
Abstract
Background: Arch supports commonly used to alleviate foot pain can impede the normal drop of medial longitudinal arch (MLA) thereby altering its function. The purpose of the study was to examine the effect of using arch supports on vertical ground reaction force (GRF) and center of pressure (COP) during simulated midstance while the foot was statically loaded. Materials and Method: Ten healthy young subjects were recruited. Two dimensional (2D) analysis of the MLA was captured for both barefoot (BF) and arch support conditions before and after loading via a custom made weight loading apparatus. The foot was loaded and positioned to simulate the midstance phase of walking. Two-dimensional reflective markers demarcated the MLA and captured with the loaded foot on a force platform. The impeded MLA drop was compared between the unloaded BF, loaded BF and loaded arch support conditions. The vertical GRF, the anterior-posterior and the medial-lateral COP displacements were also measured in response to the impeded MLA by the arch supports. Results: The arch supports impeded the MLA drop (p < 0.05) and shifted the COP toward the medial side (p < 0.05), specifically for the rearfoot (calcaneal segment region), but no changes were determined for the vertical GRF (p > 0.05). Conclusion: The impedance of MLA drop by the arch support altered the pattern of the ML COP shift in the rearfoot region. Clinical Relevance: The use of arch supports may not relieve painful foot conditions that are associated with excessive calcaneal eversion indicated by altering COP shifts in localized foot regions.
INTRODUCTION
The medial longitudinal arch (MLA) of the human foot has important mechanical functions-absorbing shock, forming a rigid lever for push off, and adapting to uneven terrains during locomotion. 17,30–32 Many studies have used the static changes of the MLA height (navicular drop) between weightbearing and nonweightbearing conditions as an important variable for predicting dynamic foot arch changes during walking 4,5,33 and as the best anthropometric parameter to characterize the MLA. 32 The arch height changes in gait have also been used to evaluate foot mechanics in terms of tibial rotation, 26 calcaneal eversion (pronation) of the foot-ankle complex 16 and in relation to the ground reaction force changes. 21
The changes of the MLA height are the result of an unbalanced vertical ground reaction force exerted on the multiple bony structures of the foot during locomotion. When the foot initially contacts the ground, the body of the talus in conjunction with the distal end of tibia bears the downward body weight; meanwhile, an upward ground reaction force exerted on the border of the foot is not aligned with this downward force on the talus. 17 This misbalance in force alignment drives the talus to rotate medially. The medial movement of the talus causes the head of the talus to be displaced anteriorly, medially, and inferiorly in a plantarflexed motion during the weightbearing condition. 17 While the talus is in plantarflexion, it depresses the navicular to the ground, and the height of the MLA decreases. The decrease of the MLA height has been shown to be coupled with calcaneal eversion. In an in vitro study, Kitaoka et al. 16 showed that the height changes of the normal arch loaded with three incremental physiologic loads were positively correlated with increased calcaneal eversion. In addition, a lowered arch height in vivo has also been found to be correlated with calcaneal eversion between early to mid-stance, 12 and with internal leg rotation during locomotion. 24,24
This coupling relationship between the MLA height and calcaneal eversion can be disrupted by arch support. For example, if the MLA is prevented from dropping, excessive calcaneal eversion or rearfoot pronation can result. In this paper, arch support has been used as a general term for medial arch supports, arch cookie, shoe inserts, and custom-molded foot orthoses. In the in vitro studies by Kitaoka and colleagues, 14,14 increased calcaneal eversion was shown for a foot loaded with 150 lb and supported by a rigid arch support. An increased peak calcaneal eversion has also been reported while running with shoes with built-in arch support. 6,6 Running with medial arch support inside shoes was found to result in greater calcaneal eversion. 25,25 Excessive calcaneal eversion has been clinically linked to a higher risk of foot injuries such as tibial stress syndrome, patellofemoral pain syndrome and posterior tibialis tendinitis. 2,10,11 The foot supports/inserts attached with arch filler were found to alter the medial/lateral ground reaction force and center of pressure shift during the early stance of walking, 22 but not the vertical ground reaction force. 13,22,36
Thus, the purpose of this study was to examine the effect of an impeded medial longitudinal arch height on vertical ground reaction forces and center of pressure displacements in anterior-posterior/medial-lateral directions when a foot was statically loaded with weights and placed in positions simulating midstance of walking from a plantarflexed towards a dorsiflexed position. We hypothesized that impedance in the medial longitudinal arch drop would result in altered vertical ground reaction force, and altered center of pressure displacements.
MATERIALS AND METHOD
Subjects and experimental setting
A total of ten healthy subjects (seven males & three females) participated in the study (age: 24.0 ± 4.7 yrs, body height: 177.3 ± 8.5 cm, body mass: 77.3 ± 11.7 kg). All subjects were recruited and screened to rule out any foot pathologies. Subjects signed written informed consents and agreed to participate in the experimental protocol, which was approved by the Institutional Review Board of the University of Oregon.
