
Abstract
Background:
The use of minimally invasive surgical technique for hallux valgus is controversial. The purpose of this study was to retrospectively evaluate the radiographic results of a minimally invasive distal metatarsal osteotomy for correction of hallux valgus.
Materials and Methods:
From September 2005 to March 2008, a minimally invasive distal metatarsal osteotomy was performed in 82 patients (125 feet) for hallux valgus. The average age was 40.8 (range, 13 to 71) years. The mean followup period was 18.3 (range, 9 to 38) months. These patients were categorized into groups based on their gender, age, preoperative hallux valgus angle, and preoperative 1–2 intermetatarsal angle. The radiographs were reviewed for preoperative and final followup hallux valgus angle, 1–2 intermetatarsal angle, and malunion or nonunion. A final followup hallux valgus angle greater than 20 degrees was defined as “recurrence of deformity” and represented a poor radiographic result.
Results:
There were no nonunions but one case of plantarflexion malunion. One case had skin irritation due to prominent bone. A poor radiographic result occurred in 29 feet (23.2%). Of those 36 feet whose preoperative hallux valgus angle was equal or greater than 30 degrees, 23 feet had a poor radiographic result (63.9%). Of those 89 feet whose preoperative hallux valgus angle was less than 30 degrees, only six feet had a poor radiographic result (6.7%) (p= 0.0001). The preoperative 1–2 intermetatarsal angle was found to have no statistically significant influence on poor radiographic results (p = 0.0539). Both the age and sex of the patients had no statistically significant influence (p = 0.8048 and 0.8604, respectively).
Conclusion:
Based on our results, we do not recommend use of this technique to treat moderate to severe hallux valgus (hallux valgus angle, 30) degrees. We believe a traditional open osteotomy with formal capsulorrhaphy would be a better choice of treatment.
Level of Evidence: IV, Retrospective Case Series
INTRODUCTION
Hallux valgus is a common foot deformity with a multifac-torial etiology. 8 More than 130 different methods of operation have been described for the correction of hallux valgus. 4 Current trends for treatment are toward more limited invasive procedures, with the desire for a more rapid recovery, a smaller operative wound, and shorter operative time. A percutaneous transverse distal metatarsal osteotomy reported by Bosch et al. 1 showed good clinical results. Magnan et al. 6 and Giannini 2 also reported good results using this percutaneous technique. On the contrary, Kadakia et al. 3 reported an unacceptable rate of complications associated with high recurrence rate after using the percutaneous technique described by Giannini. 2 Although the use of a minimally invasive surgical technique for hallux valgus is still controversial, we were encouraged by the success of Magnan 6 and Giannini 2 and started to perform this minimally invasive osteotomy for correction of hallux valgus in September 2005. The goal of this study was to evaluate the radiographic results of this minimal incision (or so-called “percutaneous”) distal metatarsal osteotomy performed and determine if there was any limitation of using this technique.
MATERIALS AND METHODS
From September 2005 to March 2008, 82 patients (125 feet) with hallux valgus underwent minimally invasive distal metatarsal osteotomy. Forty-three patients had bilateral operations, simultaneously. All operations were performed by the senior surgeons. All but three feet had mild to moderate hallux valgus deformity as defined by a hallux valgus angle less than 40 degrees. The other three feet had preoperative hallux valgus angle of 40.4, 43.8, and 42.6 degrees, respectively. The patient population consisted of 78 females (120 feet) and four males (5 feet). The average age of the patients was 40.8 (range, 13 to 71) years. The average followup period was 18.3 (range, 9 to 38) months. Patients with severe degeneration of first metatarsophalangeal joint, rheumatoid arthritis, and hallux rigidus were not included in this study. Patients with a congruent metatarsophalangeal joint were also excluded. Conservative management failed in these patients. Nine patients (nine feet) underwent lesser metatarsal osteotomy also due to severe lesser toe metatarsalgia.
