
Abstract
Level of Evidence: V, Expert Opinion
INTRODUCTION
Although rarely indicated for hip and knee joint disorders, arthrodesis is still a common surgical procedure for ankle joint disorders such as end-stage degeneration, inflammation including rheumatoid arthritis and infection, and avascular necrosis of the talus.1,5 Recently, arthroscopic ankle arthrodesis has been performed widely and several satisfactory outcomes after surgery have been reported.4,20 Although the greatest advantage of arthroscopic arthrodesis is that it is a less invasive procedure to surrounding soft tissues, which leads to quicker radiographic union and higher fusion rate than ordinary open arthrodesis,13,14 the indications for this procedure include minimal deformity. Generally, valgus or varus deformity of more than 10 to 15 degrees in the coronal plane needs correction by an open procedure.1,4,13,14,20
There are several types of fixation techniques for open ankle arthrodesis such as use of compression screws,7,9 screw with plate system,10,18 and external fixator. 16 The most frequently encountered complication associated with open ankle arthrodesis has been nonunion.1,6,15 The reported nonunion rate from one review of ankle arthrodesis with outcomes of 126 cases was 41%. The major problems contributing to nonunion have been inadequate bony surface contact and poor fixation. 1 In 1943, Blair described a procedure of tibiotalar fusion fixated with an anterior sliding bone graft for cases of loss or collapse of the talar body. Although the use of this procedure alone has not been reliable,3,5,8 it does bring about adequate bony contact between the tibia and the talar head and we believe a higher fusion rate can be expected if this technique is combined with some rigid internal fixation technique.
Recently, development of locking compression plates which act as angular stabilizers has improved the outcome of fracture care. 19 Effective fixation by these types of plates for cases with poor bone quality have been reported.11,17 To achieve adequate bony surface contact and more rigid fixation, we have recently applied internal fixation using a locking compression plate combined with anterior sliding bone graft for open ankle arthrodesis. We have used this procedure not only for ankle disorders with severe deformity, but also for avascular necrosis of the talus.
TECHNIQUE
The patient is placed in the supine position with a pneumatic tourniquet placed on the ipsilateral thigh, under general or lumbar anesthesia. The pneumatic tourniquet is inflated to a pressure of 300 mm Hg. The ankle joint is exposed through an anterior approach. After incision into the extensor retinaculum, the tibialis anterior tendon is retracted medially and the extensor hallucis longus and neurovascular bundle is retracted laterally. The neck of the talus is exposed along with the anterior surface of the distal tibia. Then resection of osteophytes and intraarticular debridement including resection of remaining cartilage and synovectomy are performed (Figure 1). After intraarticular debridement, drilling of the tibial and talar surfaces using a 1.5-mm Kirschner wire similar to an arthroscopic drilling technique for osteochondral lesions is performed. We do not recommend the use of a drill with a large size as contact area between the tibia and talus is reduced and which may result in delayed union or nonunion.