Prior to data collection, each subject was asked to stand with his/her left foot on a force plate where a foot tracing paper was taped. With the subject standing, two parallel longitudinal lines were drawn on the sides of the foot to create a foot tracking path for guiding foot position changes. Within this path, a central line was drawn along the longitudinal foot axis and was used to visually align with the foot axis when the foot was positioned within the path (Figure 1A). The longitudinal foot axis was marked on the dorsal surface of the foot between the second and third metatarsals and a calcaneal vertical line bisecting the posteromedial and posterolateral aspects of the calcaneus. These lines were important to align the foot with respect to the anteroposterior axis of the force plate (Figure 1B). Ten reflective markers for two-dimensional (2D) motion analysis were attached to the bony landmarks of the left foot on its medial side, and eight markers were used to represent the medial longitudinal arch of the foot (Figure 1C). The acceptable accuracy and reproducibility of using skin markers were previously reported in 2D and 3D foot motion analysis. 29,29
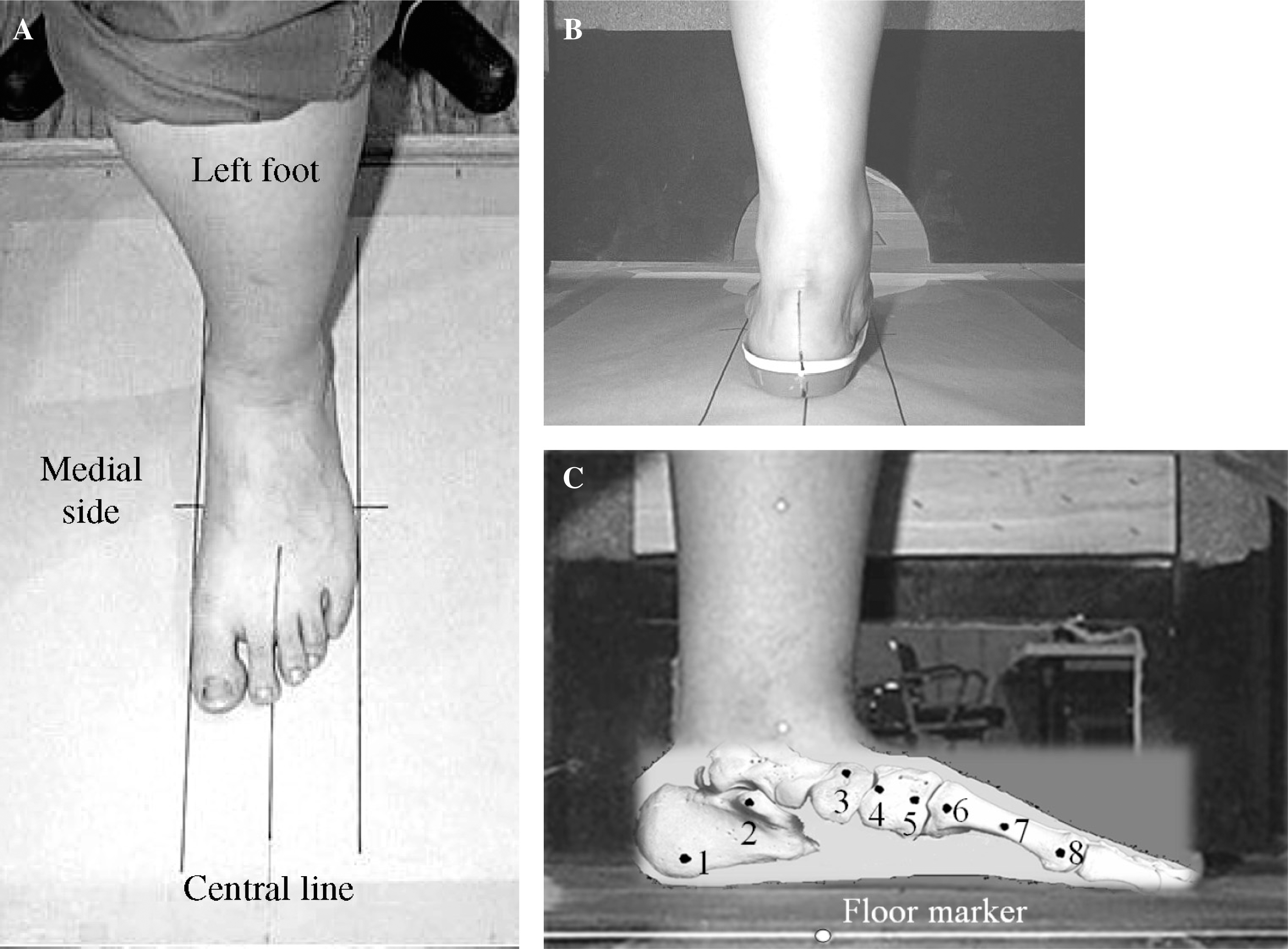
Foot positioning track and marker placements: front view (A) and rear view (B). Two longitudinal parallel lines (track) were drawn with the left foot width as reference. A central line was also drawn to visually align with the longitudinal foot axis and the posterior vertical line of the calcaneus when the foot was positioned within the track. The central line represented the anterior-posterior (y) axis of the force plate.
Reflective markers were also placed on the medial malleolus of the ankle and on the medial side of tibia about one third from its distal end for creating the tibial segment for kinematic calculations. A third reflective marker was fixed to the edge of the force plate at its central point (floor marker; Figure 1C) and was used as a reference for positioning the foot.
