
Abstract
Background:
We hypothesized that using a cadaveric Lisfranc ligamentous injury model, abduction stress would provoke greater post-injury motion than axial weightbearing between the medial cuneiform (MC1) and the base of the second metatarsal (MT2). Second, we hypothesized that both a tensioned suture-button device and a rigid screw fixation method could maintain a reduction and similarly restrain motion to intact (pre-injury) levels.
Materials and Methods:
Motion was measured between MC1 and MT2 in five matched pairs of human cadaveric feet. Specimens were tested prior to injury, following a transverse ligamentous Lisfranc injury, and then randomized to either screw or tensioned suture-button fixation. Axial then abduction loads were applied. Measurements were repeated after one thousand loading cycles.
Results:
With both axial and abduction loads, statistically significant differences in motion were detected between the intact and post-injury conditions, although the magnitudes were greater with abduction (6.8 mm versus 2.0 mm, p = 0.000004). With abduction loads, both fixation methods were effective in restraining motion to pre-injury levels (screw fixation: 1.5 mm intact versus 1.1 mm post-fixation, p = 0.487; suture-button fixation: 1.3 mm intact versus 2.1 mm post-fixation, p = 0.063), and similarly, both devices restrained motion to less than post-injury levels (screw fixation: 8.1 mm post-injury versus 1.1 mm post-fixation, p = 0.001; suture-button fixation: mean 5.5 mm post-injury versus 2.1 mm post-fixation, p = 0.0002). No significant differences in these patterns were detected following cyclic loading.
Conclusion:
Small, though statistically significant, amounts of motion are produced between MC1 and MT2 with axial loading after a ligamentous Lisfranc injury. With abduction stress, we were able to show a significantly greater difference between pre- and post-injury motion and the ability of both fixation methods to restrain motion to pre-injury levels.
Clinical Relevance:
Abduction stress may be valuable when diagnosing and testing the transverse ligamentous Lisfranc injury. Both suture-button and screw fixation methods restrain motion at the Lisfranc complex.
INTRODUCTION
Consistent successful outcome after midfoot injuries continues to elude treating surgeons. Even subtle injuries of the Lisfranc complex may lead to significant morbidity. 7 Treatment options vary, ranging from a nonweightbearing cast in selected cases, to open reduction and internal fixation (ORIF) and even primary arthrodesis. 7 All have a common goal of restoring and maintaining an anatomic reduction. 23
The ligamentous Lisfranc disruption has been shown to be a unique injury requiring particular attention with respect to treatment. 18 Arthrodesis has been one proposed treatment of these injuries. 20 Until recently, arthrodesis has been thought of as a salvage procedure for the Lisfranc injury. 22 With screw fixation, cyclic loading across joints may lead to fatigue failure of metallic implants. As a result, hardware is often removed from joints fixed with rigid fixation and this can be associated with impaired patient outcomes. 6 The placement and subsequent removal of transarticular screws yields increased articular cartilage destruction and this articular trauma may lead to higher rates of degeneration. 1 Given the problems associated with current treatment techniques and outcomes, it is reasonable to consider alternative forms of fixation. Such alternatives are perhaps best applied to the purely ligamentous Lisfranc injury as it is a unique subset of the Lisfranc injuries with the opportunity to maintain normal joint function if anatomic stabilization can be achieved.
Flexible fixation, as opposed to either rigid internal screw fixation or primary arthrodesis, is a fixation technique with little data to support its use in the ligamentous Lisfranc injury. Normal motion at the Lisfranc complex has been characterized, and although it is a small amount, it does exist. 25 The attributes of early controlled motion in ligamentous healing is meaningful and studies have assessed ligament healing in the rat knee model, for example, which indicate that ligamentous tissue heals with better organization and strength when joints are stabilized but not rigidly immobilized. 13,24,30,32 Similar reasoning has been applied to flexible fixation techniques at the ankle syndesmosis, and in other areas of trauma related fixation such as in intramedullary nailing. 3 –5,10,16,17,21 There has been a paradigm shift in the understanding and teaching of fracture fixation with some advocacy of relative stability contrasted with absolute stability in appropriate settings. 27 Regardless of the stabilizing device used, biological healing must occur prior to the implant, be it rigid or flexible, failing.
A tensioned suture-button device is a form of flexible fixation, which has shown some favorable results and few failures when applied to ankle syndesmosis injuries. 28,29 Only one biomechanical study has been published comparing a tensioned suture-button device for use at the Lisfranc joint with screws. 26 This cadaveric study utilized only axial loads, showed small median displacements, and did not utilize cyclic loading to test the construct.
The purpose of this study was to investigate a tensioned suture-button device as a form of internal fixation in a ligamentous Lisfranc injury model as an alternative to traditional rigid screw stabilization. We hypothesized that using a cadaveric Lisfranc ligamentous injury model, abduction stress would provoke greater post-injury motion than axial weightbearing between the medial cuneiform (MC1) and the base of the second metatarsal (MT2). Second, we hypothesized that both a tensioned suture-button device and a rigid screw fixation method could maintain a reduction and similarly restrain motion to pre-injury levels.
METHODS AND MATERIALS
IRB approval for this study was obtained under a cadaveric study IRB approval and deemed exempt as per HHS regulation 45 CFR 46.101(b). Five matched fresh frozen pairs (total of ten specimens) of human cadaveric transtibial specimens were utilized in a biomechanical study including three male donors (ages 55, 57, and 59) and two female donors (ages 56 and 57). The specimens consisted of the entire foot and ankle complex, transected at the tibial diaphysis. Specimens had been frozen at −40°C, and were completely thawed 24 hours prior to testing. Bone mineral densities of the distal tibia using previously established protocols were obtained by Dual Energy X-Ray Absorptiometry (DEXA)imaging (GE Lunar Prodigy™, Model 8743, GE Healthcare, Waukesha, WI) to ensure likeness of interspecimen and intraspecimen bone quality, with the intent to eliminate any specimen that was of poor quality that could otherwise add confounding variables related to the specimen rather than the fixation device being tested. 31 Fluoroscopic imaging was also utilized to check for and exclude specimens with pre-existing pathology of the foot or ankle. No specimens revealed any pre-existing pathology on visual inspection or fluoroscopic evaluation. The measured bone mineral density of each specimen yielded acceptable results with DEXA scanning, and thus no specimens were excluded from the study.