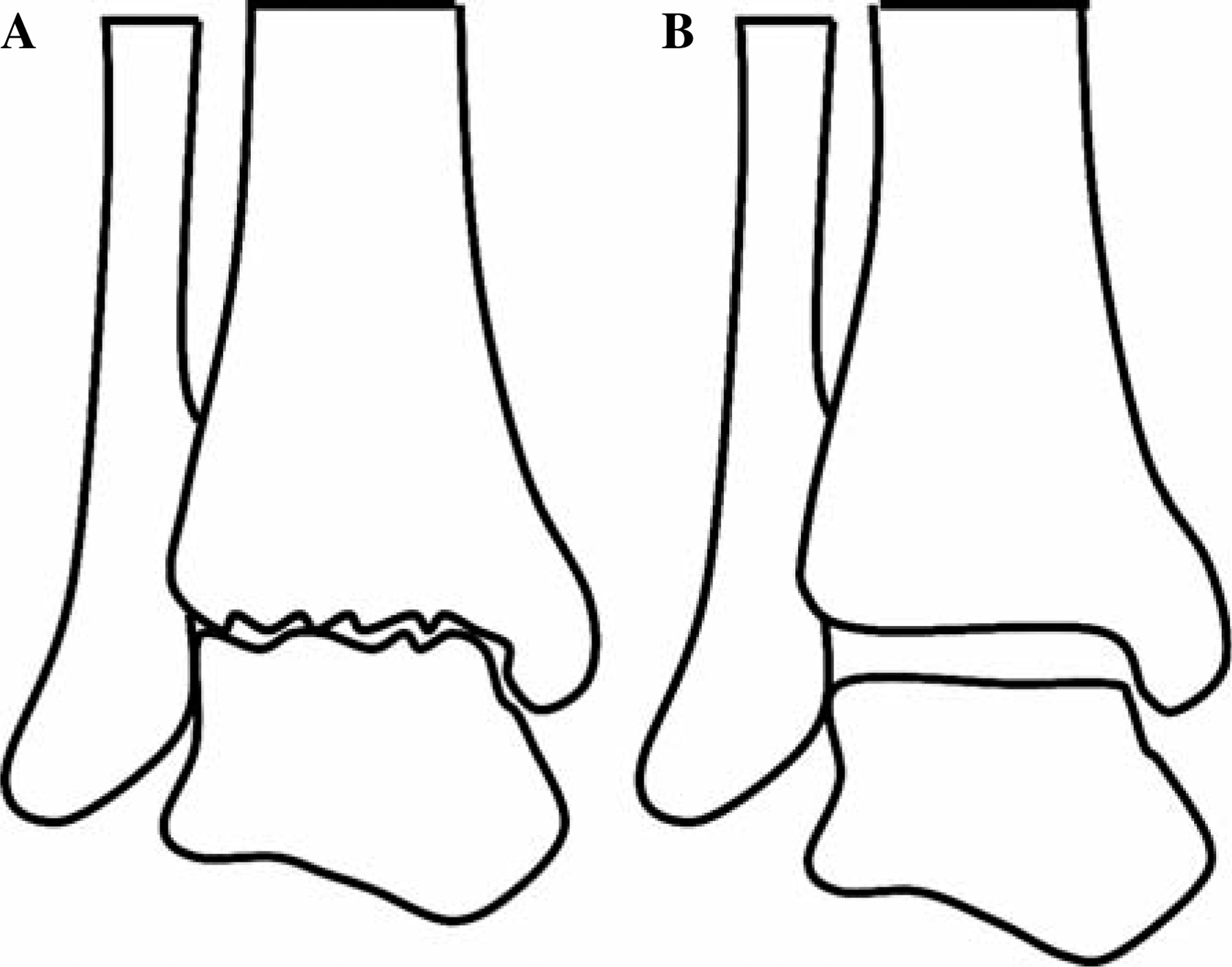
Schematic diagram showing before (A) and after (B) intra-articular debridement of an affected ankle joint.
Next, the anterior tibial sliding bone graft is performed. A tibial graft in the shape of a triangular column with the size of approximately 5 cm in length and 1 cm wide is created using a saw in the lateral half of the distal tibia. The talus is positioned so that the forefoot is in slight external rotation and the hind foot is in 5 degrees of valgus position with slight dorsiflexion of the talocrural joint, and the point within the surface of the talus which is to come into contact with the anterior bone graft after inferior sliding is marked. At the marked point, a triangular bone tunnel matched to the bottom of the bone graft is created with the depth of approximately 1 cm using an osteotome (Figure 2). After sliding of the anterior bone graft, two or three cortical screws are inserted into the tibial part of the graft and a cancellous screw is inserted into the talar part to fix it rigidly (Figure 3).