Surgical procedure
The patients were placed in the supine position with a thigh tourniquet. Our surgical procedure was based on the technique described by Magnan et al. 7 A 1-cm skin incision was made centered over the medial aspect of the first metatarsal neck (Figure 1). The periosteum was elevated, and the intended osteotomy site was visualized. The osteotomy was done at the subcapital level with an oscillating saw in a single plane, perpendicular to the first metatarsal shaft axis. A 2.0-mm Kirschner wire was inserted manually in a distal-to-proximal direction along the medial aspect of the first metatarsal head in a subperiosteal position until the tip was observed in the wound. Lateral translation of the metatarsal head fragment was done, and the Kirschner wire was introduced under direct vision into the medullary canal of first metatarsal shaft. During this procedure, the hallux valgus angle was corrected to slight overcorrection. The wire was then driven through the first tarsometatarsal joint for more stability. The medial sharp edge of the proximal metatarsal was not trimmed because this part provided stability to the Kirschner wire. Weightbearing was permitted on the day after surgery in a stiff-soled postoperative shoe. The wire was removed at the 6th week postoperatively, and the patients were allowed to wear normal shoes then.
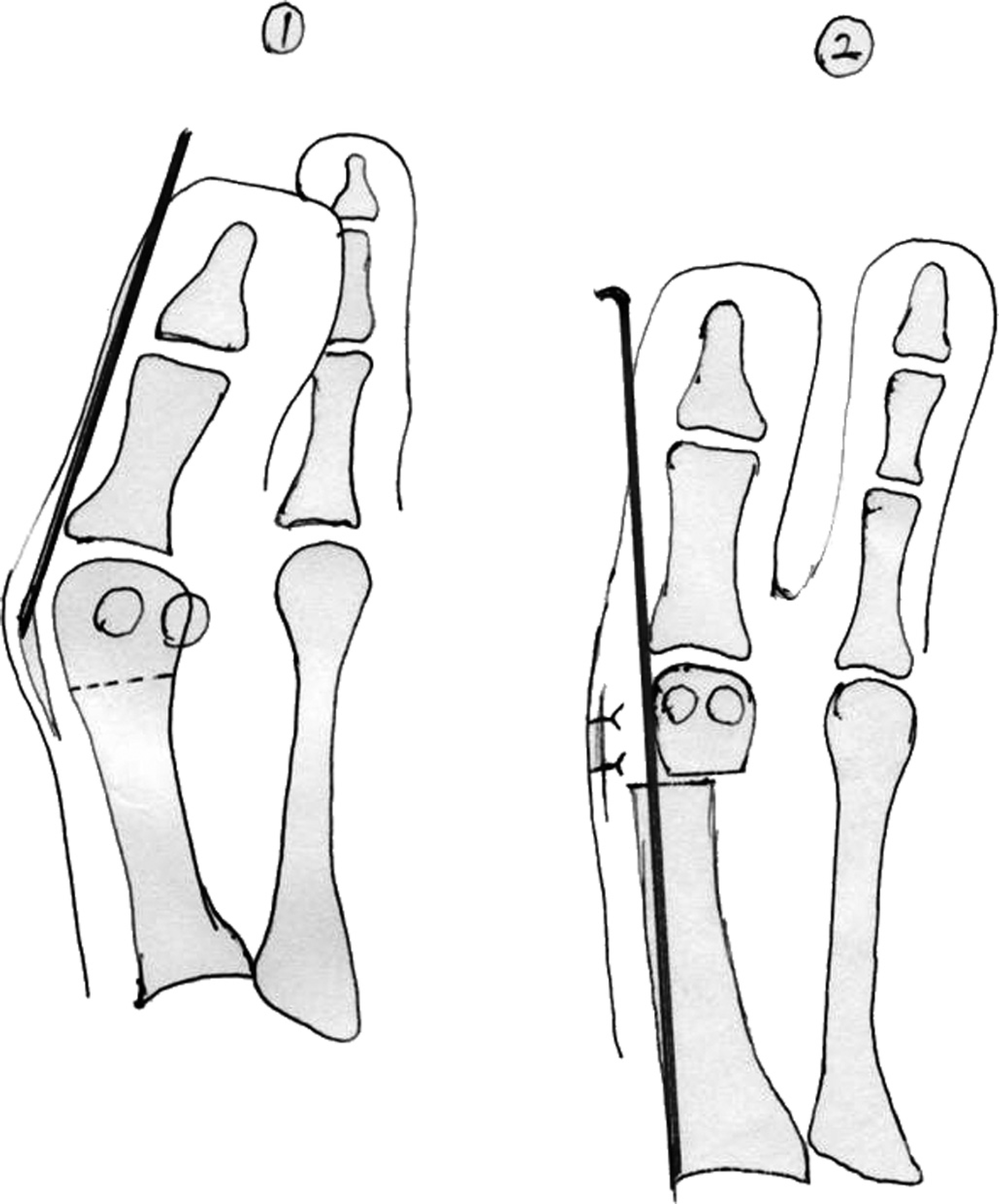
Surgical procedure: A 1-cm skin incision was made centered over the medial aspect of the first metatarsal neck. The osteotomy was done at the metatarsal neck perpendicular to the first metatarsal shaft axis and a 2.0-mm Kirschner wire was inserted manually in a distal-to-proximal direction along the medial aspect of the first metatarsal head until the tip was observed in the wound. The metatarsal head fragment was shifted laterally and the Kirschner wire was driven intramedullary to the first tarsometatarsal joint.
