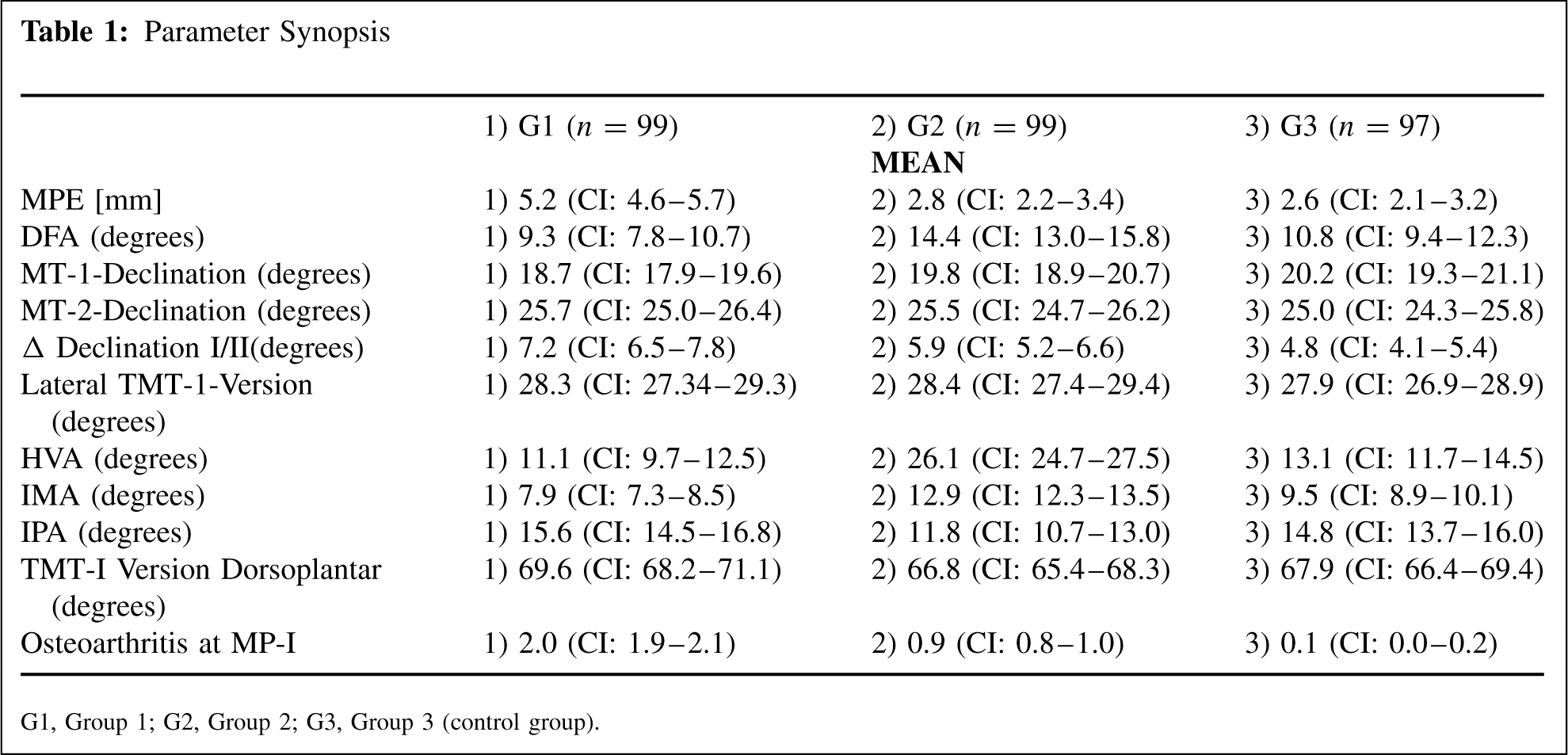
G1, Group 1; G2, Group 2; G3, Group 3 (control group).
Arthrosis Distribution Among Groups
MPE Comparison Among Grade 1 and 2 Arthrosis
HR, hallux rigidus; HV, hallux valgus; MN, control group.