To test the MLA responses to the arch support, a 2D analysis of the MLA was conducted with the subjects seated in two conditions: barefoot and arch support. The arch support used in the study was a commercial product (Sorbothane II, Spectrum Sports Inc., USA). The subject was seated on a chair, and the left foot was placed on an AMTI force plate which sampled data at 1000 Hz. The foot was loaded with a physiological weight (160lb/713N) via a customized weight loading apparatus which consisted of a Weight Support Enclosure and a sliding weight loading platform (Figure 2A). The physiological weight of 160 lb was comparable to the load tested in the studies by Kitaoka and colleagues. 15 The chair height was adjusted for the subject to sit comfortably, and the upper trunk and thigh were strapped to the chair to avoid extraneous movement during testing (Figure 2B). Eight resting foot positions were determined between a plantarflexed and a dosiflexed position of the foot by sequentially aligning the eight MLA foot markers (1 to 8 numbered from rearfoot to forefoot segments, Figure 1C) with the fixed floor marker (Figure 2C). These foot placements were meant to simulate the loaded foot during the stance period of walking. For each position, the subject's foot was manually placed along the foot tracking path, and its longitudinal axis was aligned with the central line. After the alignments for each foot position, the 160 lb weight was directly loaded onto a sliding weight loading platform which had a foamed concave contact surface (10 cm in width) to fit snugly onto the distal end of the thigh of each subject. This design of loading the knee in a seated position was comparable to the leverage device used in the Basmajian and Stecko study. 1
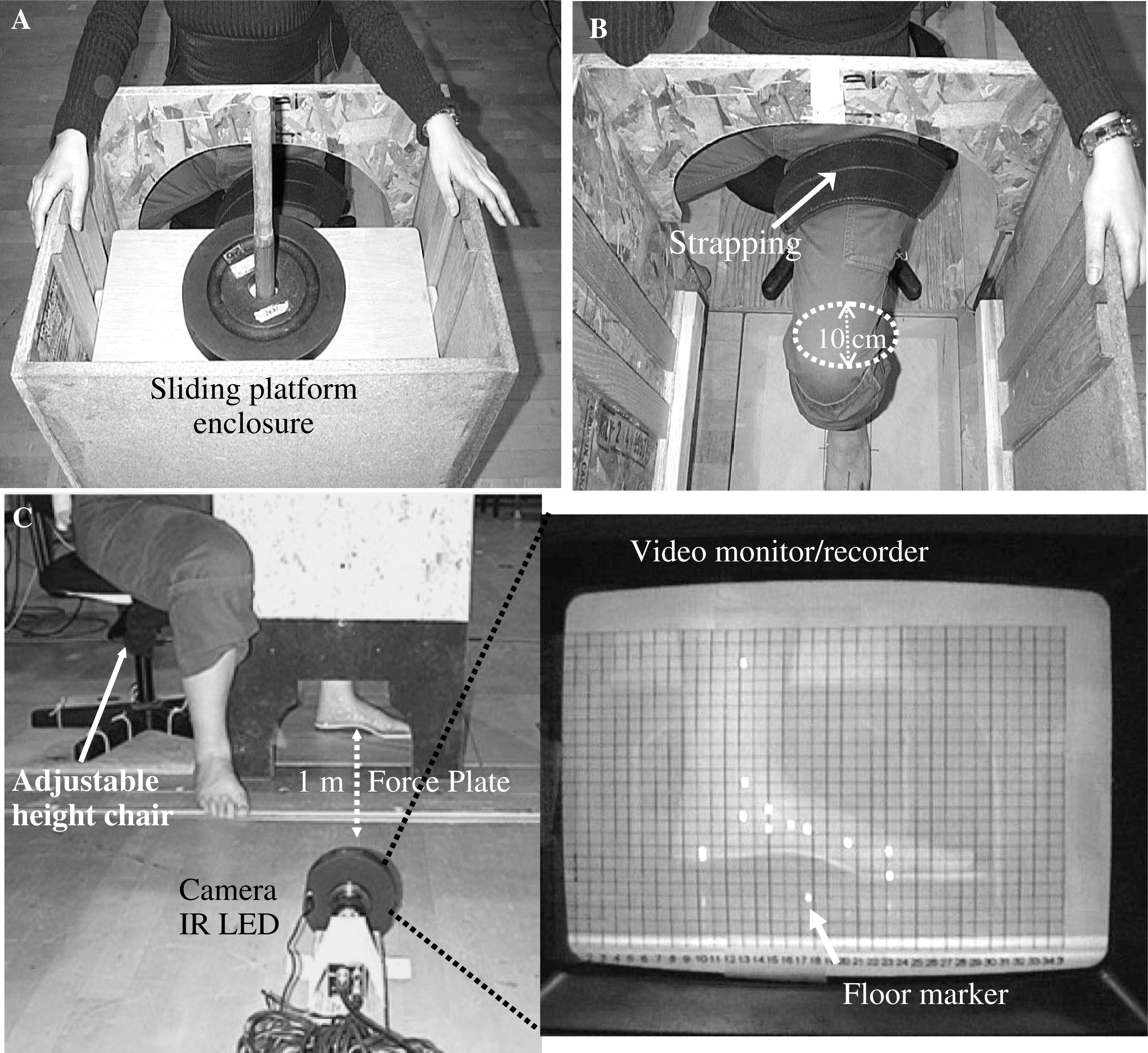
Markers of the lower limb were captured with a 30 Hz NEC video camera (NEC Corp. Japan) attached with an IR LED. The camera captured the marker positions through a side window on the weight support enclosure. The camera was placed on level ground one meter away from the foot. The marker images of the foot were transmitted to a portable video recorder and a monitor screen for viewing the side view of each foot alignment. The foot alignment between each MLA marker and the floor marker was guided by a grid transparency attached to the monitor screen (Figure 2C). Each static loaded foot position for the two testing conditions (barefoot and arch support) was recorded for three seconds. Vertical ground reaction force for each loaded foot position was acquired during each foot testing condition using the Ariel Performance Analysis Software (APAS, San Diego, CA). Prior to collecting the GRFs, the force plate was initially zeroed while the flexed left limb was rested on the plate during the immobilized seated position. After the plate was zeroed, the weight loading platform was slid down to contact with the distal end of the thigh. Six 25 lb weights added to the 10 lb sliding platform were used to provide the 160 lb (713N) load during the barefoot and arch support testing conditions. The positive x-axis was in the medial-lateral direction pointing away from the center of the plate towards the lateral aspect of the left foot, the positive y-axis was in the anterior-posterior direction pointing away from the center of the plate towards the forefoot, and a positive z-axis was in the vertical direction pointing downward from the center of the plate. A 2D reference calibration frame (5 cm ×5 cm) was filmed to provide a 1 mm precision for digitization.
