
Abstract
Background:
A special type of trimalleolar fracture with the involvement of the entire posterior tibial plafond has been reported recently. Because of the low incidence, the characteristics of the fracture in different studies have not been consistent. We describe our clinical experience with this fracture type.
Materials and Methods:
From January 2007 to December 2009, 12 patients were identified with a trimalleolar fracture with involvement of entire posterior tibial plafond. All the fractures were openly reduced and fixed through a combined operative approach (posterolateral and posteromedial). Ten of 12 patients were followed up. The clinical outcome was assessed with the Short Form-36 (SF-36) and standardized AAOS foot and ankle questionnaire, and the radiological evaluation with an osteoarthritis-score (OA-score).
Results:
Based on the pathoanatomy of the posteromedial malleolar fragment, all the fractures could be classified into two types. Using a combined operative approach, anatomical reduction and stable fixation was accomplished in all 12 patients. At a mean followup of 18.9 (range, 12 to 30) months, 10 patients achieved a good radiological result and satisfactory clinical recovery.
Conclusion:
This fracture pattern may be classified into two types with different injury mechanisms, which has not been described previously. After anatomic reduction and stable fixation through a combined operative approach, the short-term outcome was good.
INTRODUCTION
Trimalleolar fractures are a relatively common orthopaedic problem. The posterior malleolar fragment may result in articular surface incongruity and joint instability, and subsequently a worse outcome compared with bimalle-olar fractures. 11 The indications for anatomic reduction and internal fixation of the posterior malleolar fragment is still controversial. 15 While most studies have been focused on the size of the fragment, only a few studies mentioned about the shape of the posterior malleolar fragment.
Recently, a special type of trimalleolar fracture characterized by fracture of the entire posterior tibial plafond, including the posterior colliculus of medial malleolus has been described. 8 –10,16 Haragushi et al. has described it as “transverse medial-extension fractures” by computed tomography (CT) scan, and assumed it to be the result of supination-external rotation injury on the basis of the Lauge-Hansen classification system. 10 Weber et al. has described that there are usually two main posterior fragments with possible impaction of the fragment at the posteromedial plafond. 16 The injury mechanism has been thought to be vertical shearing with the foot in hyperflexion under a partial axial load, by which the fracture could not be classified in the Lauge-Hansen system. 9 Gardern et al. has reported seven cases fractured similarly except that axial impaction of the osteochondral fragments was scarce or absent. 8 As the creation of this fracture pattern required external rotation of the foot initially, the authors considered it as a special type of ankle fracture. Amorosa et al. has also reported on nine similar fractures, 1 which was felt to due to the combination of rotational force and axial load, but considered it to be a posterior pilon fracture, a unique pattern between a low-energy rotational ankle fracture and a high-energy axial loaded pilon fracture. So the mechanism of injury and the nomenclature of the fracture pattern are still indefinite.
The incidence of this type of fracture was reported to be only 6% to 8% of ankle fractures, 8,16 and it could be underestimated. 16 However, the operative techniques described were quite different for reduction of the posteromedial fragment. 2,16 Here we have reviewed a cohort of 12 patients with this special trimalleolar fracture type, refining the classification, proposing the mechanism of the injury, and present the operative techniques and short-term outcomes.
MATERIALS AND METHODS
From January 2007 to December 2009, 107 consecutive patients with ankle fractures were treated operatively by authors in the same institution. A retrospective review of those identified 12 patients who were trimalleolar fractures with involvement of the entire posterior tibial plafond. Six patients were injured by falling from an electric bicycle at a sudden stop, three patients by twisting injury upon falling from not less than one step height, two patients by a crush injury and one patient by ground-level fall. There were five men and seven women with a mean age of 47.1 (range, 22 to 66) years. Two patients had concurrent ipsilateral fracture of a patella or rib, respectively. Four patients underwent surgery at 2 to 3 days, and seven patients underwent surgery at 6 to 10 days when the soft tissue swelling subsided. The mean time from injury to operation was 5.6 (range, 2 to 10) days. In the emergency department, if there was a fracture-dislocation, closed reduction and splinting or calcaneal traction was performed before further assessment by CT scan.