Axial Load Displacements
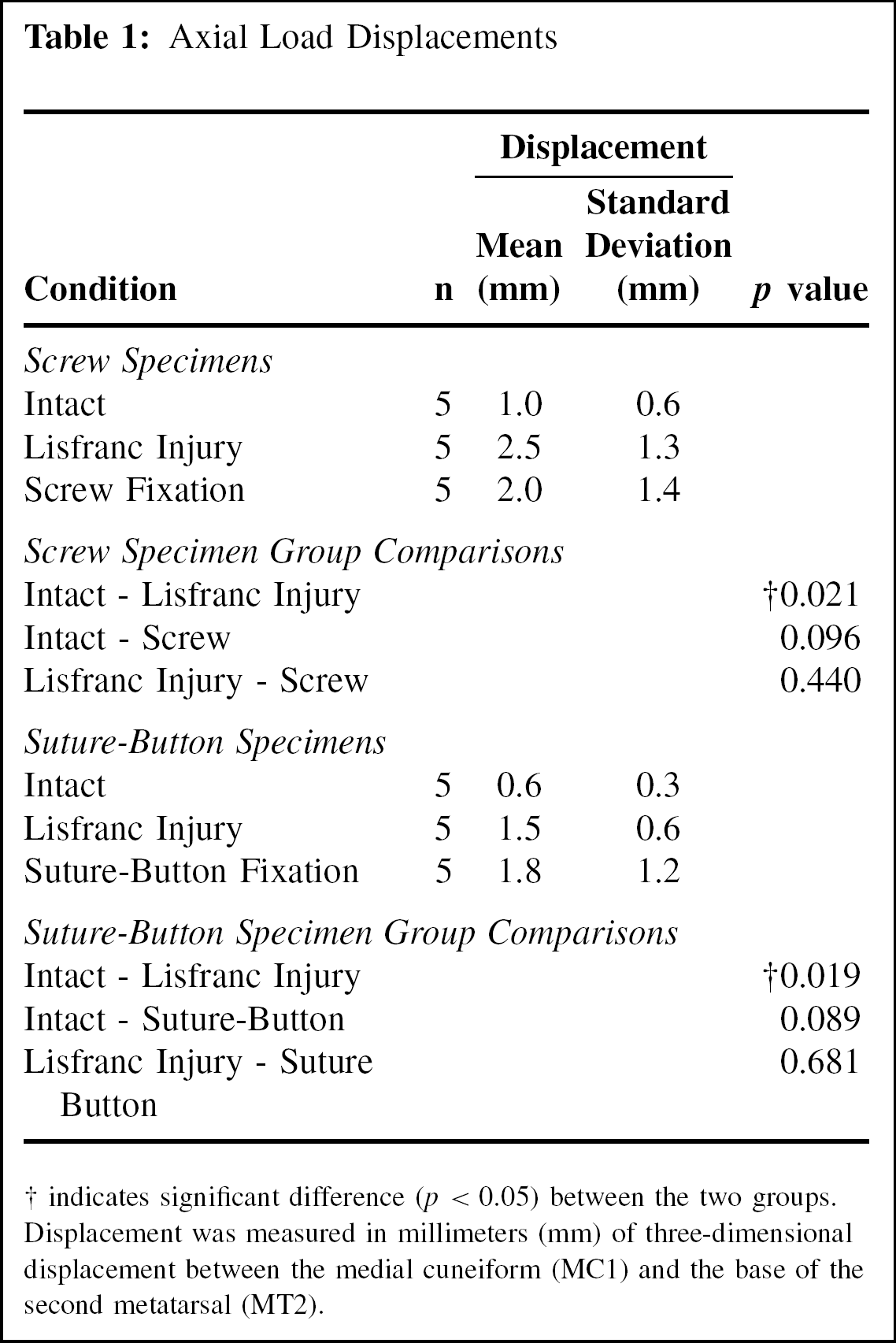
indicates significant difference (p < 0.05) between the two groups. Displacement was measured in millimeters (mm) of three-dimensional displacement between the medial cuneiform (MC1) and the base of the second metatarsal (MT2).
Experimental setup
Specimens were mounted in a multipoint contact vise that was designed for placement in a servohydraulic materials testing machine (Instron® model 8500, Norwood, MA). Careful dissection of the specimens was performed uniformly wherein the overlying dorsal subcutaneous tissues at the first and second tarsometatarsal and first and second intercuneiform joints were removed, while preserving the capsular attachments. 15 Care was taken to preserve the interosseous and plantar ligaments, including the plantar fascia and long plantar ligaments, thereby preserving the natural tie-rod mechanism. 15 To produce the point of maximal strain on the Lisfranc complex, as would occur in the repaired patient if allowed to bear weight, the tibiotalar joint was fixed at 30 degrees of plantarflexion with three out-of-plane threaded Steinman pins. 1,6 Additionally, to simulate the hindfoot rigidity that occurs during toe off in the human gait cycle, the point of maximum stress seen by the midfoot, threaded Steinman pins were also placed across the talonavicular, subtalar, and calcaneocuboid joints in a neutral position. 6 All were placed with fluoroscopic guidance and were placed from the posterior aspect of the specimen so as to minimize their interference with the testing region of the midfoot. Using fluoroscopy, the joints of the midfoot were marked with indelible ink so as to allow directed dissection and accurate placement of fixation devices during later steps.