In order to determine the amount of impedance in arch height drop due to the loaded MLA being supported by the arch support, all subjects also underwent a barefoot unloaded condition while being seated, with the axis of the tibial segment vertical to the floor.
Data processing and analysis
The foot markers at each foot position were digitized using the HU-M-AN software version 3.0 2D (HMA technology Inc., Canada). After the digitization, the x/y coordinates of the MLA markers were determined and exported to the Microsoft Excel program. Then, the MLA height and length were calculated for each subject in each condition. The MLA height was the measured distance between the marker attached to the dorsal side of the navicular and the floor marker, and the MLA length, between the markers attached to the medial calcaneal tubercle and the first metatarsal head. The 3-mm thickness of the arch support was subtracted from the MLA height measured in order to get the true effect of the load on the change in MLA height. To detect the impedance of the MLA height when using the arch support, the changes in the MLA height were compared among the three foot conditions across the subjects: 1) barefoot unloaded versus barefoot loaded, 2) barefoot unloaded versus arch support loaded and 3) barefoot loaded versus arch support loaded. A one-way within-subjects ANOVA with a simple planned contrast was performed to detect the MLA height impedance as a result of the use of the foot support at the foot position 2, with the tibial segment vertical to the floor.
When the foot was statically loaded with weights in each foot position, the vertical ground reaction forces were collected and averaged across the subjects for each condition. The center of pressure changes in both anterior-posterior and medial-lateral directions were calculated with respect to the center of the force plate in the x and y directions, respectively. To position the foot in each of the eight foot positions, each marker on the MLA beginning from the calcaneus was sequentially used to align with the center of the force plate. The anterior-posterior center of pressure displacement with respect to the center of the force plate in each foot position was further calculated in relation to the calcaneal marker by adding the anterior-posterior center of pressure displacement and the horizontal distance between the MLA aligned marker and the calcaneal marker. Then, the calculated anterior-posterior center of pressure displacement was normalized to each subject's MLA length as the percentage (%) center of pressure shift in the anterior-posterior away from the calcaneal marker for each foot position. The normalized % anterior-posterior center of pressure displacements thus obtained were averaged across the subjects. Simple planned contrast comparisons with two-way within-subjects ANOVA were conducted to detect the effects of the MLA impedance and foot position (P1 to P8) on the changes of the anterior-posterior and medial-lateral center of pressure displacements and the vertical ground reaction forces between the barefoot and arch support conditions.