Operative technique
The operative technique was similar to what had been described previously. 16 Patients were placed prone on a radiolucent table, with a bolster under the distal lower leg to facilitate the talus being reduced. A pneumatic tourniquet was routinely used on the ipsilateral thigh. A standard posterolateral approach was used initially, through the interval between the peroneals and the flexor hallucis longus, and the posterolateral and the posteromedial fragments were both identified. First, impacted osteochondral fragments on the posteromedial corner were elevated directly under fluoroscopic control, then all the marginal fragments of the posterior tibial plafond were anatomically reduced and fixed temporarily by Kirschner wire. A standard posteromedial approach was performed subsequently, not only for the fixation of the medial malleolus, but also for confirmation of anatomic reduction of the posteromedial fragment at its medial edge. Finally, the lateral malleolar fracture was reduced and fixed by plating. Syndesmosis stability was checked by Cotton test, and a syndesmosis screw was used routinely if it was associated with Tilluax-Chaput fracture.
The operative technique varied in some cases. Without osteochondral impaction of the posteromedial corner, the posterolateral fragment could be reduced and fixed, and fibular plating on the lateral side could be performed subsequently. Finally, a standard posteromedial approach was performed to accomplish the reduction and fixation of the posteromedial fragment.
Postoperative care
Postoperatively, the patients were placed in a plaster splint or an orthosis for 4 to 6 weeks. After the first 3 weeks, range of motion exercises were started in reliable patients. Partial weightbearing was allowed after 6 weeks, then clinical assessment of fracture-healing was made when no pain or tenderness with weightbearing or walking, or local or axial percussion. Full weightbearing was restricted for about 3 months postoperatively. Clinical and radiological followup was performed in all patients for at least one year, and any complication was recorded.
The Short Form-36 (SF-36) and standardized AAOS foot and ankle questionnaire were used to assess the clinical outcomes. The SF-36 measures eight health domains using eight scales assessing physical function (PF), role limitation due to physical problems (RP), bodily pain (BP), general health (GH), vitality (VT), social function (SF), role limitation due to emotional problems (RE), and mental health (MH), which may be summarized into physical component summery (PCS) and mental component summery (MCS). The AAOS Foot and Ankle Questionnaire has 20 items or questions that combined form the Foot and Ankle Core Scale and another five questions that form the Shoe Comfort Scale.
An osteoarthritis-score (OA-score) was additionally used to determine degenerative changes of the ankle joint radi-ologically at about 1-year followup. 4 A score of 0 was a normal joint; a score of 1 was assigned to the presence of osteophytes without joint space narrowing; a score of 2 was assigned to joint space narrowing with or without osteo-phytes; and a score of 3 was assigned with sub or total disappearance or deformation of the joint space.
RESULTS
All the patients had the entire posterior tibial plafond fractured into two main posterior fragments. Based on the pathologic anatomy of the posteromedial malleolar fragment, all these fractures could be classified into two types. Type 1 was present in five patients with AO-type C fibular fracture, while on the posteromedial side, the fracture separating the posterior colliculus of the medial malleolus from the anterior colliculus (Figure 1). On anteroposterior radiographic view, a double contour sign could be seen above the medial malleolus. 16 Type 2 was presented in seven patients with AO-type B fibular fracture, the whole medial malleolus was fractured and connected with the posteromedial fragment (Figure 2). The average area of the posterior malleolar fragment comprised 26% of the cross-sectional area of the tibial plafond for Type I fractures and 34.4% of the cross-sectional area for Type II fractures. There was one dislocation and three subluxations in all seven Type 1 fractures, while three dislocations and one subluxation in all five Type 2 fractures. The occurrence of ankle joint dislocation or subluxation in Type 1 and Type 2 was 57.1% and 80%, respectively. Osteochondral impaction occurred only in one fracture-dislocation with Type 1 and two fracture-dislocations with Type 2. Patients' data are summarized in Table 1.

Patient No. 4, a 49-year-old woman with a hyperplantarflexion trimalleolar fracture of Type 1 from a ground-level fall.

Patient No. 9, a 60-year-old man with a hyperplanterflextion trimalleolar fracture of Type 2 from an electric bicycle accident.