Axial load testing was established in a manner that allowed forefoot weightbearing only through the first and second metatarsal heads by placing a metallic block beneath just the medial forefoot, positioning the hindfoot off the platform, again concentrating maximal force on the first-second tarsometarsal (TMT) complex (Figure 1). A force of 222.4 N was set as the target loading force for testing in the Instron machine, and was based on reasoning as described in previous studies testing the Lisfranc complex. 15,26
During abduction stress testing, the Instron elevated the specimen above the supporting platform allowing unimpeded abduction stress testing. A Kirschner wire was driven, dorsal to plantar, through the third metatarsal head to allow an abduction force to be applied by a lateral pull transferred through the intermetatarsal ligaments. During axial weightbearing the pin in the third metatarsal was not allowed to touch the platform. While suspended, a pneumatic actuator was attached to the Kirschner wire running through the third metatarsal head and a 50N laterally directed force was applied to produce the abduction stress (Figure 1). Pilot testing revealed that 50N provided adequate motion while still being tolerated by the specimens without causing apparent damage.
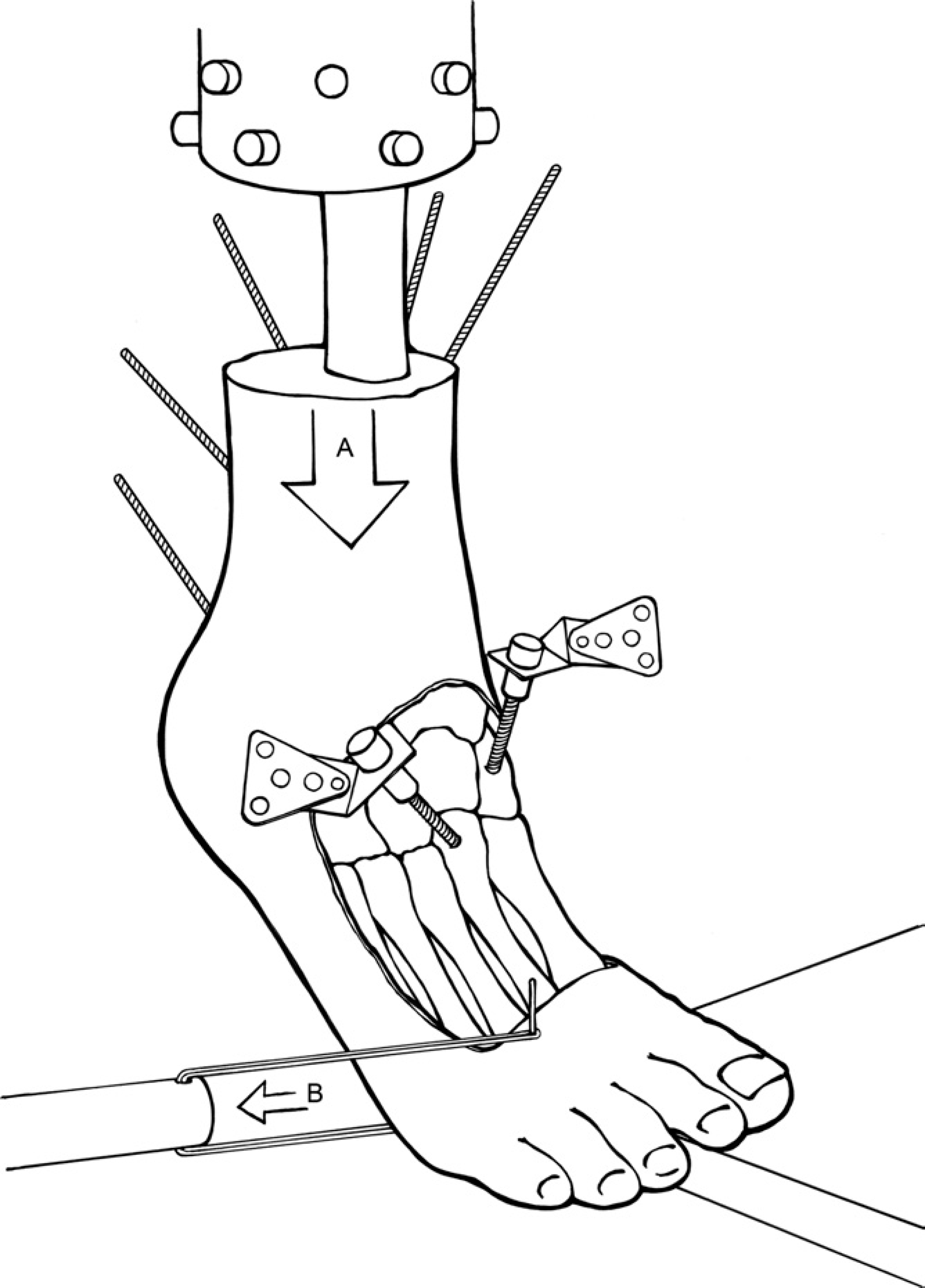
The specimen and testing construct. Fully threaded Steinman pins were driven through the ankle, subtalar, calcaneocuboid, and talonavicular joints to rigidly lock the hindfoot, with the ankle in thirty degrees of plantarflexion. Axial load (A) was applied using the Instron, with the first and second metatarsal heads mounted on the platform. During abduction testing, the foot was suspended above the platform, and an abduction load (B) was applied by pull with a pneumatic actuator through a pin driven in the third metatarsal head. Optical markers were fixed to the bones via solid screws.
An optoelectronic motion capture system (OptoTRAK Model 3020, Northern Digital Inc., Waterloo, Ontario, Canada) with a manufacturer and laboratory calibrated accuracy of 0.1 mm was utilized for recording motion. Micro-motion sensors attached to rigid screws were screwed into bone at the base of the first metatarsal, the base of the second metatarsal (MT2), the medial cuneiform (MC1) and the intermediate cuneiform in a uniformly standardized orientation in all specimens so as to prevent their later obstruction of planned fixation devices. A fifth motion marker was placed in the navicular.