Radiographic evaluation
The preoperative hallux valgus angle, 1–2 intermetatarsal angle were recorded from weightbearing radiographs. We used the center of the articular surface of the metatarsal head and the proximal articulation as reference points to draw the first metatarsal axis. All measurements were done by a single person to decrease potential bias. All patients were available for followup radiographic review. The followup hallux valgus angle, 1–2 intermetatarsal angle were recorded. We defined “a poor radiographic result with recurrence” as a final followup hallux valgus angle greater than 20 degrees. Any radiographic sign of nonunion or malunion was also recorded.
Statistical analysis
The recurrence rates for different characteristics of patients were compared by Chi-square tests. In addition, to consider the followup time, log-rank tests were also used for comparison.
RESULTS
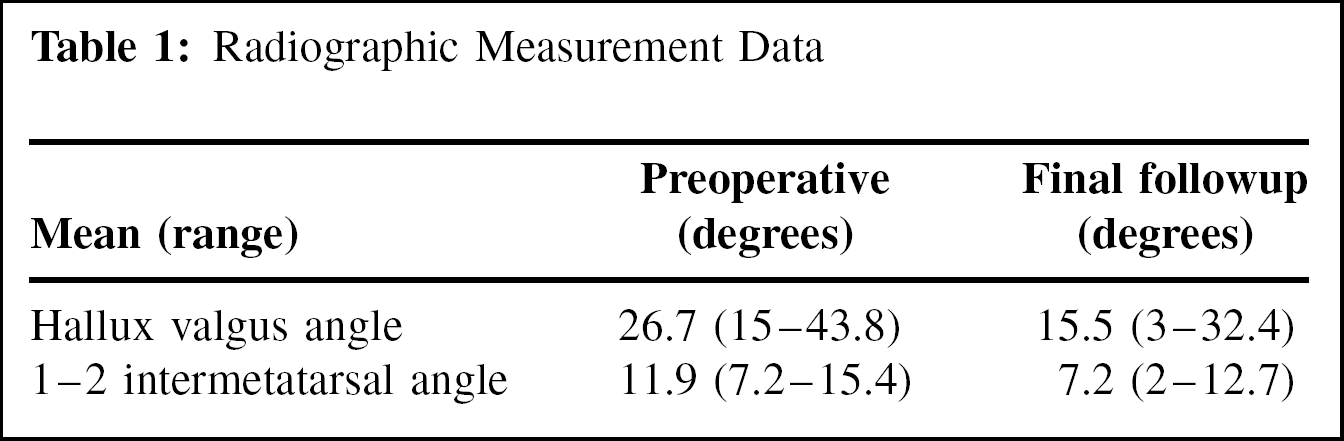
The mean preoperative hallux valgus angle (HV angle) was 26.7 (range, 15 to 43.8) (Table 1). The mean preoperative HV angle for the group with preoperative HV angle less than 30 degrees was 23.7 degrees. The mean preoperative HV angle for the group with preoperative HV angle > 30 degrees was 34.1 degrees. The mean preoperative 1–2 intermetatarsal angle was 11.9 (range, 7.2 to 15.4) degrees. The mean final followup hallux valgus angle was 15.5 (range, 3 to 32.4) degrees. The mean final followup 1–2 intermetatarsal angle was 7.2 (range, 2 to 12.7) degrees. The average improvement of hallux valgus angle was 11.2 degrees, and the average improvement of 1–2 intermetatarsal angle was 4.7 degrees.