Patient Data
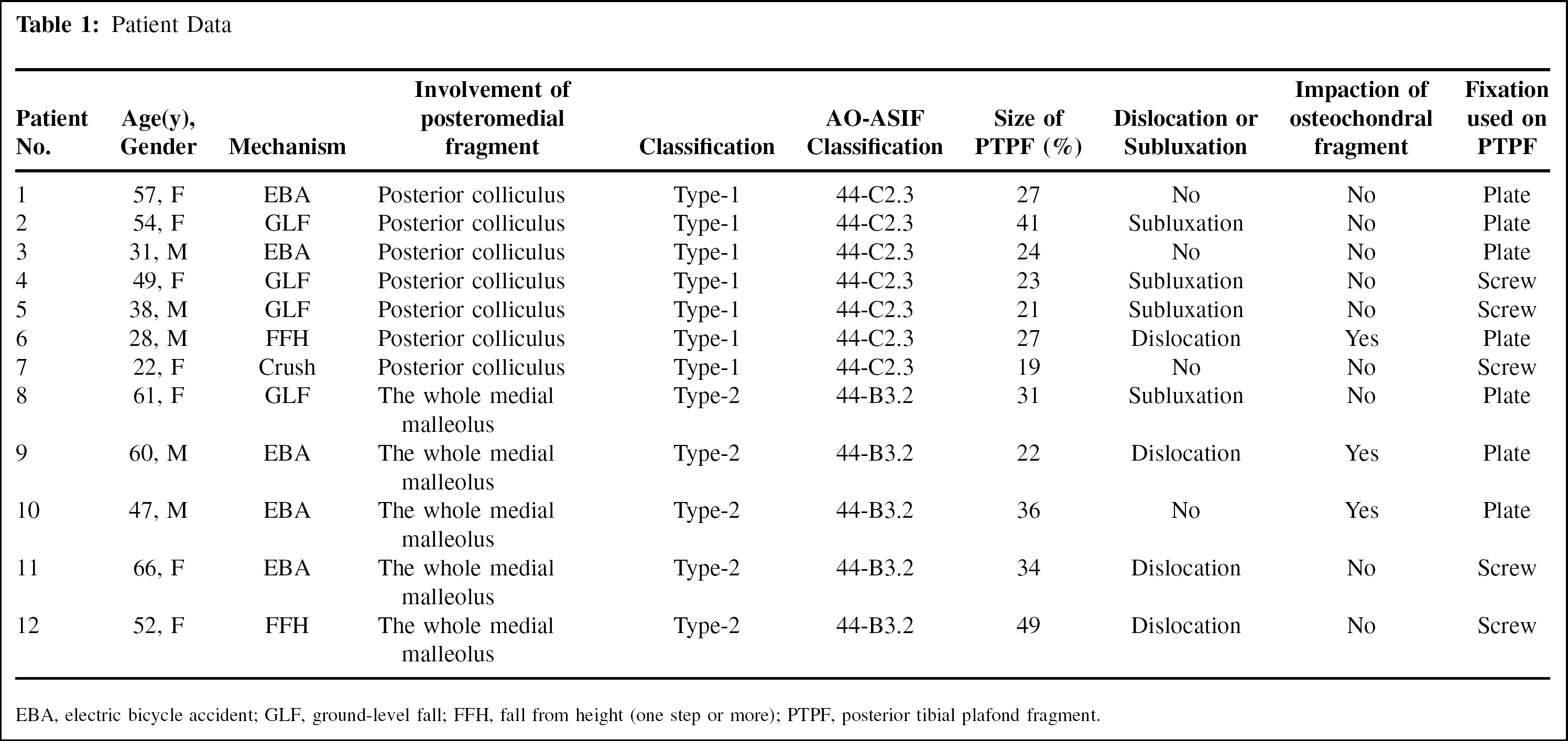
EBA, electric bicycle accident; GLF, ground-level fall; FFH, fall from height (one step or more); PTPF, posterior tibial plafond fragment.
A combined operative approach (posteromedial and posterolateral) was used in all patients (Figure 3), and all the trimalleolar fractures were anatomically reduced under fluo-roscopic control intraoperatively. Buttress plates were used on the posterior tibial side in four patients, and absorbable screws were used additionally for the syndesmosis in two patients when the Chaput tubercle fractured. Because the posterior tibial tendon runs directly over the main part of the posteromedial fragment, space for placement of hardware was limited so we preferred multiple cannulated screws with screw heads countersunk (Figure 4) rather than buttress-plate fixation (Figure 5) unless there was a multi-fragment fracture or osteochondral impaction on the posteromedial corner of the tibial plafond.