Experimental testing
Based on pilot testing, we found an initial preconditioning phase of approximately 200 cycles was required to achieve consistent motion with loading. Uncycled specimens did not yield consistent motion measurements, likely due to stretching out of soft tissues of the cadaver. Accordingly, all intact mounted specimens experienced 200 cycles at 0.5 Hz, roughly half the frequency of the uninjured adult human gait, 9 from 50 N to 222.4 N. Pre-injury stress testing was performed in all specimens with initial axial weightbearing followed by abduction stress with motion data recorded and stored for analysis. For axial stress testing, simulated toe-off weightbearing was performed by cycling the Instron to 222.4 N ten times, with motion data recorded during the last two cycles. The foot was then suspended above the testing platform and the pneumatic actuator pulled 50N of force laterally ten times with motion data collected during the last two cycles.
The Lisfranc injury model was produced based on a reproducible transverse ligamentous Lisfranc injury pattern. 15 Transection of the ligamentous structures of the Lisfranc region was performed with a 15-blade scalpel. The blade was passed between the bases of the first and second metatarsals to transect the Lisfranc ligament, the plantar ligament between MC1-MT2, and the dorsal and plantar capsules of the intermediate cuneiform to MT2. The transverse injury pattern was then continued by disrupting the plantar ligaments between the medial cuneiform and the second and third metatarsal bases at the plantar aspect of the second metatarsal base and intermediate cuneiform, mimicking the model published by Kaar et al. 15 The first TMT capsule and the intercuneiform ligaments between the medial and intermediate cuneiforms were not cut. A small laminar spreader distracted obliquely between the medial cuneiform and the second metatarsal base interval to ensure complete disruption of the stabilizing ligaments. Once disrupted, the specimens were tested using the same axial weightbearing and abduction stress protocols as outlined previously, utilizing the optical motion capture system to measure motion.
Randomization of the matched pairs was performed such that one specimen was stabilized by screw fixation while the contralateral specimen received stabilization by a tensioned suture-button device.
Surgical technique for screw or suture-button fixation
In the screw fixation group, an anatomic reduction was obtained and a provisional 0.062-inch Kirschner wire was placed from the base of the second metatarsal base into the intermediate cuneiform. A pointed bone tenaculum was placed from the proximal medial aspect of the medial cuneiform to the lateral base of the second metatarsal to hold an anatomic reduction. A 2.5-mm drill bit was used to drill between the medial cuneiform and the base of the second metatarsal. A 3.5-mm fully threaded cortical screw (Synthes USA, West Chester, PA) was placed from the medial cuneiform to the base of the second metatarsal and the clamp was removed. A second 2.5-mm drill hole was placed from the base of the second metatarsal into the intermediate cuneiform followed by the second 3.5-mm cortical screw (Figure 2), and the provisional Kirschner wire was then removed. The arrangement of the screws was placed in this pattern so as to best reproduce the support lost by the “injured” stabilizing structures, and is similar to a pattern described in a previous study. 19
In the suture-button fixation group (Figure 3), an anatomic reduction was obtained and a 0.062-inch Kirschner wire was placed from the base of the second metatarsal into the intermediate cuneiform, and left for definitive fixation of this joint. The proximal medial cuneiform was clamped to the base of the second metatarsal with the use of a pointed bone tenaculum. Starting at a point near the plantar distal quadrant of bone along the medial wall of the medial cuneiform, a site found to have superior bone density properties in pilot testing, a 2.9-mm drill bit which was included in a commercially available suture-button fixation device kit (Standard Tightrope®, Arthrex, Naples, FL) was used to produce a pilot hole starting from the medial cuneiform and exiting from the base of second metatarsal. The exit point was at the junction of the proximal second metatarsal diaphyseal-metaphyseal flare laterally in all specimens. The drill bit was slowly removed while the guidewire of the Tightrope® was passed in reverse so as to have the flat button present at the subcutaneous medial aspect of the medial cuneiform and the larger, more prominent knots present at the lateral aspect of the second metatarsal, a location that in vivo would allow tucking the knot between the second and third metatarsals. Once the guidewire exited the medial aspect of the medial cuneiform, the button was flipped to lay flush along the medial cuneiform and the guidewire and its passing suture were clipped and removed. While the reduction was still secured by the bone clamp, the sutures were tightened to the point of maximal reduction and the knots were tied by the same surgeon so as to avoid variability in the technique performed.

A representative fluoroscopic image taken of the rigid screw fixation model. Also note the hindfoot fixation with large threaded Steinmann pins extending to the navicular and cuboid to simulate the hindfoot locking mechanism during toe off, as well as the Kirschner wire in the third metatarsal head, used for the application of abduction loads.
Following fixation by one of these methods, the specimens were tested with the axial and abduction stress protocols. To look for possible changes in motion restraint afforded by the fixation device following a number of cycles, specimens from both groups were axially loaded from 50 N to 222.4 N for 1000 cycles at 0.5 Hz. Motion data was collected at the first and final two cycles. Subsequently, to evaluate whether cyclic weightbearing affected the ability to maintain a reduction with loads in the abduction plane, the specimens were then suspended and abduction stress testing was performed at 50N for ten cycles, collecting motion data from the last two cycles. Fluoroscopy was used to verify placement of each fixation device in the desired location and to evaluate the accuracy and any failures of fixation.

A representative fluoroscopic image taken of the flexible suture-button fixation model.
Data from the motion detector was digitally stored on the computer. Maximum displacements were recorded and listed for each specimen as the greatest displacement vector of three-dimensional diastasis between minimum and maximum loading (50 N and 222.4 N), which in all cases was greatest in the horizontal plane, as measured between the markers at MC1 and MT2. Markers were placed in the intermediate cuneiform, first metatarsal base and navicular, and although data from these are not utilized in the measurements tested for this study, the data were collected for use in later studies. A professional laboratory engineer, familiar with the motion analysis system, performed data analysis to provide information regarding the relative motion of the structures using Microsoft Excel (Microsoft, Redmond, WA). Initial calibration was performed.