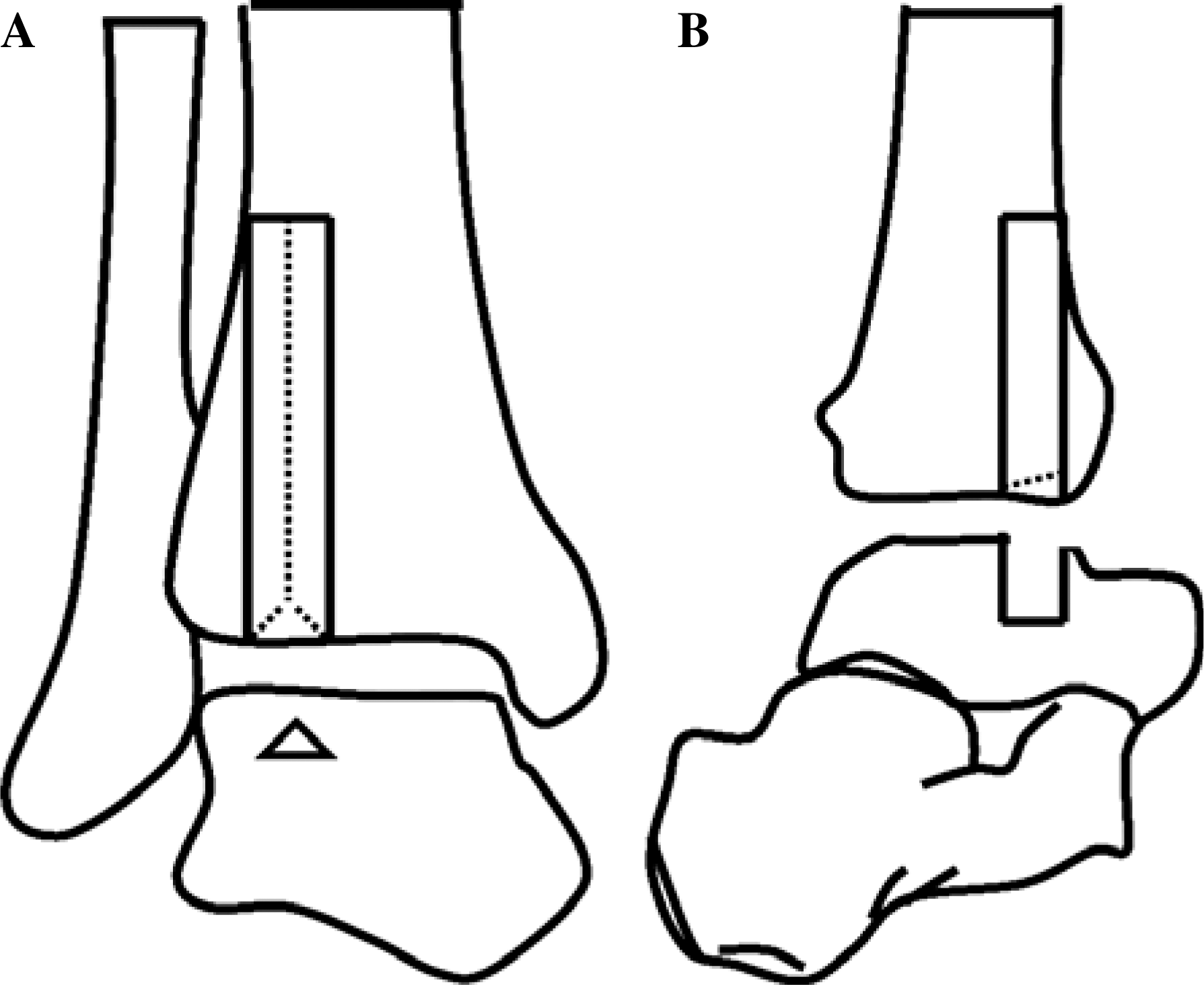
Schematic diagram of AP (A) and lateral (B) views showing creation of a triangular column-shaped tibial graft approximately 5 cm long and 1 cm wide and a triangular accepting bone tunnel in the talus approximately 1 cm deep.