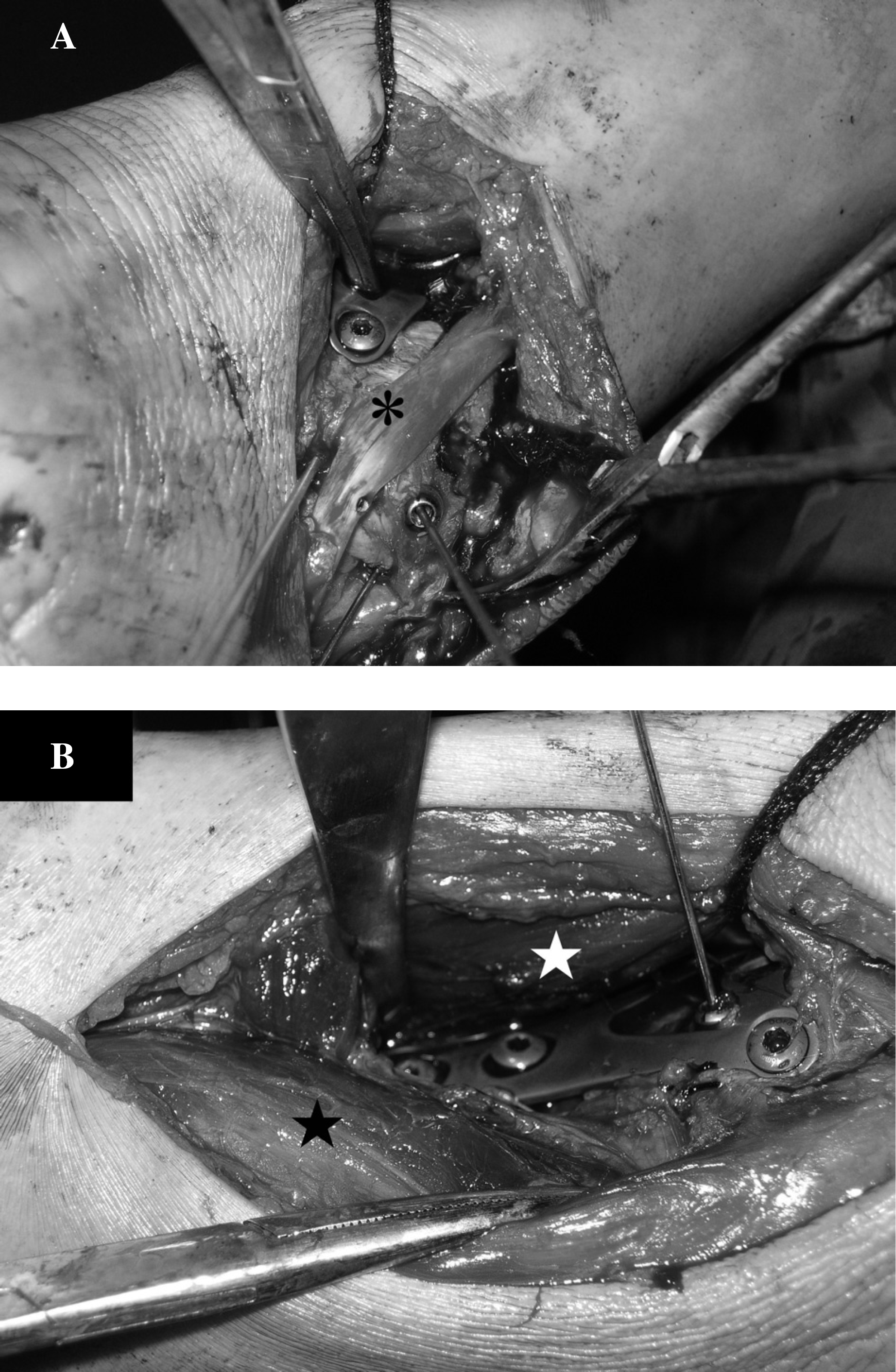
A combined approach was used in this Type 2 fracture.