Statistical analysis
Data were tabularized and graphically plotted utilizing Microsoft Excel® (Microsoft, Redmond, WA). Comparisons were performed using a two-tailed paired t-test. Significance was set at alpha
RESULTS
Motion data during axial and abduction stress during pre-injury and post-injury conditions are displayed in Figure 4. There was a statistically significant difference in motion between the intact state and the Lisfranc injury state with axial loading (mean 0.8 mm intact versus 2.0 mm post-injury, p = 0.007). There was also a statistically significant difference in motion between the intact state and the Lisfranc injury state with abduction loading (mean 1.4 mm intact versus 6.8 mm post-injury, p = 0.00001). Notable in this comparison is a significantly greater magnitude of mean motion between MC1-MT2 with abduction loads compared with axial loads after Lisfranc injury (mean 6.8 mm post-injury with abduction load versus 2.0 mm post-injury with axial load, p = 0.000004).
With axial loads (Table 1), no significant differences in motion were detected between the intact and post-fixation conditions fixed with either screws or suture-buttons (screw fixation: mean 1.0 mm intact versus 2.0 mm post-fixation, p = 0.096; suture-button fixation: mean 0.6 mm intact versus 1.8 mm post-fixation, p = 0.089). However, even though significance was shown in the difference between pre- and post-injury motion (screw fixation group: mean 1.0 mm intact versus 2.5 mm post-injury, p = 0.021; suture-button fixation group: mean 0.6 mm intact versus 1.5 mm post-injury, p = 0.019), given the relatively small overall magnitudes of motion observed with axial loading in addition to the available sample size, we were unable to show significance in the ability of either technique to restrain motion to less than the post-injury condition when tested with axial loads (screw fixation: mean 2.5 mm post-injury versus 2.0 mm post-fixation, p = 0.440; suture-button fixation: mean 1.5 mm post-injury versus 1.8 mm post-fixation, p = 0.681). Data were recorded in the axial plane after one-thousand cycles as described, however due to changes in the position of the foot and dampening of the specimen over time, this data was not felt to be valid for interpretation (see discussion).
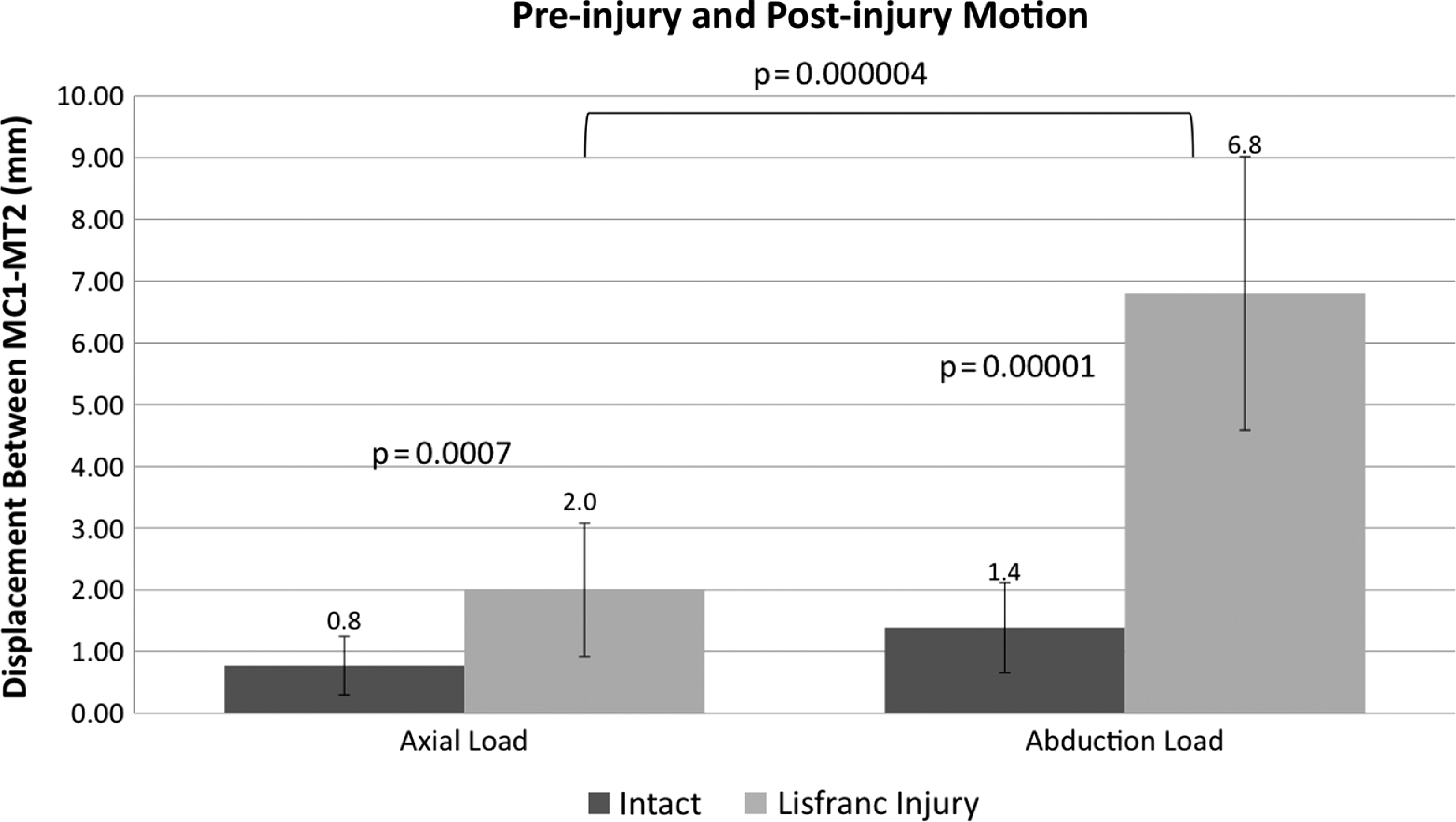
Statistically significant difference in motion between the medial cuneiform (MC1) and the base of the second metatarsal (MT2) was detected between the intact (pre-injury) and Lisfranc injury states in both axial and abduction load testing. Note the magnitude of difference in the average motion seen with axial loads (0.8 mm intact versus 2.0 mm post-injury) compared with that seen with abduction loads (1.4 mm versus 6.8 mm, respectively).
