
Abstract
Background:
High rates of arthrodesis nonunion have been described in the ankle, hindfoot and midfoot in patients with significant risk factors. The purpose of this study was to evaluate fusion rates, risk of reoperation, postoperative pain scores and patient satisfaction for a slot graft inlay arthrodesis technique used in a high-risk group of foot and ankle patients.
Materials and Methods:
We retrospectively reviewed all ankle, hindfoot and midfoot arthrodeses by two foot and ankle surgeons in our institution between January 2000 and January 2009. Seventeen arthrodesis procedures in 16 patients using the slot graft technique were identified. Patient charts were reviewed for medical history, risk factors, previous surgery and postoperative complications. Time to union was evaluated on radiographs. Patients provided final followup by phone with an assessment of pain, overall satisfaction and use of orthotic or assistive devices.
Results:
Union occurred in 13 arthrodesis procedures (77%) with an average time to union of 5 months. Postoperative infection occurred in one patient. Additional surgery was performed in nine patients. At final followup patients reported low pain scores (3 of 10) and high satisfaction (8 of 10). Fourteen of 15 patients contacted indicated that they would choose to undergo the procedure again.
Conclusion:
The slot graft arthrodesis technique provided satisfactory results in this small group of patients with a low complication rate. Patient satisfaction rates were high with low pain scores at an average of 62 months postoperatively.
Level of Evidence: IV, Retrospective Case Series
INTRODUCTION
Arthrodesis in the foot and ankle is a common solution for end stage arthritis. Although total ankle arthroplasty is becoming more widespread, ankle arthrodesis remains the best treatment option for many patients and is often required for salvage after failure of total ankle arthroplasty. In addition, for joints of the hindfoot and midfoot, fusion is usually the only option.
Nonunion is a well-known potential complication associated with primary or revision arthrodeses of the foot and ankle. Historically, nonunion rates for ankle arthrodesis have been reported as high as 41%. 13 With advances in surgical technique as well as newer implants, more recent studies have reported lower nonunion rates from 0% to 28%. 12,16,23,26,36 Primary subtalar and midfoot fusions have lower reported nonunion rates compared to ankle arthrodesis. However, patients with known risk factors for nonunion present a challenge for the foot and ankle surgeon regardless of the joint fused. Patient demographics, compliance with postoperative instructions, prior surgery, underlying medical comorbidities, medications, and operative technique can influence the development of nonunion. Multiple risk factors have been identified in the literature including tobacco use, avascular necrosis of the talus, infection and a history of open injury. 