SPSS Base 10.0 statistical software (SPSS, Inc. Chicago, IL) was used to perform the statistical analyses. The statistical significance level was set at 0.05.
RESULTS
Medial longitudinal arch height impedance
There was a significant effect of impedance of the MLA height by the arch support (F (2, 18) = 19.31, p < 0.01) among the three loaded conditions: barefoot unloaded, barefoot loaded, and arch support loaded (Figure 3). The simple planned contrast showed significant differences in the MLA height between the unloaded and loaded barefoot conditions (p < 0.05). No significant difference was detected between the unloaded barefoot and loaded arch support conditions (p > 0.05). When the MLA height was compared between the barefoot and arch support conditions, significant differences were detected (p < 0.05).
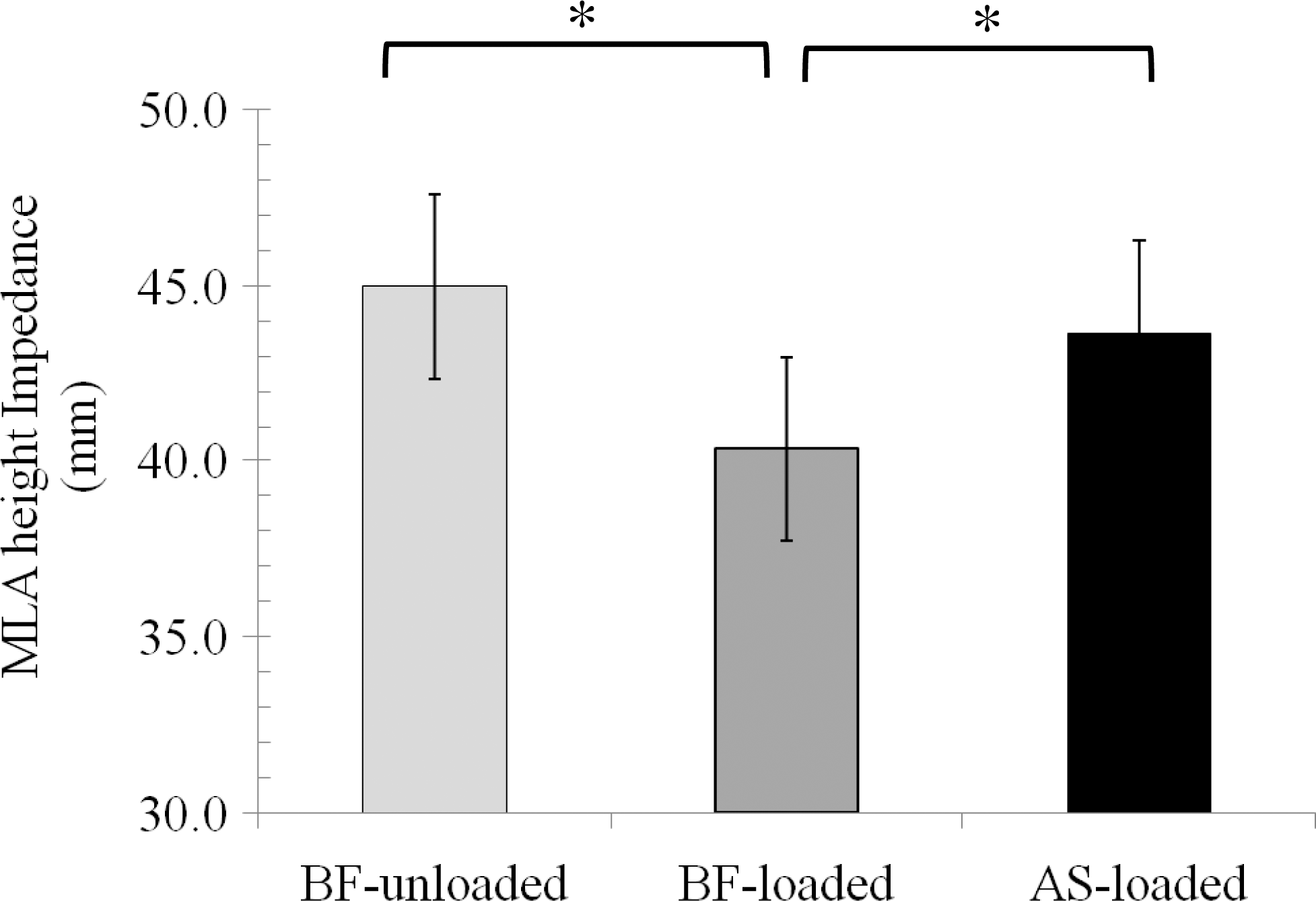
MLA height with respect to the floor marker. Means and standard errors of the mean MLA heights were compared among unloaded BareFoot (BF), loaded BF and loaded Arch Support (AS) conditions. The impeded MLA height was measured when the foot was placed at the second foot position where the loaded weights were vertically transmitted through the lower leg to the foot.
Vertical ground reaction force
There was no significant effect of the impeded MLA height on the vertical ground reaction force, i.e., no significant differences were detected between the barefoot and arch support conditions (F (1, 18) = 0.067, p > 0.80; Figure 4). The vertical ground reaction force exerted on the static loaded foot showed a gradual decline from the p1 to p8 positions of the foot as it acquired a more dorsiflexed position. There was a significant effect of foot position on the vertical ground reaction force (F (7, 56) = 8.832, p < 0.01). The simple planned contrast tests showed significant vertical ground reaction force differences between foot positions 1 and 7 and between 1 and 8.
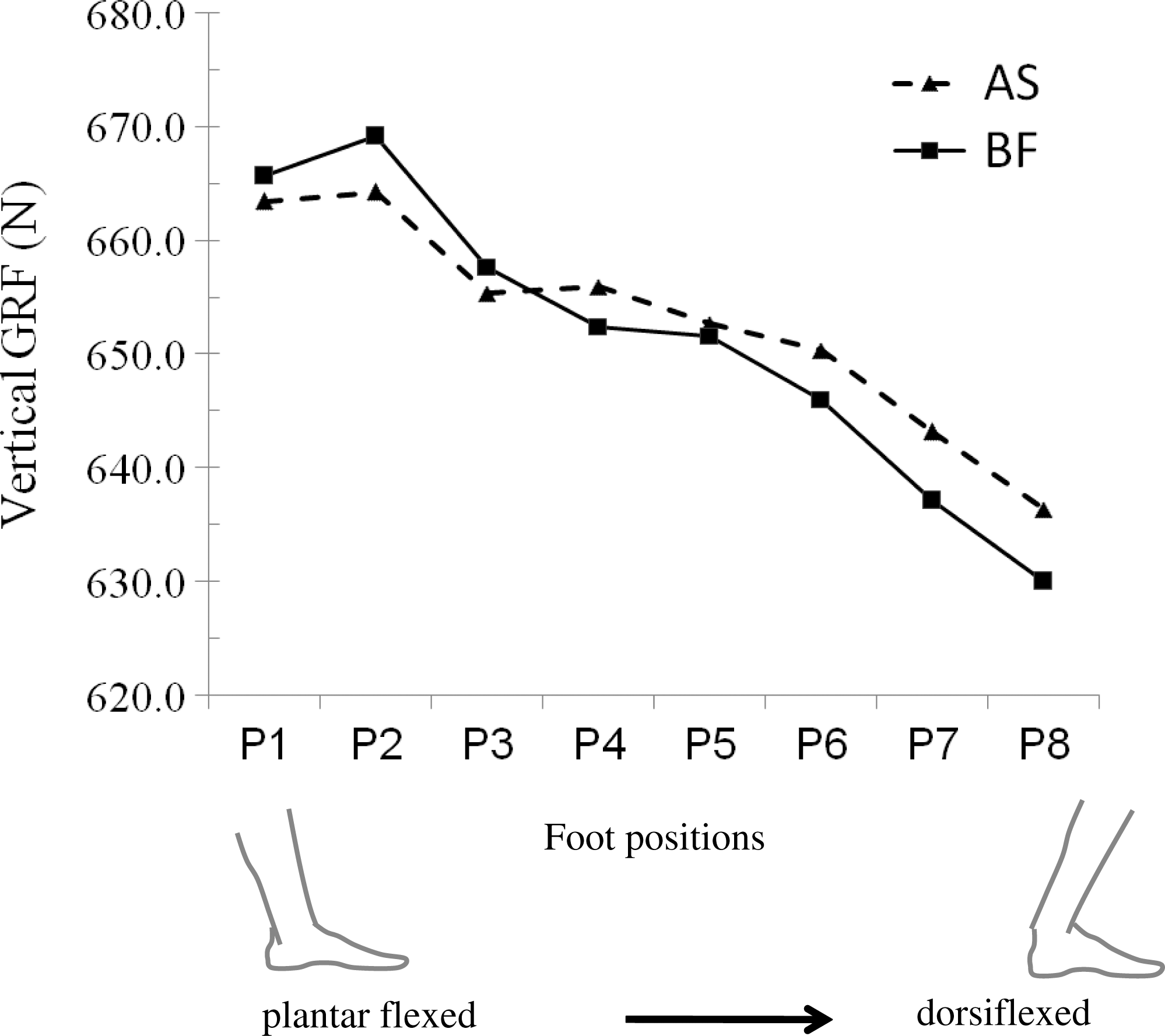
Vertical GRF (N) changes at each foot position between the BF and AS conditions. The foot was statically loaded during each foot position moving from a plantarflexed to dorsiflexed position. The second foot position (P2) was the position where the tibia was perpendicular to the foot segment, and the loading weights were transmitted vertically through the lower leg to the foot.