Abduction Load Displacements
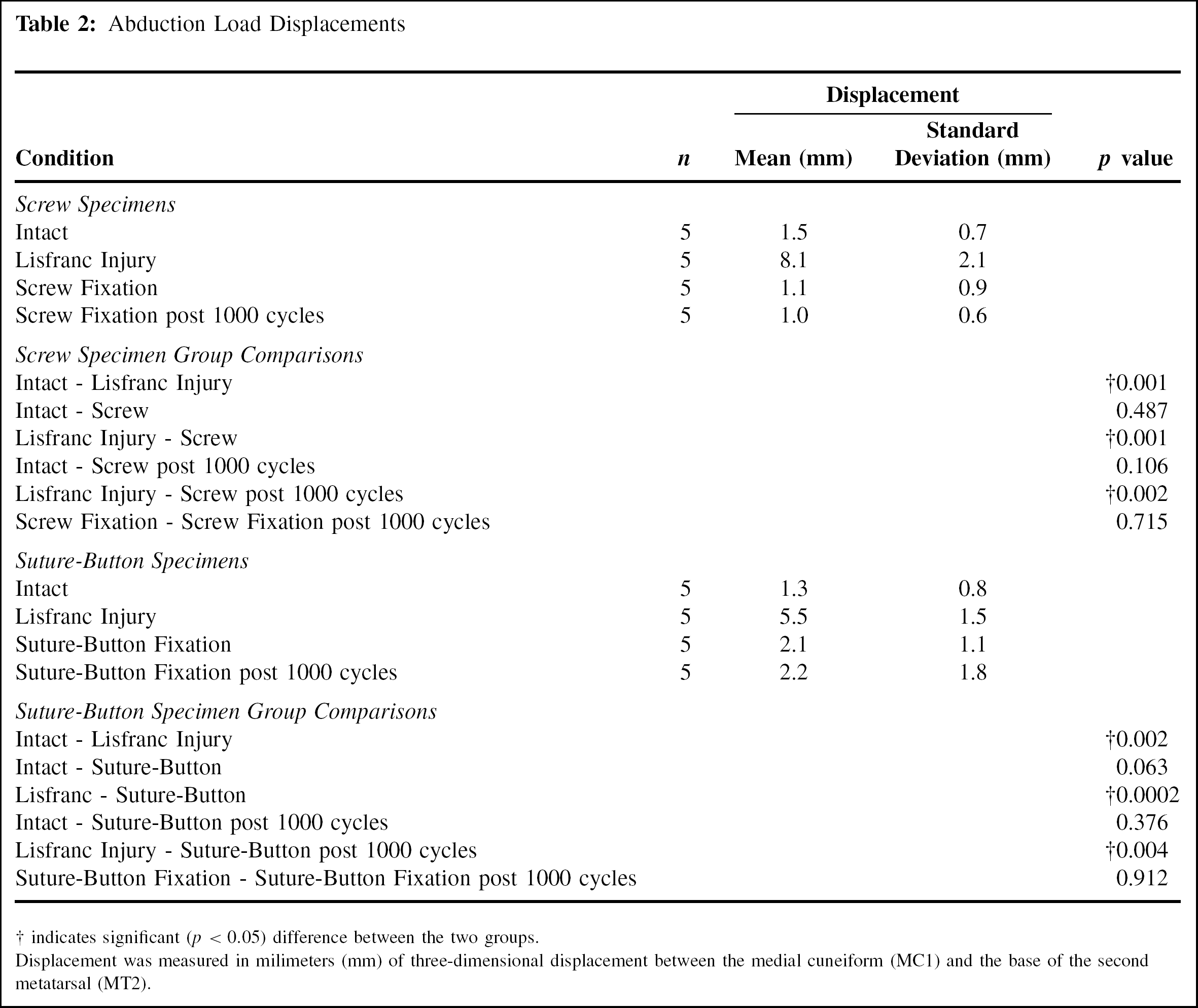
indicates significant (p < 0.05) difference between the two groups.
Displacement was measured in milimeters (mm) of three-dimensional displacement between the medial cuneiform (MCI) and the base of the second metatarsal (MT2).
With abduction stress testing (Table 2), no statistically significant difference in post-fixation motion compared to pre-injury motion was detected with either fixation technique (screw fixation: mean 1.5 mm intact versus 1.1 mm post-fixation, p =0.487; suture-button fixation: mean 1.3 mm intact versus 2.1 mm post-fixation, p = 0.063), suggesting that with abduction loads, both fixation methods were effective at restoring motion to pre-injury levels. Additionally, both fixation methods yielded significantly less motion than the post-injury condition (screw fixation: mean 8.1 mm post-injury versus 1.1 mm post-fixation, p = 0.001; suture-button fixation: mean 5.5 mm post-injury versus 2.1 mm post-fixation, p = 0.0002). Following one thousand cycles, no change in these patterns was demonstrated, suggesting that axial cyclic loading did not loosen either fixation construct.