1,7,13,18,26 In many cases, multiple risk factors exist in a single patient. Other medical conditions associated with nonunion include drug and alcohol use, psychiatric history and diabetes. 26 High rates of nonunion have also been reported in rheumatoid patients. 23
The purpose of our study was to evaluate fusion rates, risk of reoperation, postoperative pain scores and patient satisfaction for a slot graft inlay arthrodesis technique used in a high-risk group of foot and ankle patients.
MATERIALS AND METHODS
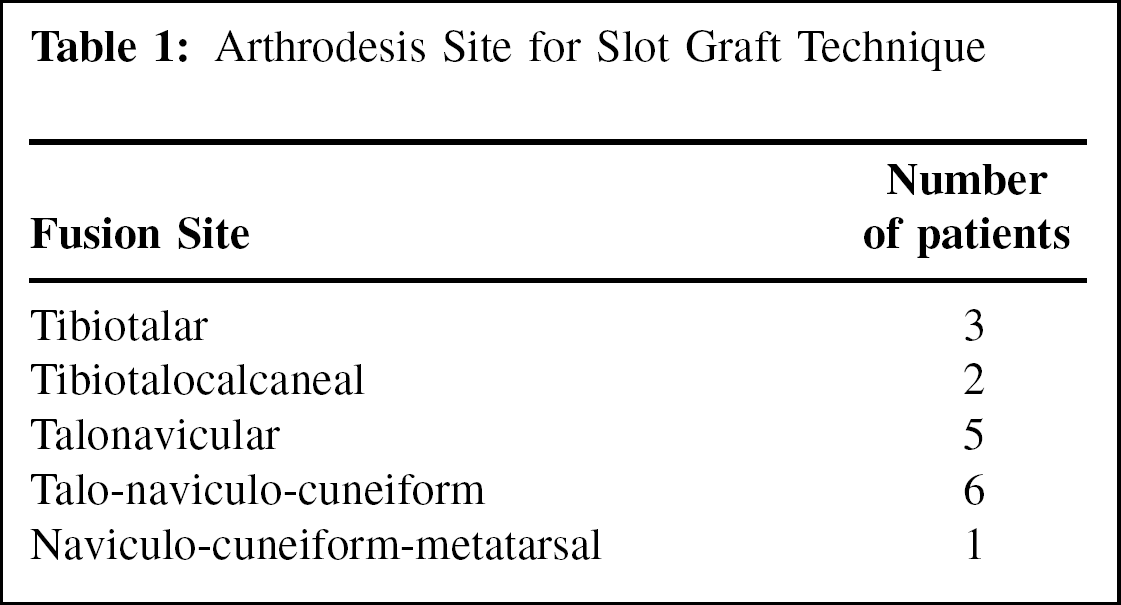
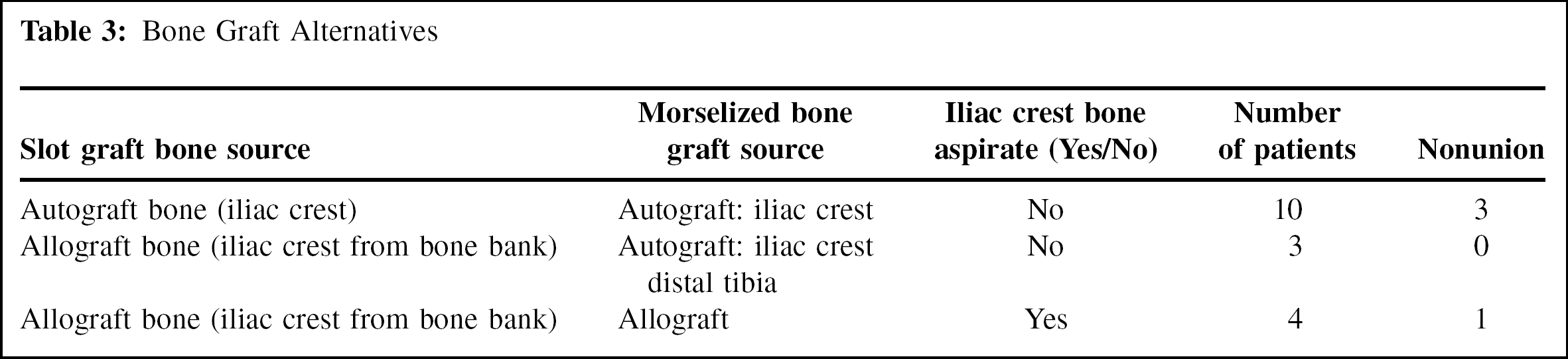
Internal Review Board approval for this study was obtained through the Human Research Protection Office of our institution. We retrospectively reviewed all ankle, hindfoot, and midfoot arthrodeses by two foot and ankle surgeons in our institution between January 2000 and January 2009, and a total of 277 cases were identified. Patient operative notes were reviewed for use of a slot graft technique of arthrodesis. Seventeen arthrodesis procedures in 16 patients using the slot graft technique were identified. Ten women and six men underwent ankle, hindfoot or midfoot fusions (Table 1) with this technique between February 2001 and September 2008. The mean age of the patients at the time of surgery was 50 years old. Nine of 17 surgeries included arthrodesis of multiple joints. Tricortical iliac crest autograft was used in ten cases and frozen tricortical iliac crest allo-graft bone was used in seven. The choice to use allograft or autograft bone was based on surgeon preference.
Arthrodesis Site for Slot Graft Technique
Patient charts were retrospectively reviewed for medical history, prior operative procedures and risk factors for nonunion. The operative notes were reviewed for intraop-erative findings that influenced the surgeon's decision to use this technique. In addition, subsequent surgeries and postoperative complications including nonunion were recorded.
Postoperative radiographs were reviewed by a separate fellowship trained orthopaedic foot and ankle surgeon who was not involved in the care of the patient but is a partner in the treating surgeon's practice. Time to fusion in months was identified by radiographic evidence of complete fusion. Radiographic criteria of a solid fusion included evidence of trabecular bone crossing the fusion site and lack of hardware loosening or failure.