DISCUSSION
Since its first description by Lambrinudi in 1938, metatarsus primus elevatus (MPE) and its specific role in the pathogenesis of hallux rigidus has remained an issue of debate. While many authors believed that it could be a causative factor leading to degeneration and thus hallux rigidus,2,4,5,6,13,15,22,36, other investigators did not.3,21,28 Horton and coworkers presented a measurement technique for MPE. A vertical distance of more than 7.8 mm between the first and second metatarsal cortices was defined as pathologic. 21 Other authors adopted the same method to investigate MPE and hallux rigidus but arrived at different threshold values of 6.8 mm and 5.8 mm, respectively.3,10,11 The main problem encountered with Horton's method is the lack of standardization and validation, which we believe explains the large variability of values obtained in different studies.
A clearly defined threshold value may have a direct impact on diagnosis and thus therapeutic measures. Those who believe that MPE is a cause of hallux rigidus, for example, recommend corrective metatarsal osteotomies.2,4–6,13,15,22,27,33,34 The present study introduces a new method, which generates reproducible and reliable data. Based on the controversial data in the literature, we aimed to show if a specific relation between an increased MPE existed in the presence of hallux rigidus. The comparison of the results obtained by the new measurement method with those reported in the literature showed that an MPE greater than 5 mm could be seen as a predictive factor for hallux rigidus. In contradiction to previous investigations, which postulated an elevated MPE to be a physiologic radiographic finding even in patients with a healthy MP-I joints, 21 we found a direct association between the presence of hallux rigidus and an MPE exceeding 5.0 mm. We chose a lower threshold value in our study as a result of the new measurement approach, which demonstrated a high reproducibility.
Based on Lambrinudi's case report and others who suspected a flexion contracture in the first metatarsophalangeal joint to be a pathogenetic factor in the evolution of hallux rigidus, we also measured the lateral dorsi-flexion angle (DFA). The DFA of 9 degrees was significantly lower in the hallux rigidus population which we believe supports Lambrinudi's original suggestion. Recent biomechanical investigations support this theory showing a rising joint reaction force in the MTP-I joint due to diminished excursion of the flexor hallucis longus tendon. 25 One possible future approach could be to investigate the biomechanical influence of flexor hallucis longus muscle and tendon function in hallux rigidus. 25 Tendon function could either be altered by muscle contracture, adhesions at the plantar plate or due to dorsal osteophytes. However, no information is currently available to support any of those theories.
An aberrant tarsometatarsal joint is not necessarily linked to an elevated first metatarsal. The current study confirms this statement by comparable measurements of the lateral and AP TMT-1 version. With regard to previous studies, we also measured the MT-1 and MT-2 declination angle, the hallux valgus angle (HVA), the intermetatarsal angle (IMA), the interphalangeal angle (IPA) and the radiographic degree of osteoarthritis in the MTP-1 joint. The current data demonstrated a consistent relationship between MPE values over 5 mm in patients with hallux rigidus. The poor positive relation between osteoarthritis and MPE suggests an elevated MPE is an independent parameter in the presence of hallux rigidus and that it might be caused by other mechanisms than degeneration alone. Our results are similar to those published by Horton et al. One limitation of the present study is the use of Morton neuroma patients as control group. This, of course, does not represent an overall healthy foot control group. However, we adhered very strictly to the inclusion criteria, which required normal radiographic appearance of foot anatomy including absence of MP-I pathology. Therefore, we think that the values obtained in the 5 study could be used for comparison. The current investigation cannot explain the underlying mechanism of MPE. Besides this we did not investigate whether the measurement method could be susceptible to or not feasible due to anatomical variation and/or alteration of the first metatarsal head such as osteonecrosis of the first metatarsal head with subsequent flattening of the joint surface. Further investigations have to be undertaken to elucidate the evolution and causative factors related to hallux rigidus and why MPE is characteristic for this specific pathology.
CONCLUSION
Based on a standardized radiographic assessment and a simple, reliable measurement method, we showed that an MPE greater than 5.0 mm seems to be predictive for the presence of hallux rigidus. The exact mechanism of MPE has still to be determined.
EDITOR'S NOTE
The authors are to be congratulated for developing a more reliable method of measurement of the MPE. It will be interesting to see whether other investigators find a similar correlation with an elevated MPE and hallux rigidus and whether the actual mechanism for this relationship can be established, i.e., is the elevated MPE the cause or effect of the hallux rigidus? Also, there was a significant preponderance of females in the hallux valgus and control patients in this study which may have affected the results.