DISCUSSION
This study is a laboratory-based biomechanical comparison of the use of a tensioned suture-button device as a means of flexible fixation with a rigid screw fixation construct for the treatment of a ligamentous Lisfranc injury model. The first aim of this study was to test the ability to produce a reproducible, purely ligmentous Lisfranc injury and test the hypothesis that abduction stress would afford a greater magnitude of displacement at the Lisfranc complex in this injury model. In both axial and abduction stress testing, we were able to show that our model afforded significantly more motion after injury than in the intact state, and thus we feel we adequately produced an injury and measurement model that simulated what may be encountered clinically. Importantly, the magnitude of motion measured with axial loads was significantly less than that seen with abduction testing (mean, 2.0 mm versus 6.8 mm, respectively). We feel that this is an important finding and one that corroborates the findings of Kaar et al., 15 who showed that with this transverse ligamentous Lisfranc pattern, radiographs accurately diagnosed the injury only one of five times (20%) with axial weightbearing loads compared to five of five times (100%) with abduction stress. With axial load, such as is produced with weightbearing, the tie-rod effect of the plantar fascia and ligaments is likely creating a compressive force at the tarsometatarsal complex, thereby eliminating some of the expected motion that could occur after loss of the Lisfranc ligament's stabilizing effect. 14,15 This reduction force at the Lisfranc complex in the purely ligamentous Lisfranc injury model with axial loads highlights the importance of testing a fixation technique for this injury with abduction loads. Additionally, in biomechanical testing, the investigator should test a “worst case scenario” wherein the maximum amount of motion possible at the area of interest is provoked, thereby allowing the greatest opportunity to detect differences in the fixation devices ability to restrain that motion. The differences in post-injury motion seen with axial loading of only 2 mm may represent a statistically significant difference, but potentially may not represent a clinically significant finding. We feel that these are reasons to support the testing of fixation devices of the Lisfranc complex using an abduction force.
The second aim of this study was to test the ability of a tensioned suture-button device to restrain motion to pre-injury levels similar to a screw fixation method with both axial and abduction loads. We were not able to test for the equivalence of the two techniques to restrain motion, but rather the ability of each technique to restrain motion to pre-injury levels. In axial stress testing we were unable to detect a difference in either the screw or suture-button techniques’ abilities to restrain motion, and neither technique reduced motion back to pre-injury levels. However, again, the magnitude of motion seen before and after injury was small when testing in axial loads, making detection of differences in motion more difficult. Additionally, the amount of motion seen in the intact and injury states and with both fixation techniques were all around or less than 2 mm. Such motion would be considered within the limits of an anatomic reduction by radiographic criteria, 7 again highlighting the fact that axial loading may not be the best method by which to test stabilization of this injury model.
Data collected after cyclic loading in the axial plane was not included in the final analysis. Following one-thousand axial loading cycles, the specimens all had significantly subsided around the stabilized midfoot and dampening of motion was observed with both the screw and suture-button fixation methods. Because of this, we were unable to comment on any changes in motion after cyclic loading with axial loads as the surrouding foot had been altered more than the area of fixation. With continued cyclic testing, we noted a visual change in the position of the foot wherein the heel subsided to attain a more plantigrade position, losing the original 30 degrees of plantarflexion position and observing a diminished relative height of the cross bar of the Instron machine at the conclusion of the cyclic testing. Some of this subsidence appeared to have occurred by attenuation of the surrounding joints and tissues, a conclusion supported by a finding of increased motion recorded at the naviculocuneiform joint over time. This may reveal a flaw in our testing model, but may also represent an inherent problem with cyclic testing in cadaveric models. A lack of biological healing and the lack of effect from muscles, tendons and a normal gait cycle produce a situation wherein cyclic testing simply investigates the material properties of the cadaveric specimens and the surrounding joints and tissues more than the area of interest or fixation technique.
In testing the ability of the tensioned suture-button device to restrain motion after ligamentous Lisfranc injury with abduction loads a few interesting points should be highlighted. Both the screw and suture-button techniques were able to restrain motion significantly after injury, and both techniques restored motion to pre-injury levels. With abduction loads, we found no difference in the amount of motion allowed by either fixation method after one-thousand cycles of axial weightbearing, and because the effect of apparatus subsidence and motion dampening, as seen with axial cyclic testing, did not translate to abduction testing conditions, we were not able to interpret this data.
The concept of “flexible-fixation” was introduced as one of the rationales behind the use of tensioned suture-button device for the treatment of a purely ligamentous injury, such as the model used in this study. Our study supports the findings of Ouzounian and Shereff, 25 showing that measurable motion does occur in the intact state at the first and second tarsometatarsal complexes. We were not able to test equivalence of the two devices, and as such, our statistical comparison of the ability of each device to restore mean post-fixation motion to levels less than the post-injury state and to the same level as the intact (pre-injury) condition in the abduction loading plane does not highlight more flexibility of the suture-button device. A closer look at the mean post-fixation motion in the abduction plane with each fixation method (mean, 1.1 mm versus 2.1 mm) in addition to the non-statistically significant difference between post-suture-button fixation and intact motion with a p value of only 0.06, suggest a non-significant trend towards more motion. With the numbers available, we were not able, however, to show statistically significant more “flexibility” with the suture-button fixation method. Further, even if this finding were shown, by virtue of being a cadaveric based study, absent a physiologic setting, we would not be able validate whether or not “flexible fixation” would allow improved ligamentous healing. Future clinical studies could be considered to investigate this issue further.
Previous biomechanical studies have investigated various methods of rigid fixation for midfoot injuries. 1,19 A flexible fixation method by means of a tensioned suture device has been studied with some favorable results at the ankle syndesmosis. 8,21,28,29 To our knowledge, only one other study investigating the use of a similar treatment of the purely ligamentous Lisfranc injury with a tensioned suture-button device has been published. 26 This recently published biomechanical investigation shared a similar rationale for treatment of these injuries with such a tensioned suture-button device. Key differences between the studies are the addition of cyclic loading, force concentration of loads with axial weightbearing to the medial two rays, the injury pattern tested, the use of a standard size tensioned suture-button device (Tightrope®), and the addition of abduction stress. The model tested in their study yielded an average displacement of only 1.3 mm, and it could be argued that such small displacement would not necessarily warrant surgical repair, as this may not represent clinically significant instability. Their injury model involved only a longitudinal transection of just the Lisfranc ligament. The present study mimics the transverse model published by Kaar et al. 15 by additionally disrupting the plantar ligaments between the medial cuneiform and the second and third metatarsal bases at the plantar aspect of the second metatarsal base and intermediate cuneiform. With this injury model, the present study demonstrated a 2.0 mm mean displacement with axial weightbearing, and a potentially more important 6.8 mm mean displacement with abduction stress. As our data and the work of Kaar et al. illustrates, 15 axial loading alone may not best determine the stability afforded by the fixation nor test the plane of maximal displacement of this injury. We believe that testing the fixation devices with an abduction load is a key difference from previous investigations and is an improvement that should be considered in future investigations of the ligamentous Lisfranc injury.