Clinical followup averaged 18 (range, 3 to 54) months. Fifteen of 16 patients were evaluated by phone at an average of 62 (range, 20 to 112) months postoperatively and questioned regarding postoperative pain scores and subjective patient satisfaction. Patients were asked to rate their pain on a 10-point scale with 0 representing no pain and 10 the worst possible pain. Satisfaction ratings were also obtained by phone on a 10-point scale with 0 indicating that patients were dissatisfied with their outcome and 10 indicating the highest level of satisfaction. Patients were questioned about the use of an assistive device, orthotics, bracing and specialized foot wear.
Operative technique
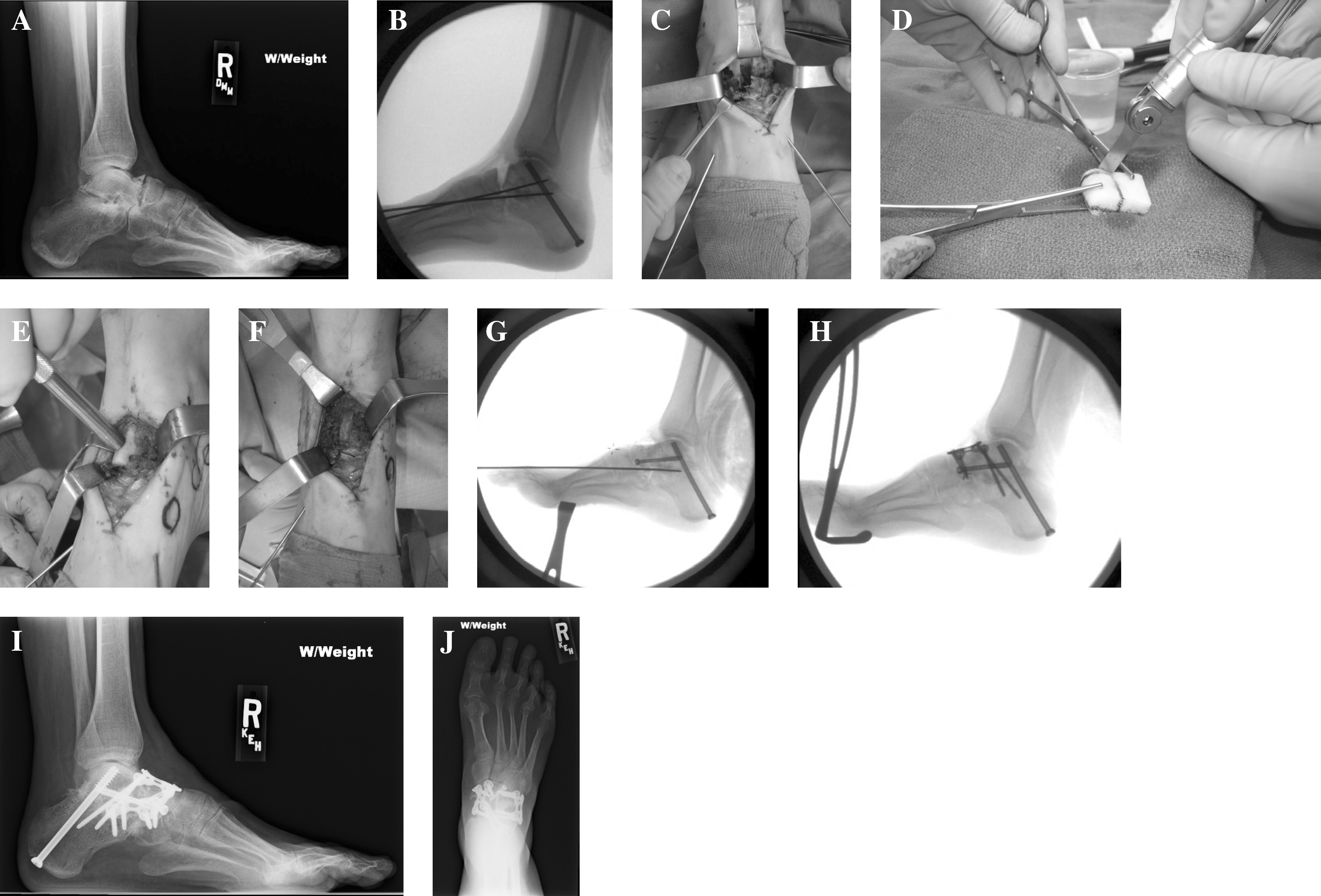
A representative case example of the slot graft technique is illustrated in figure 1. The surgical limb was prepared and draped as well as the ipsilateral iliac crest in the cases when autograft bone was harvested. A pneumatic thigh tourniquet was used in all cases. The joint(s) to be fused were exposed through standard approaches. Once the joint was exposed, a thorough preparation of the joint surfaces was performed. All remaining cartilage was removed from the articular surface and all necrotic or avascular bone was de'brided. Once the surfaces were completely prepared, the joints were copiously irrigated and final preparation with multiple drill holes in the surfaces of bone to be fused was performed.