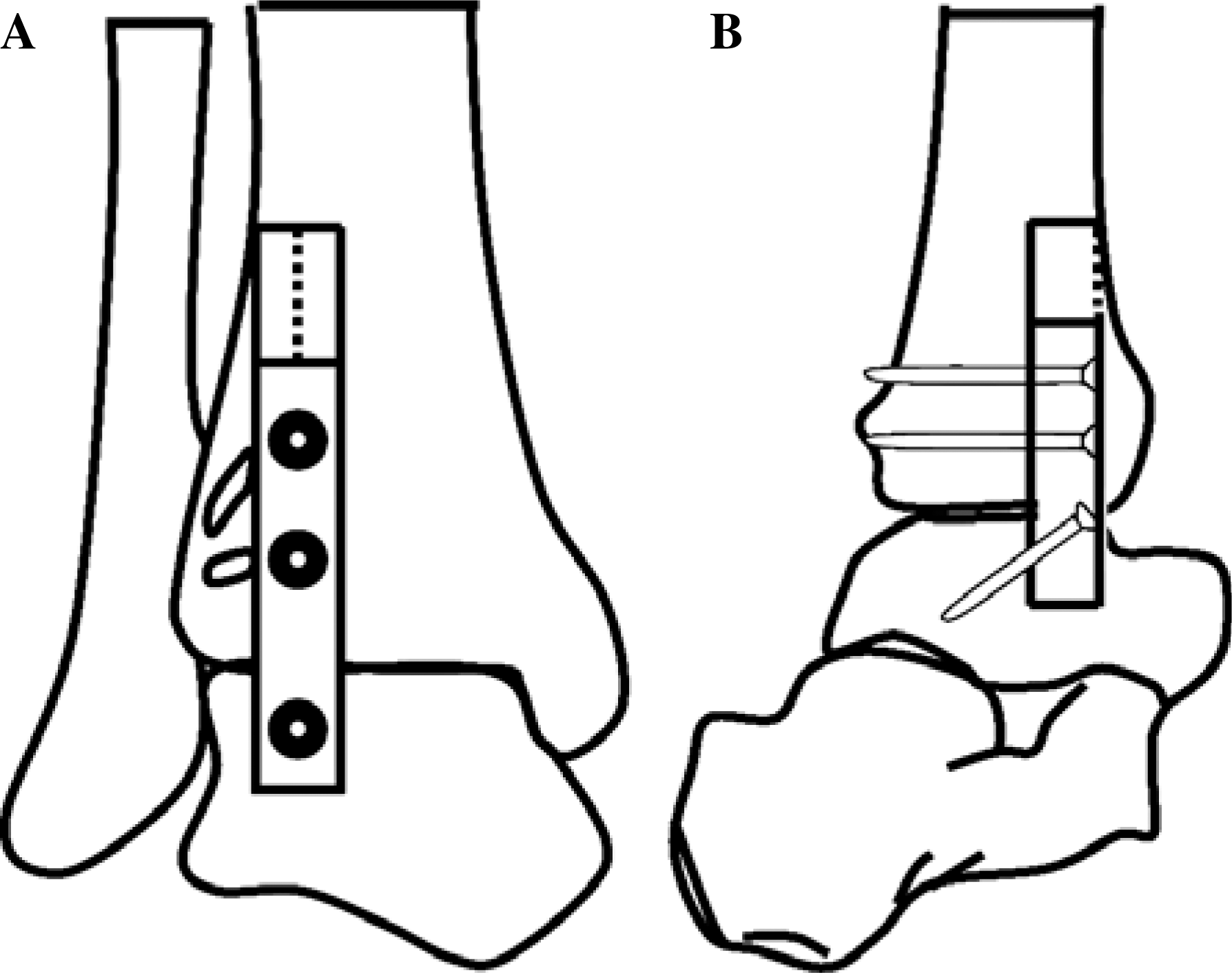
Schematic diagram of AP (A) and lateral (B) views showing fixation of an anterior bone graft after inferior translation.