Other differences from previous investigations exist. The present study avoided using the same specimen for a second round of testing with the other fixation device given our findings of specimen attenuation. Unlike the previous study, we elected to load just the medial two rays of the foot with axial loads on the platform. Placing just the first and second rays on the platform allowed us to prevent force dissipation and load sharing through the remainder of the foot and minimized the remainder of the bony and ligamentous architecture of the foot that could act as a reducing force at the Lisfranc complex. In pilot testing, we found that axial loads applied to the entire forefoot led to relatively little motion. This is consistant with the findings of Kaar et al. 15 As a result, we piloted different scenarios of force application with axial loads and found more displacement, although still relatively small, occurred at the Lisfranc complex with just the medial two rays on the platform. Although this differs from the techniques previously seen in the literature, we felt this was an improvement in a biomechanical study attempting to evaluate two fixation devices and their ability to, again, restrain “worst-case scenario” motion. The importance of maximizing displacements was also the rationale for the addition of the abduction stress exams. A final difference included an average age of specimens in our study of 56 years in comparison to 80.5 years.
The ligament pattern for transection was selected based on our desire to test the two different repair constructs on an injury pattern that would most commonly be encountered by treating surgeons, and is another difference from the previous similar investigation. In reviewing the literature, information on the subset of ligamentous Lisfranc injuries and their typical injury patterns is scant. As such, we relied on the recent work of Kaar et al., 15 who demonstrated which structures are likely injured in both the longitudinal and transverse ligamentous Lisfranc injuries. It is doubtful that the purely ligamentous Lisfranc injury is an isolated injury to the Lisfranc ligament. Our clinical experience indicates that the transverse pattern is more often encountered, and therefore this was used in our study, although we did not destabilize the first tarsometarsal complex. Additionally, both clinically and in pilot testing, it is clear that the motion occurring at the Lisfranc complex with the ligamentous injuries is three-dimensional, rather than two-dimensional diastasis. The base of the second metatarsal translates dorsally, while also externally rotating and abducting. In testing, this motion was visibly enhanced with this transverse ligamentous disruption pattern. As a consequence of the decision to utilize a transverse purely ligamentous pattern that destabilized the base of the second metatarsal base, we added supplemental fixation in both of our models, as we felt this mimicked what would be done clinically. In the screw fixation group, a second screw helped stabilize the second metatarsal base to the intermediate cuneiform. In the suture-button fixation group, a Kirschner wire was placed at the same location. The Kirschner wire was utilized as an implant in the flexible fixation model, instead of a screw as was placed in the rigid fixation model, and maintained the rationale of minimizing future surgical hardware removals, minimizing articular damage given the smaller implant diameter compared to a screw, and allowing for slight flexibility. The use of the Kirschner wire as a definitive fixation device has been used historically, 11,12 and despite later studies showing improved rigidity and fixation of Lisfranc injuries treated by rigid internal fixation, 2,18,19 in pilot testing we found that either the screw or the Kirschner wire only supported the primary stabilizing device (i.e., the oblique screw or suture-button between the medial cuneiform and second metatarsal base) and therefore do not feel that the use of the Kirschner wire as secondary supporting device would be of negative functional consequence.
In addition to the limitations and differences discussed above, there are other limitations to the present study. As a cadaveric study, we are unable to investigate the effect that may be seen where physiology and healing may offer further changes over time or with cyclic testing. One thousand cycles was selected based on pilot testing showing a plateau in effect, and as many as 10,000 cycles showed no further change. Soft tissue attenutation, along with likely viscoelastic creep and hysteresis, could have contributed to this effect on the soft tissues around the area of interest, dampening the force distributed. In the absence of physiology, further cycling was not felt to be of benefit. Another concern in this study was the sample size. Because the key findings in this study were those seen with abduction stress, we feel that the statistical inability to show differences in post-fixation motion with either fixation device compared to the post-injury state in axial plane testing, albeit due to being underpowered given small mean motions with high variability, is of less clinical relevance. Power analyses were performed a priori and post hoc to evaluate adequate sample size, and while adequate power was found for abduction testing, a few scenarios in axial load testing revealed such small magnitudes of motion with high variability and associated high standard deviations, that inadequate power likely contributed to some of the statistical findings. To maintain the integrity of the scientific process, none of the outliers were thrown out of this study. Increasing the sample size tremendously would be a way to overcome this issue, but due to constraints of reasonable use of resources and specimen availability, this may not be feasible in cadaveric biomechanical research. An additional method of increasing sample size would have been to reuse specimens for conjugate testing, but for reasons explained above, this was not done.
This treatment method appears to provide adequate restoration of motion to pre-injury levels similarly to the current gold standard of screw fixation. In this era of needed healthcare cost containment, the added expense of an implant such as the one used in this study would have to be offset by improved clinical outcomes and the potential for reduced subsequent expenses, such as future complications and surgical hardware removals. An anatomic reduction continues to be the primary goal of treatment, regardless of the implant utilized. We feel that a tensioned suture-button device could be tested in a randomized, prospective clinical trial in the future.
In conclusion, this study suggests that abduction stress may provide an improved method for diagnosing a subtle transverse ligamentous Lisfranc injury and thus may be a more suitable plane of stress to test fixation devices. We have additionally shown that, even after cyclic testing, which had not been included in prior studies, a tensioned suture button device restrained motion to pre-injury levels similar to the current gold standard. In future studies, we hope to further characterize the three-dimensional motion that occurs at the first and second tarsometatarsal complex in both the intact and injury conditions. Further laboratory and clinical testing may be necessary, but the data afforded by Panchbhavi's et al. 26 study combined with the findings in this study both provide a biomechanical basis to support the use of a suture-button device as a means of flexible fixation in the treatment of the ligamentous Lisfranc injury in future investigations.