Once reduced and fixed in appropriate alignment, a slot or rectangular trough was created using a sagittal saw across the joints to be fused. The length of the slot varied by location, but all slots were created approximately 6 mm to 1 cm wide and 1 to 1.5 cm deep. The allograft or autograft tricortical iliac bone was fashioned into the appropriate dimensions using the sagittal saw. The graft was soaked in unconcentrated autogenous iliac crest bone marrow aspirate in four cases. The specific type of grafts used are outlined in Table 2. A bone tamp and mallet were used to impact the bone into place to create a press fit. Morselized bone graft was then packed around the slot graft prior to placing final fixation. The postoperative protocol included 6 weeks of nonweightbearing in a splint or cast followed by 4 weeks in a weightbearing cast. At 10 weeks postoperatively, patients were transitioned into a walker boot for up to 4 to 6 additional weeks. The length of nonweightbearing was doubled in patients with diabetes and peripheral neuropathy.
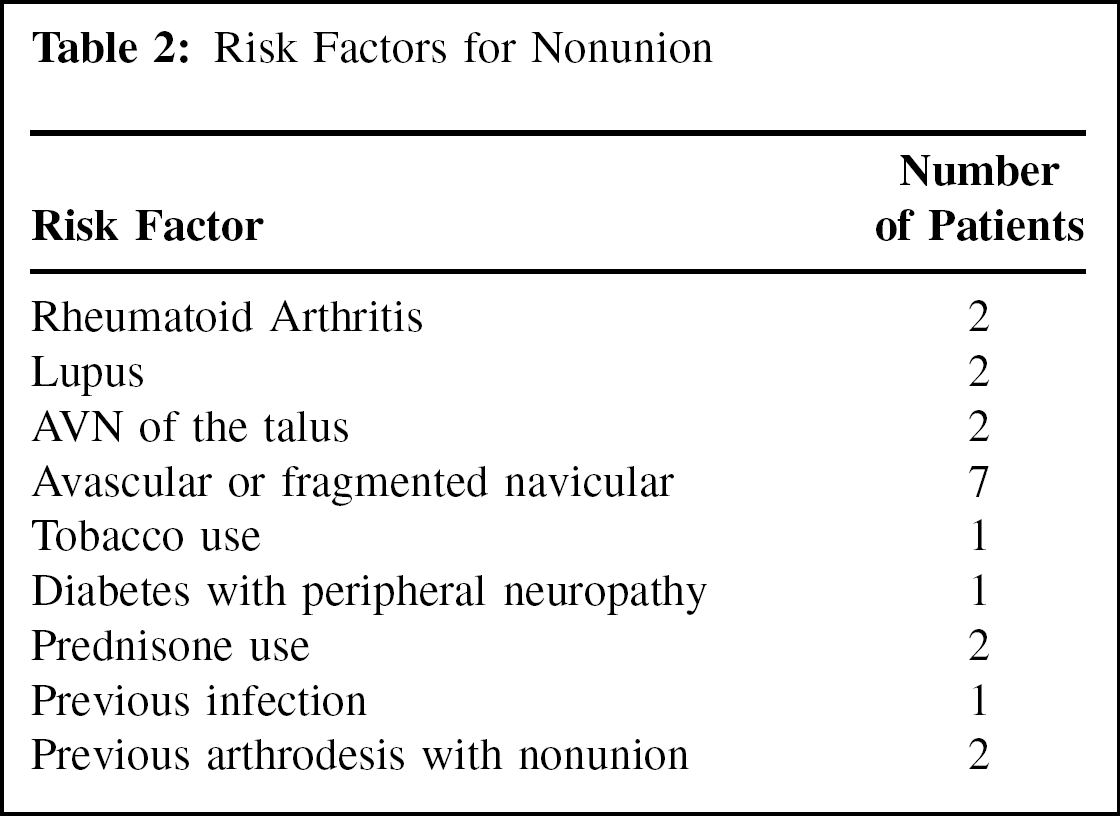
Risk Factors for Nonunion
RESULTS
All patients had at least one risk factor and four patients had greater than one risk factor (Table 3). Eight patients had a history of prior surgery and two patients presented with a nonunion of a previously attempted fusion. Intraoperatively, sclerotic, avascular or fragmented bone was identified as a risk factor for nonunion resulting in a decision to use the slot graft technique in six patients without other identifiable risk factors. In the two patients with a nonunion of a previous arthrodesis, there was no clinical evidence of infection.