Then internal fixation using a locking compression plate (LCP reconstruction plate 3.5; Synthes, Bettlach, Switzerland) is performed. Plate modification is made using a vise to adapt to the configuration of the anterior ankle, and internal fixation using locking screws for several holes is made between the tibia and talus (Figure 4). Finally, any gap between the tibial and talar surface is filled with cancellous bone chips harvested from the ipsilateral iliac crest (Figure 5).
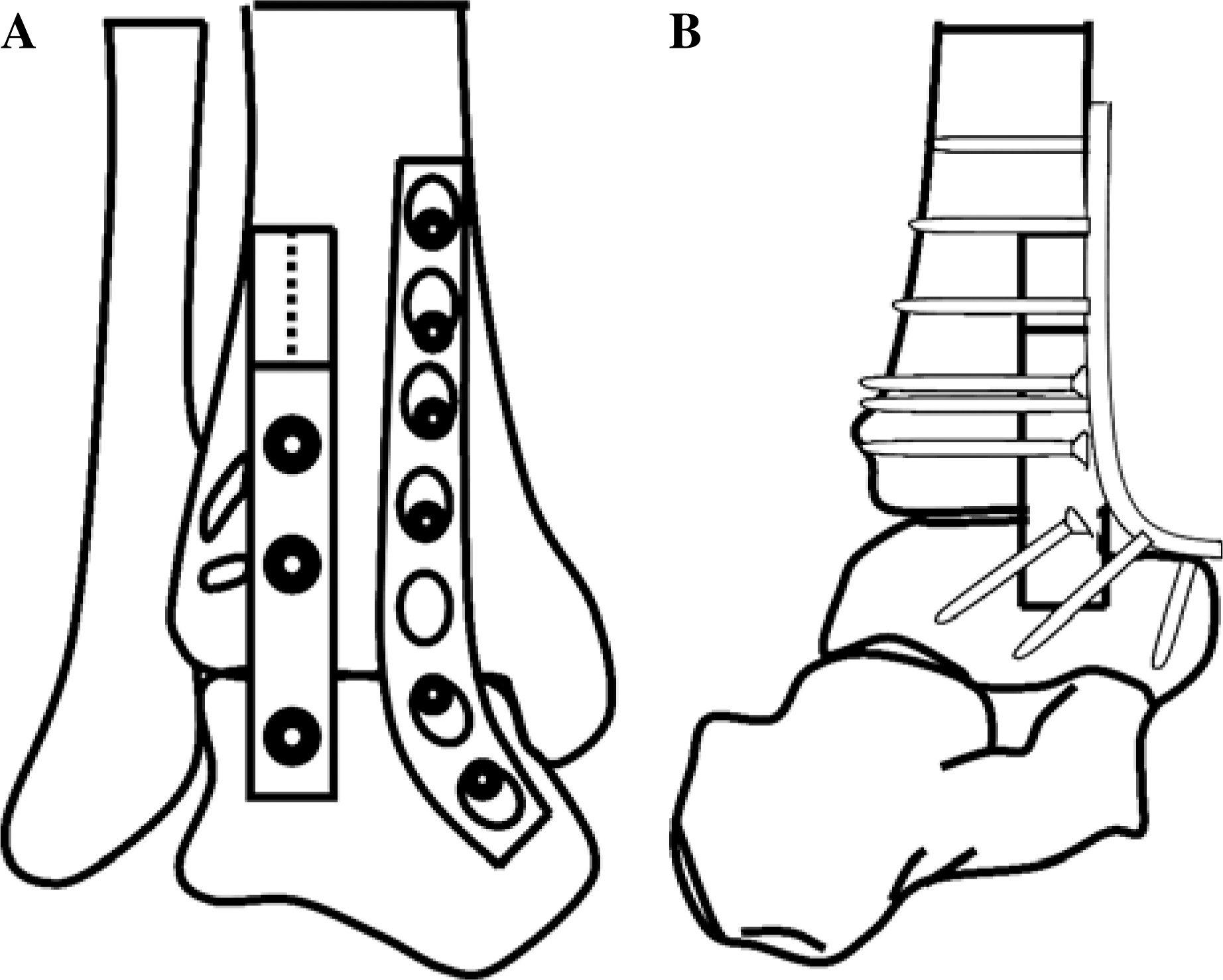
Schematic diagram of AP (A) and lateral (B) views showing an ankle arthrodesis using locking compression plate combined with anterior sliding bone graft.