Radiographic Measurement Data
29 feet had poor radiographic results (Table 2). The hallux valgus recurrence rate was 23.2%. For the 89 feet with preoperative hallux valgus angle less than 30 degrees, 6 feet had poor radiographic results for a recurrence rate of 6.7%. But for the 36 feet with preoperative hallux valgus angle greater than 30 degrees, 23 feet had poor radiographic results for a recurrence rate of 63.9% (p = 0.0001). Both the age and gender of the patients were not found to have significant influence on the radiographic result. Although theoretically, the severity of hallux valgus deformity is related to 1–2 intermetatarsal angle, the influence of the preoperative 1–2 intermetatarsal angle on final radiographic result was not statistically significant with the numbers available (p = 0.0539).
Comparison of Recurrence Rates Among Patients’ Characteristics
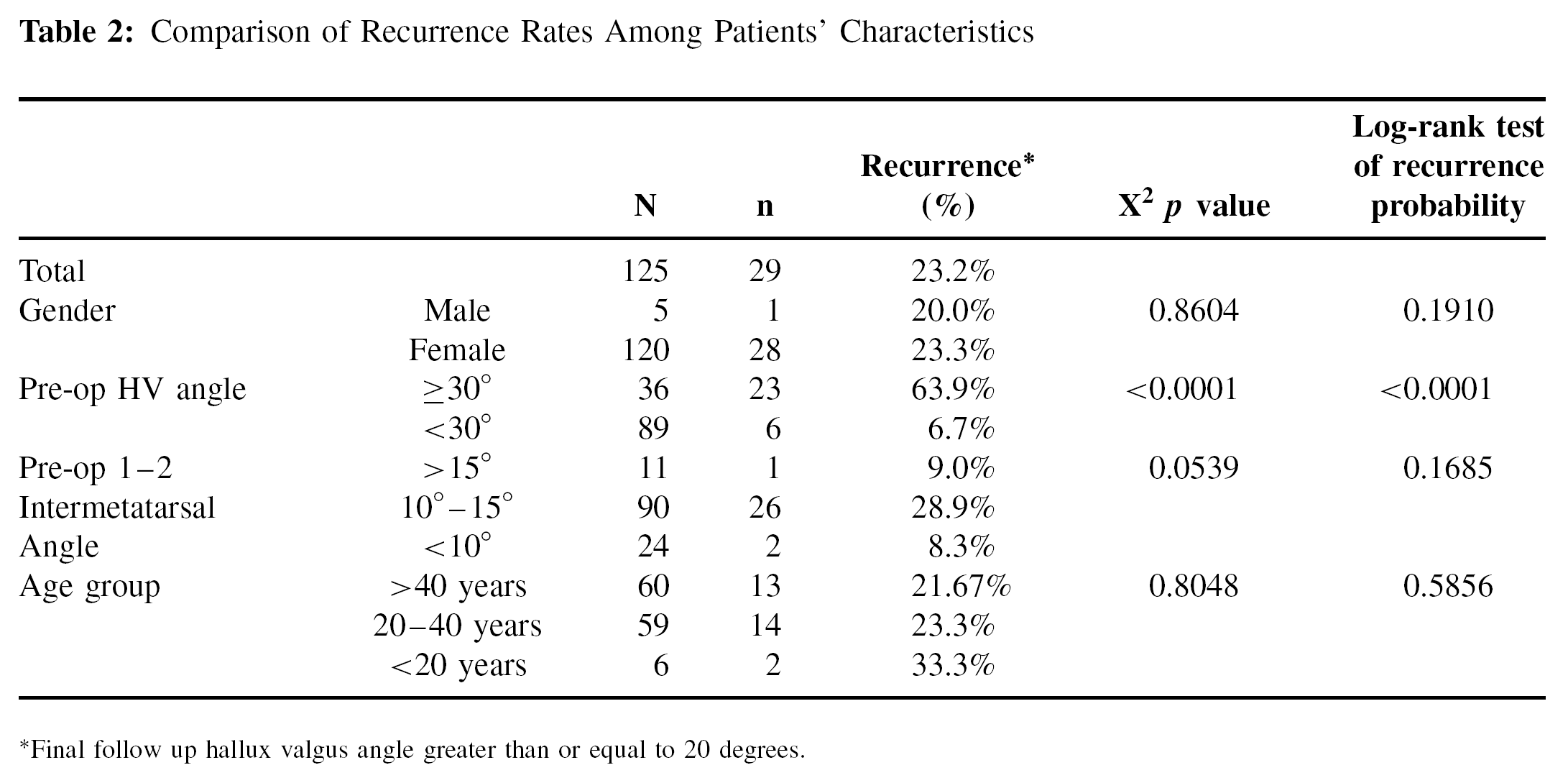
Final follow up hallux valgus angle greater than or equal to 20 degrees.