Bone Graft Alternatives
Postoperative infection occurred in one patient with a history of lupus. Nonunions were noted in four patients. Three of these patients had iliac crest autograft used in the slot graft. Additional surgery was performed in nine patients for hardware removal (five), nerve release (two), revision fusion (three) and treatment of an ipsilateral tibia fracture (one). Three of the four patients with nonunion were treated with revision surgery with successful fusion in two patients.
The average time to complete radiographic union was 5 (range, 3 to 10) months. At the time of telephone followup, patients rated their current satisfaction as 8 on average (range, 5 to 10 with 10 indicating most satisfied). Pain scores averaged 3 (range, 0 to 6.5 with 10 indicating severe pain). Fourteen of the 15 patients contacted indicated that they would undergo the surgery again. Two patients still required an assistive device when walking and nine patients reported the use of an orthotic, brace, or specialized footwear. Even in patients with nonunion after a slot graft technique, the average satisfaction rating was 9.3 (range, 8 to 10) and all indicated that they would undergo surgery again. Pain scores averaged 3 for patients with nonunion (range, 1 to 6). These patients were contacted at an average of 5 years after their original surgery.
DISCUSSION
Nonunion after foot and ankle arthrodesis is a challenging problem faced by all foot and ankle surgeons. Nonunion rates as high as 41% 13 have been reported for the ankle, while midfoot and subtalar arthrodesis are associated with lower rates of nonunion 9,29 except in the case of a high-risk patient. Multiple factors are associated with nonunion including avascular necrosis, infection, open fractures, tobacco use and medical conditions such as psychiatric disorders, rheumatoid arthritis or diabetes. 3,7,13,18,23,26,31
Many specialized techniques and use of adjuncts to fusion have been described to address the high rates of nonunion especially in high-risk patients. Use of autologous bone graft or bone morphogenic protein has been shown to increase fusion rates. 4 Some authors favor the use of bone stimulators for primary fusions in high-risk patients. 10 The use of bone stimulators has mixed results when used for nonunion or delayed union. 10,14,28 Specialized operative techniques have also been described in small groups of patients with one or more risk factors. Grafting with vascularized fibular grafts, creating dowels or inlay grafting are all considerations in the high-risk patient. 19,27,32,35,37 Biomechanical studies have improved our understanding of the best fixation techniques to reduce the risk of nonunion. 5,6,8,14,17,24,25,30,33,34
Failure of revision procedures has also been reported with relatively high rates and occasionally below-knee amputation is the final salvage operation. 1,11,21,28,31,38 Even when arthrodesis is successful, postoperative complications are common and patients occasionally report high levels of pain postoperatively. 1,22 The reported level of patient satisfaction after arthrodesis varies in the literature. Arthritic changes in adjacent joints can cause ongoing pain and dysfunction. Malunion or a poorly positioned arthrodesis also contributes to poor outcome.
Many techniques to improve union rates in high-risk foot and ankle arthrodeses have been described. This is not the first description of an inlay or structural graft technique for complex fusions of the foot or ankle. In 1921, Hoke described a type of structural grafting using the head and neck of the talus to correct deformity in a paralytic foot. 15 Johnson and Johnson described a technique of dowel graft arthrodesis in 15 patients undergoing arthrodesis for post traumatic arthritis of the tarsometatarsal joints. 19 They report three nonunions, two of which were later treated with an inlay bone graft technique. Similar to our results, most patients reported only mild or no pain at final followup (12 of 13).