Plain AP (A) and lateral (B) radiographs immediately after surgery.
Postoperatively, a splint is applied until wound healing and toe touch gait is allowed after 4 weeks. At 6 weeks after operation, the patient advances to full weight bearing if pain is tolerated.
Our procedure was performed on eight patients; five with end-stage osteoarthritis with severe deformity, and three with avascular necrosis of the talus. All patients achieved complete fusion by 10.3 weeks after surgery without complication. The mean American Orthopaedic Foot and Ankle Surgeons ankle and hindfoot score at 1 year after surgery was 89.7 points (Figure 6).

Plain AP (A) and lateral (B) radiographs of same case as Figure 5 at 2 years after surgery.
DISCUSSION
There are several types of fixation procedures which have been applied for open ankle arthrodesis.7,9,10,16,18 The most widely used fixation procedure is cancellous screw fixation, and this procedure has brought about relatively favorable fusion rates.7,9 The fusion rate using screw fixation reported by Holt et al 7 was 74% and that reported by Frey et al. 6 was 66%. To gain more rigid internal fixation, anterior plating techniques have been developed with higher fusion rates.10,18 Sowa and Krackow 18 applied an anterior plating technique using a modified dynamic compression pediatric blade plate with lateral fibular strut augmentation for ankle disorders such as post-traumatic degenerative arthritis, rheumatoid arthritis and ischemic necrosis of the talus, and their reported fusion rate was 94%. However, their procedure requires two incisions including a straight lateral incision and a gently curving anteromedial incision, which is more invasive than other procedures. Mears et al. 10 used an anterior tension plate technique for open ankle arthrodesis and reported a fusion rate of 82%. Although this fusion rate is higher than fusion rates for other procedures, their indication was cases with minimal deformity or bony destruction.
One characteristic of our present technique is the use of a locking compression plate which was originally developed to improve fracture care. 19 Angular stability due to the locking mechanism is the greatest advantage of this type of plate, and more rigid internal fixation can be expected with it than with use of an ordinary non-locking plate in a case where bone quality is poor. 19 Another characteristic is application of an anterior sliding bone graft for adequate anterior contact between the tibia and talus.
The original procedure for tibiotalar arthrodesis after removal of the talar body was described in 1943 by Blair, and various modifications such as addition of screw fixation to bone graft or talocalcaneal fixation using Steinmann pin 12 have been reported since then. However, use of this technique by itself is not reliable.3,5,8 We consider that one of the main reasons for the unreliability of this technique alone is inadequate fixation between the tibia and talus. However, by combining this technique with application of a locking compression plate through a single incision, adequate anterior contact and rigid fixation is achieved throughout the ankle joint, which are major factors for complete union. Although traditional procedures for arthrodesis without an anterior sliding bone graft have resulted in favorable fusion rates for cases without a large amount of bone loss, these procedures can not bring about sufficient contact area between the tibia and talus for cases with a large amount of bone loss after debridement. Our indications for this procedure include end-stage degeneration and rheumatoid arthritis with severe ankle deformity and avascular necrosis of the talus with preserved posterior talocalcaneal joint with a large amount of bone loss after debridement. Avascular necrosis of the talus is a risk factor for nonunion, however a high fusion rate can be expected with application of our technique.