Complications
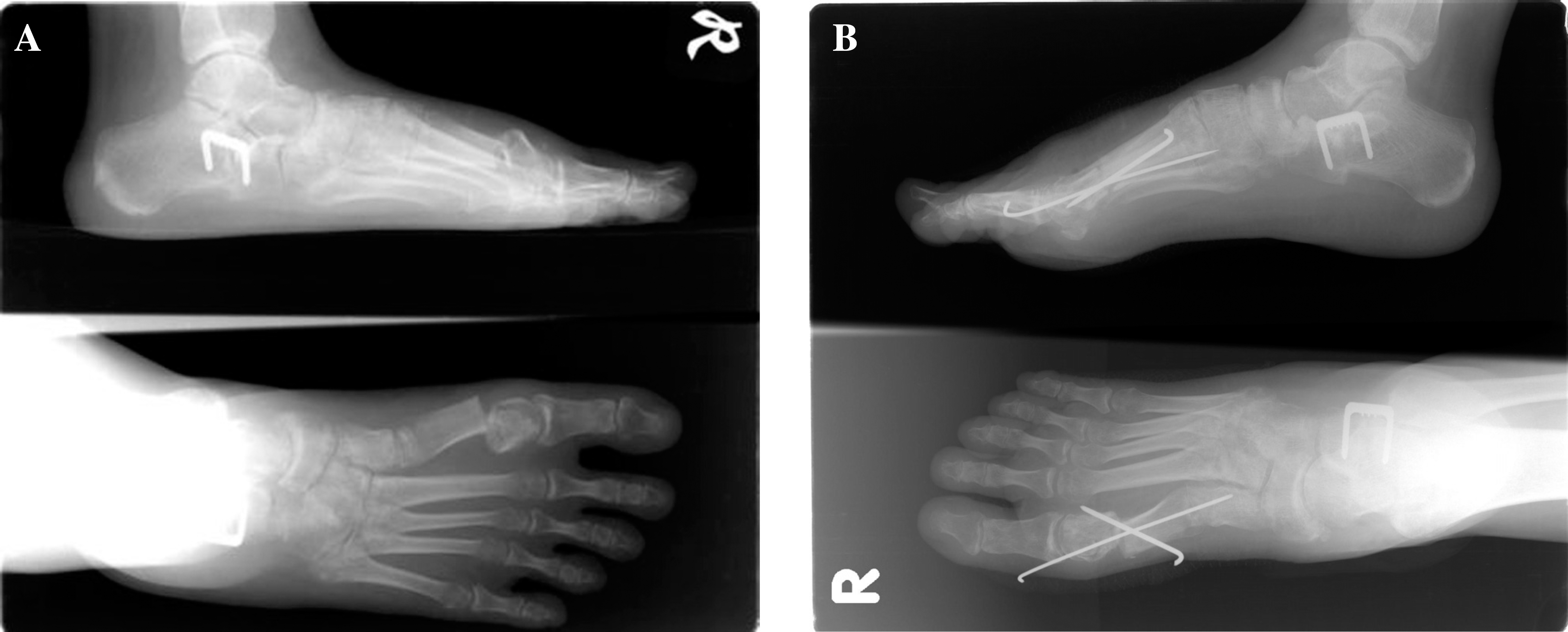
There was no case of nonunion but one case was found to have plantar angulation of the head fragment at the 6th week followup. This patient underwent revision surgery (Figure 2). The Kirschner wire was repositioned and the plantar angulation was corrected. One patient experienced skin irritation due to the untrimmed edge of proximal fragment and subsequently underwent ostectomy. The most often encountered complication other than recurrence was superficial skin infection related to the pin (11 feet, 8.8%). This problem was handled with pin tract care and oral antibiotics. All cases healed uneventfully.