Center of pressure displacement in medial-lateral direction
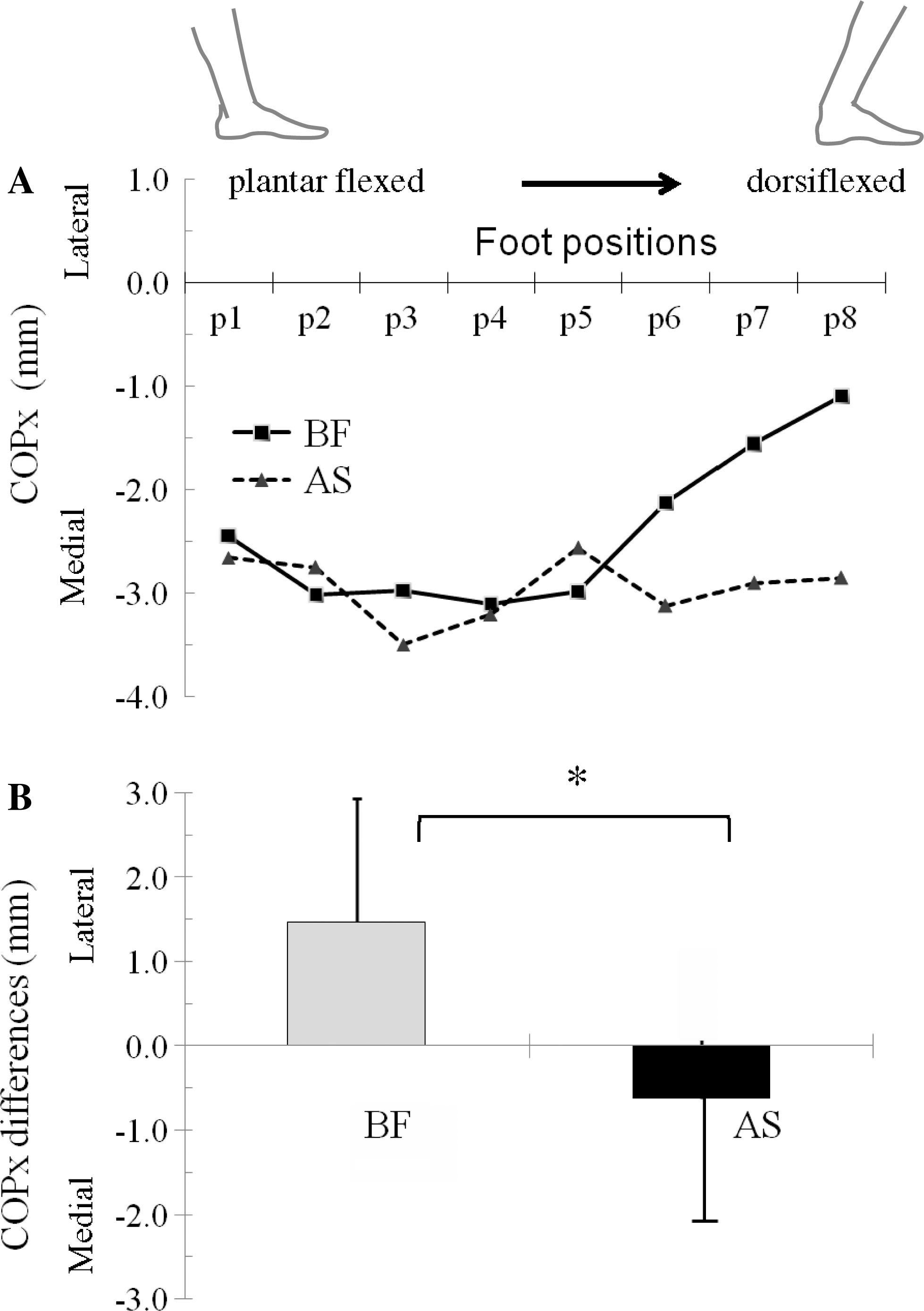
The medial-lateral center of pressure displacement (COPx) was plotted showing a medial shift away from the anterior-posterior foot axis for both barefoot and arch support conditions when the foot was positioned from the plantarflexed (p1) to dorsiflexed (p8) positions (Figure 5A). Compared to the arch support, the medial-lateral center of pressure of the barefoot was observed to shift toward the anterior-posterior foot axis as the foot moved to a more dorsiflexed position. The COPx differences between the plantarflexed (p1) and dorsiflexed positions (p8) were significantly different for the barefoot in comparison to the arch support condition (F (1, 8) = 6.15, p < 0.05; Figure 5B).