Petj et al. described a similar technique in a group of 11 patients treated for post-traumatic arthritis and flat foot deformity. 27 Arthrodesis of the naviculocuneiform and first tarsometatarsal joint was performed using an iliac crest structural inlay graft technique to stabilize the medial column. Additional joints were fused using a dowel grafting technique as described by Johnson and Johnson. 19 Joints were fixed using smooth wires that were removed after 3 months. The authors report a 100% union rate and good or excellent results in all patients using a clinical scoring system described by Arntz et al. 2 The authors did not comment on the preoperative risk factors for nonunion in this group of patients. Our patient group included several patients with post-traumatic ankle arthritis or arthritic changes throughout the midfoot. In comparison to Petj et al., we used this technique in patients with a higher risk for nonunion.
Our technique is modified from one described by Johnson in which a trough is created across the intertarsal joints of the midfoot. 20 A tricortical iliac crest graft is harvested en bloc and split longitudinally into two cortical cancellous strips that are placed into the trough with the strips oriented cortex to cortex. Morselized bone graft is then packed around the strips and into the joint spaces prior to insertion of internal fixation. Johnson did not report clinical results or fusion rates using this technique.
Verhulst and Swierstra reported a technique of posterior inlay grafting for ankle nonunions with non structural cancellous bone graft. 35 These authors packed a 2 cm × 3 cm × 2 cm “slot” across the ankle with cancellous bone graft in 11 patients with nonunions. Successful fusion was achieved in 10 of 11 patients with this technique. Sward et al describe this same technique in 19 ankle arthrodeses with successful fusion in 16 patients (15% nonunion).32 The overall nonunion rate in our group of patients was 23% which is consistent with reports in the literature of fusion in patients with a high risk for nonunion.