DISCUSSION
Percutaneous distal transverse metatarsal osteotomy was first described by Bosch et al. 1 Giannini et al. 2 and Magnan et al. 6 also reported good results using a similar technique. The benefits of this minimally invasive osteotomy were smaller wound, shorter operative time and theoretically decreased morbidity. However, this minimally invasive surgery should be able to produce the same therapeutic effect as the other traditional distal metatarsal osteotomies. Although Magnan et al. 6 and Giannini et al. 2 demonstrated good results using this percutaneous osteotomy, Kadakia et al. 3 reported poor results after their trial of 13 cases and they did not recommend this technique due to complications including dorsal malunion and recurrence of hallux valgus.
Based on our results, we found the average improvement of hallux valgus angle and 1–2 intermetatarsal angle was 11.2 degrees and 4.7 degrees, respectively. Although this difference was statistically significant, the power of correction for hallux valgus angle was apparently not enough for those patients whose preoperative hallux valgus angle was greater than 30 degrees. In this patient group, the hallux valgus recurrence rate was 63.9%.
We believe that the major drawback of this minimal incision technique is it is a pure extra-articular procedure without a formal capsular plication. The soft tissue balance is not completely corrected at the time of surgery. The hallux valgus angle correction obtained during the operation depends on the transfixation of the joint capsule by the Kirschner wire. Although slight overcorrection of the hallux valgus angle was achieved intraoperatively, after removal of the wire, loss of correction occurred and this contributed to the recurrence noted in our study. For those patients with radiographic recurrence, the patients noted the deterioration of the correction after removal of the Kirschner wire. This phenomenon was especially obvious in patients with more severe preoperative hallux valgus deformity which resulted in a high dissatisfaction rate among these patients. According to Magnan et al., 6 the lack of soft tissue surgery does not appear to affect the prevalence of recurrent hallux valgus deformity. However, we were not able to reproduce the same good results using this minimal incision surgery. The hallux valgus recurrence rate for mild deformity (hallux valgus angle ≥ 30) degrees was 6.7%, which was still higher than our series of traditional distal metatarsal osteotomy with capsular plication. 5 For more severe deformity (hallux valgus angle ≥ 30) degrees, the hallux valgus recurrence rate was 63.9%. This was unacceptably high compared to our series of traditional distal metatarsal osteotomy.
After using percutaneous distal metatarsal osteotomy, Kadakia et al. 3 reported a high rate of complications including dorsal malunion (69%) and recurrent hallux valgus (38%). In our series, the hallux valgus recurrence rate was 23.2%. We considered this rate correlated with Kadakia's series because the criteria for hallux valgus recurrence was 15 degrees in their series and 20 degrees in our series. This may have resulted in our slightly lower recurrence rate compared to their series. As for the complication of malalignment, we only found one case developing plantar malalignment in our 125 feet. The sagittal alignment of the subcapital fragment was generally preserved in our series.
CONCLUSION
Although our series showed that correction of both the hallux valgus angle and 1–2 intermetatarsal angle was obtained using this minimal incision osteotomy, the correction often decreased after removal of the Kirschner wire. Without formal plication of the joint capsule, it was difficult to control and maintain the alignment. We suggest that, for mild hallux valgus deformity (hallux valgus angle ≥ 30) degrees, although this minimal incision surgery could achieve deformity correction with the benefits of a smaller wound and shorter operative time, the surgeons should bear in mind that this technique still has a higher hallux valgus recurrence rate (6.7% in our series) compared to other traditional distal metatarsal osteotomies. For more severe hallux valgus deformity (hallux valgus angle ≥ 30) degrees, this surgery had an unacceptably high rate of recurrence Thus, we suggest it not be used in this patient group.