Center of pressure displacement in anterior-posterior direction
The anterior-posterior center of pressure displacement (COPy) was plotted showing an anterior shift away from the center of the force plate for both barefoot and arch support conditions when the foot was positioned from the plantarflexed (p1) to dorsiflexed (p8) positions (Figure 6A). No significant effect of condition (barefoot and arch support) was detected for the anterior-posterior center of pressure displacement (F (1, 7) = 0.14, p > 0.05). However, a significant effect of foot position was detected (F (7, 49) = 230.4, p < 0.05). Simple planned contrasts comparing anterior-posterior center of pressure displacements for each foot position showed significant differences between the foot positions (p1 versus p2, p1 versus p3, p1 versus p4, p1 versus p5, p1 versus p6, p1 versus p7, p1 versus p8; p < 0.05).
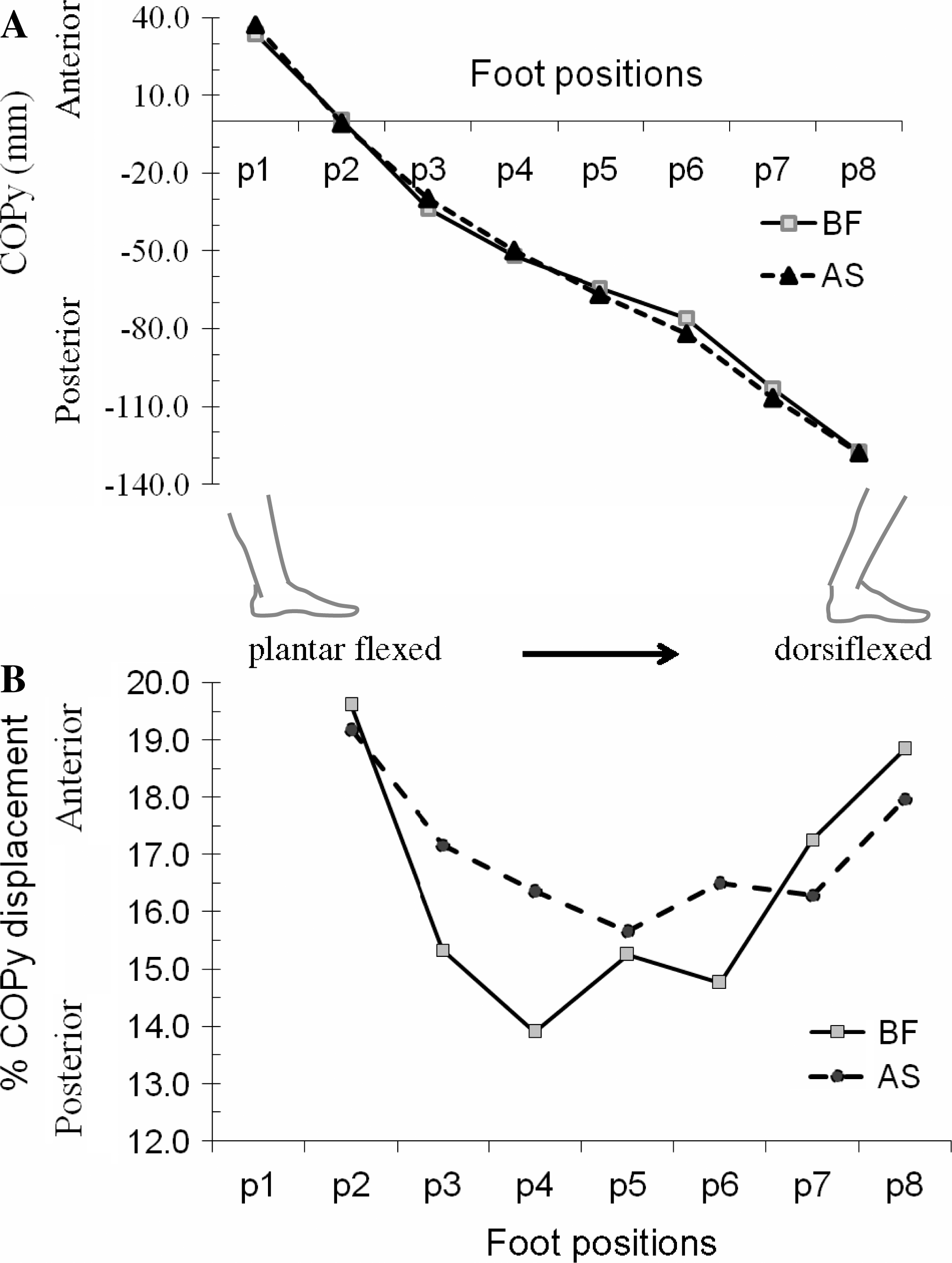
The % normalized anterior-posterior center of pressure displacements to the MLA length in both barefoot and arch support showed a consistent anterior-posterior shift moving first toward and then away from the heel of the foot (p1) when the foot was positioned sequentially from a neutral (p2) to a dorsiflexed (p8) position (Figure 6B). No significant effect of condition (barefoot and arch support) was shown for % anterior-posterior center of pressure displacements, but a significant effect of position was found specifically between p1 versus p2, p1 versus p3, p1 versus p4, and p1 versus p5 (p < 0.05; Figure 6B).