Yajima et al. described a technique using vascularized fibular grafts in seven patients with onlay grafting in two and inlay grafting in five patients. 37 The authors report successful union in six patients with radiographic union at an average of 6 months. One patient required revision surgery. Risk factors for nonunion in that study closely matched those in our group of patients. The average time to radiographic fusion was similar. It is difficult to compare fusion rates with a small number of patients; however, vascularized grafting across the fusion site does not seem to provide additional benefit compared to the autograft or allograft bone used in our series.
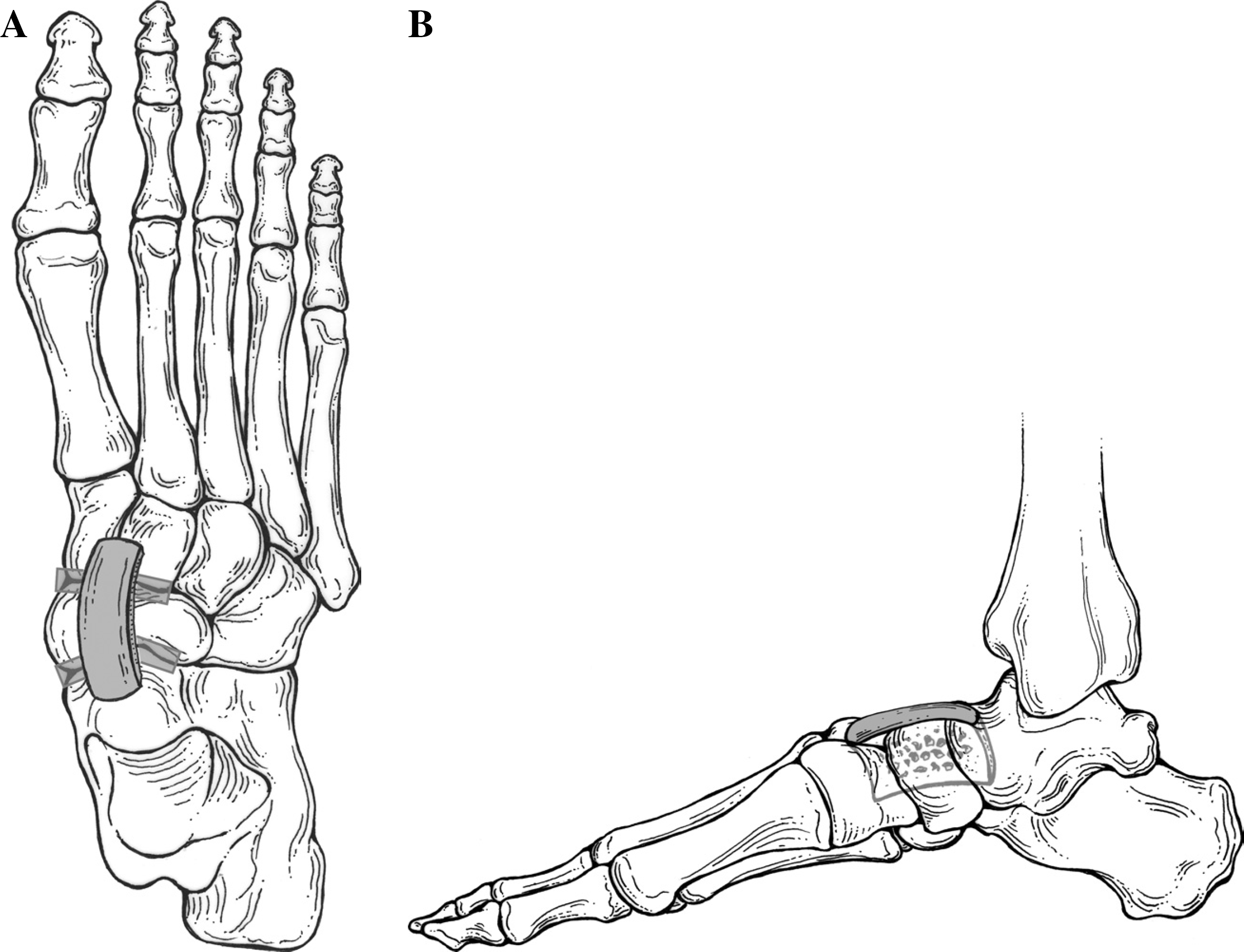
We believe the slot graft technique for augmentation of fusion has particular advantages over other techniques for several reasons, especially in the midfoot. The slot graft seems to provide additional fixation by the press fit nature of the graft being impacted into the trough, especially in resistance of rotational stresses. In addition, the dorsally placed bone graft helps to resist plantar midfoot collapse with weightbearing stresses with the graft acting much like the keystone of a Roman arch as illustrated in figure 2. We hypothesize that the intact ligaments on the plantar aspect of the midfoot joint and the intact plantar fascia create additional compression of the dorsally placed bone graft through a tension band effect. The slot graft technique may be extended from the talonavicular joint into the midfoot joints as part of an extended medial column triple arthrodesis or an isolated medial column fusion (figure 3).
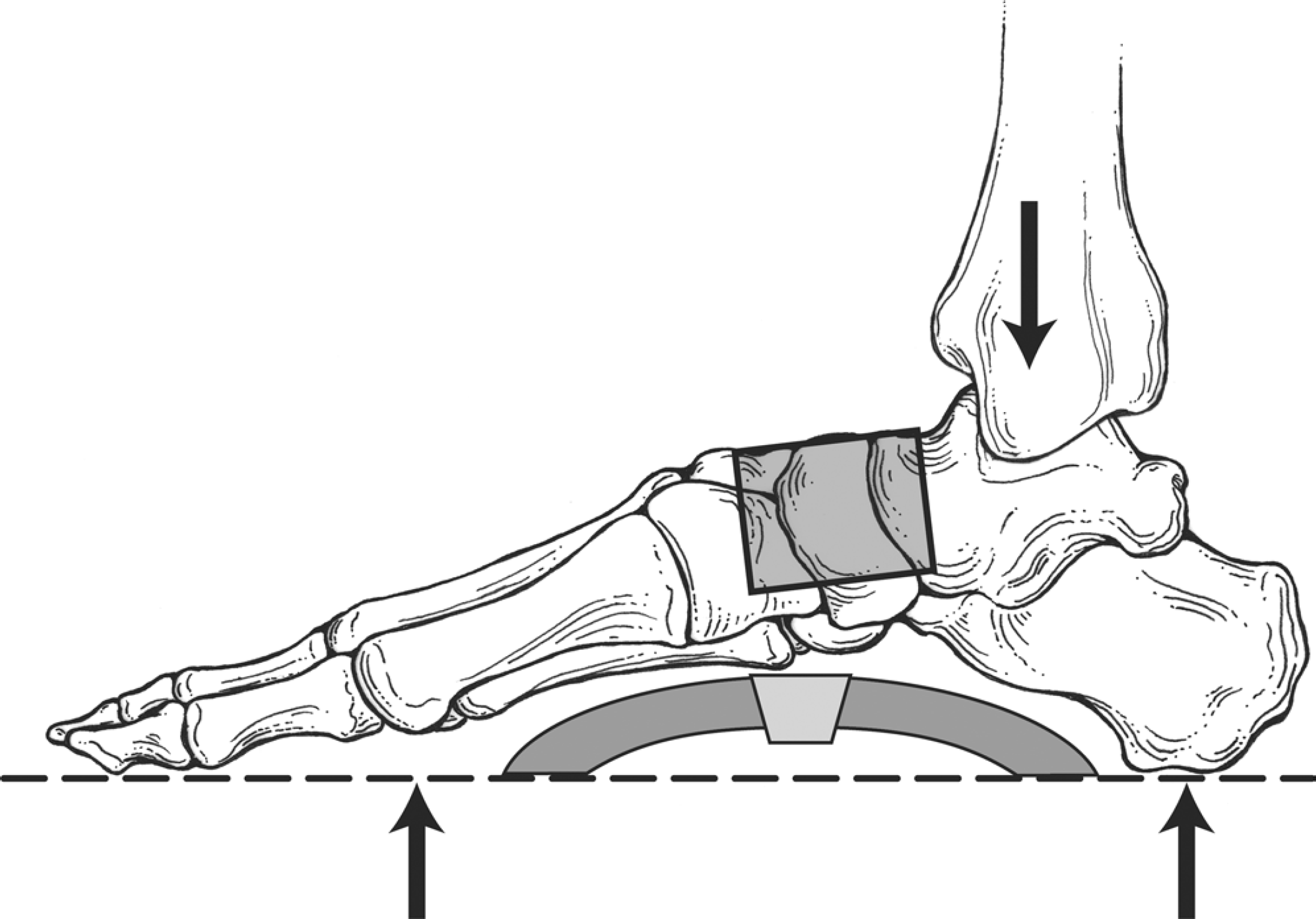
Illustration of the weightbearing stresses transmitted through the tibia (downward arrow) with the ground reaction forces (upward directed arrows) with the dorsally placed slot graft acting as a keystone in a Roman arch configuration.