DISCUSSION
In this study, the effects of impeding the drop of the MLA of the foot by using an arch support on the vertical ground reaction force and center of pressure displacements were studied during static loading. The results showed that the arch support impeded the MLA drop and altered the center of pressure displacement in the medial-lateral direction during static loading; however, it had no effect on the vertical ground reaction force.
The arch support impeding the MLA drop with the weights directly loaded on the tibia perpendicular to the resting foot (the position 2) were comparable to the effects of the arch support on the MLA height found in other studies. 14,14 In these studies, the three-dimensional (3D) joint rotations between the calcaneus, talus, navicular and first metatarsal bones of the cadaveric feet were measured using 3D magnetic tracking sensors when the tibia was axially loaded using different loads. When a load of 667N was applied to the static feet, the difference in the impeded MLA height between the loaded barefoot and arch support conditions was found to be approximately 4.2 mm which is comparable to the current study. However, in the studies by Kitaoka, and colleagues, 14,14 the MLA height between the unloaded barefoot and loaded arch support conditions were not compared. Thus, the effect of the arch support in impeding the MLA drop in terms of not being significantly different from the normal unloaded foot was not revealed. Therefore, in the current study, the arch support blocking the MLA height was evident by showing no significant MLA height differences between the unloaded barefoot and loaded arch support conditions.
The lack of significant differences in the vertical ground reaction force between the arch support and the barefoot conditions was expected since the arch support was not likely to cause a significant change in the orientation of the force vector which resulted from the weight loading through the tibia on the foot. Therefore, the same amount of the external weight loaded on the foot for each condition produced similar vertical GRFs. The vertical ground reaction force unaltered by the arch support has been demonstrated in other studies with arch support during walking 9,13,22 and running. 36 In terms of significant differences between the different foot positions, the change in the tibial segment orientation caused a change in the orientation of the force vector which affected the vertical ground reaction force component.
When the MLA drop of the left foot was blocked by the arch support during the simulated midstance, the medial-lateral center of pressure displacement (COPx) was shifted in the medial direction more than that of the barefoot condition. The altered medial-lateral center of pressure displacement reveals that the location of the vertical ground reaction force exerted on the foot was shifted toward the medial side of the foot during the simulated midstance. Similar findings have been reported in running with medial inserts in shoes. 23 The medial shift of the center of pressure displacement could be explained by the arch support causing an alteration in the orientation of the midfoot in relation to the rearfoot. In the studies by Kitaoka and his colleagues, 14,14 a significantly increased calcaneal eversion relative to the talus was detected in cadaver studies when a rigid arch support impeded the MLA drop in comparison to no arch support condition. Increased calcaneal eversion was also reported in a study where the effect of arch support on running was investigated. 7,20,25 A positive relationship between the peak calcaneal eversion and MLA drop has been shown during midstance phase of walking. 3 Indeed, increased calcaneal eversion has led to the belief that it increases the risk of foot injuries, and therefore research has been conducted investigating the effect of customized arch support that reduces calcaneal eversion during walking 8,37 and running. 18,18
The center of pressure displacement in the anterior-posterior direction (COPy) was not altered by the arch support. The unaltered anterior-posterior center of pressure displacement indicates that the location of the vertical ground reaction force exerted along the longitudinal foot axis was not affected by the restricted MLA drop in the arch support condition. Although the center of pressure shift in the anterior-posterior direction was not affected by arch support, the fact that the center of pressure shift in the medial-lateral direction was significantly affected, can be explained by the greater contact between the arch support and the plantar surface of the MLA in the anterior-posterior direction, but not in the medial-lateral direction. This may have affected the load distribution in the two directions. The change in COPy with respect to foot position was significant; however, the interaction (condition and position) was not, which was expected because in both conditions, the same load was exerted on the foot through the tibia in both conditions.
The % normalized anterior-posterior center of pressure displacement with respect to the calcaneal marker also showed no changes with respect to condition. In both conditions, the % center of pressure shifted first toward and then away from the heel of the foot (p1) when the foot was positioned sequentially from a neutral (p2) to a dorsiflexed (p8) position. These changes with respect to position were significant, and they reflect the motion of the tibia on the articulation surface of the talus producing characteristic weight-bearing patterns. 28
A limitation of the study was that a sequence of static loaded foot positions does not simulate the true dynamics of the loaded MLA in response to the arch support. However, it is known that biomechanical measures like ground reaction forces are difficult to discern for isolated anatomical entities like the ankle-foot complex during locomotion. 34 Therefore, an experimental paradigm was required in which the results would not be confounded by other limb segments and also not be influenced by muscle contraction. To our knowledge, this was the first time such a paradigm was used in vivo to isolate biomechanical changes in the foot-ankle segment.
CONCLUSION
The arch support was studied during a simulated midstance of walking. With static loading, a shift in the medial-lateral center of pressure was shown in the rearfoot which can be related to findings of calcaneal eversion in other studies with arch supports. This finding has significant clinical importance because the use of arch support may not relieve painful foot conditions that are associated with excessive calcaneal eversion indicated by altering COP shifts in localized foot regions. Future directions of this study may isolate such biomechanical changes during normal walking with an arch support and investigate different measures to reduce the risk of foot injuries due to an arch support.