Many techniques other than bone grafting have been described to reduce the risk of nonunion in high-risk patients. Arthroscopic ankle fusion is associated with a lower rate of nonunion and faster union rates in the literature. 12,36 This technique is a consideration to improve union rates in the uncomplicated isolated ankle fusion. Bone stimulators have been studied in both primary and revision settings in foot and ankle arthrodesis. Donley and Ward report an ankle and hindfoot union rate of 92% in a group of high-risk patients treated with standard fusion techniques, bone grafting and implantable bone stimulators. 10 These authors concluded that bone stimulation were a useful adjunct in the high-risk patient.
Bone morphogenetic proteins are a more recent area of study in high-risk ankle and hindfoot fusions. Bibbo et al. evaluated 112 fusion sites in 69 patients with at least one risk factor for nonunion. 4 Overall fusion rate was 96%. While adjuvants can improve the rate of fusion in these high-risk groups, most authors emphasize that they are not a substitute for meticulous operative technique and the high cost of these devices limits their widespread use.
There are several limitations to this study, most notably the small sample size, the retrospective design of the study and the lack of a control group. However, the 16 patients in our study were comparable to other similar studies in the literature. Our criteria for a successful arthrodesis was based on radiographic evaluation by an experienced fellowship trained orthopaedic foot and ankle surgeon. Although computed tomography (CT) was not utilized, we feel that trabecular bone crossing the fusion site and the absence of any evidence of hardware failure or loosening is a reasonable indicator of a solid fusion. Finally, a phone interview followup was performed instead of a face-to-face history and physical examination. Since joint range of motion was not one of the determinants of outcome, and we feel that a telephone interview by an orthopaedic fellowship trained foot and ankle surgeon who was not involved with the surgery was a reasonable next best method of data collection.