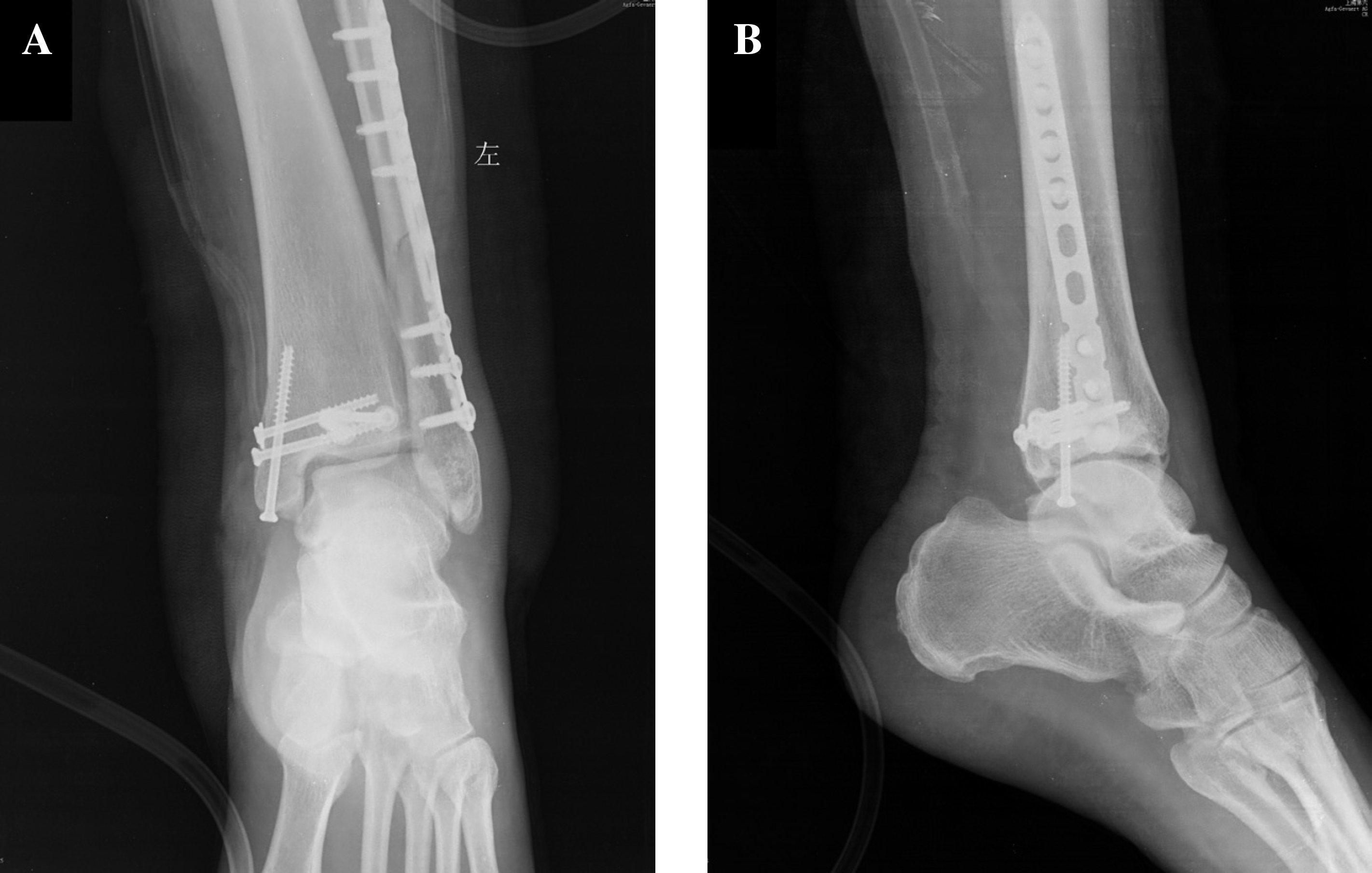
AP (A) and lateral (B) radiographs after open reduction and internal fixation. Because of the limitation of the space for plating on the posteromedial fragment, we preferred cannulated screws with the screw head countersunk.
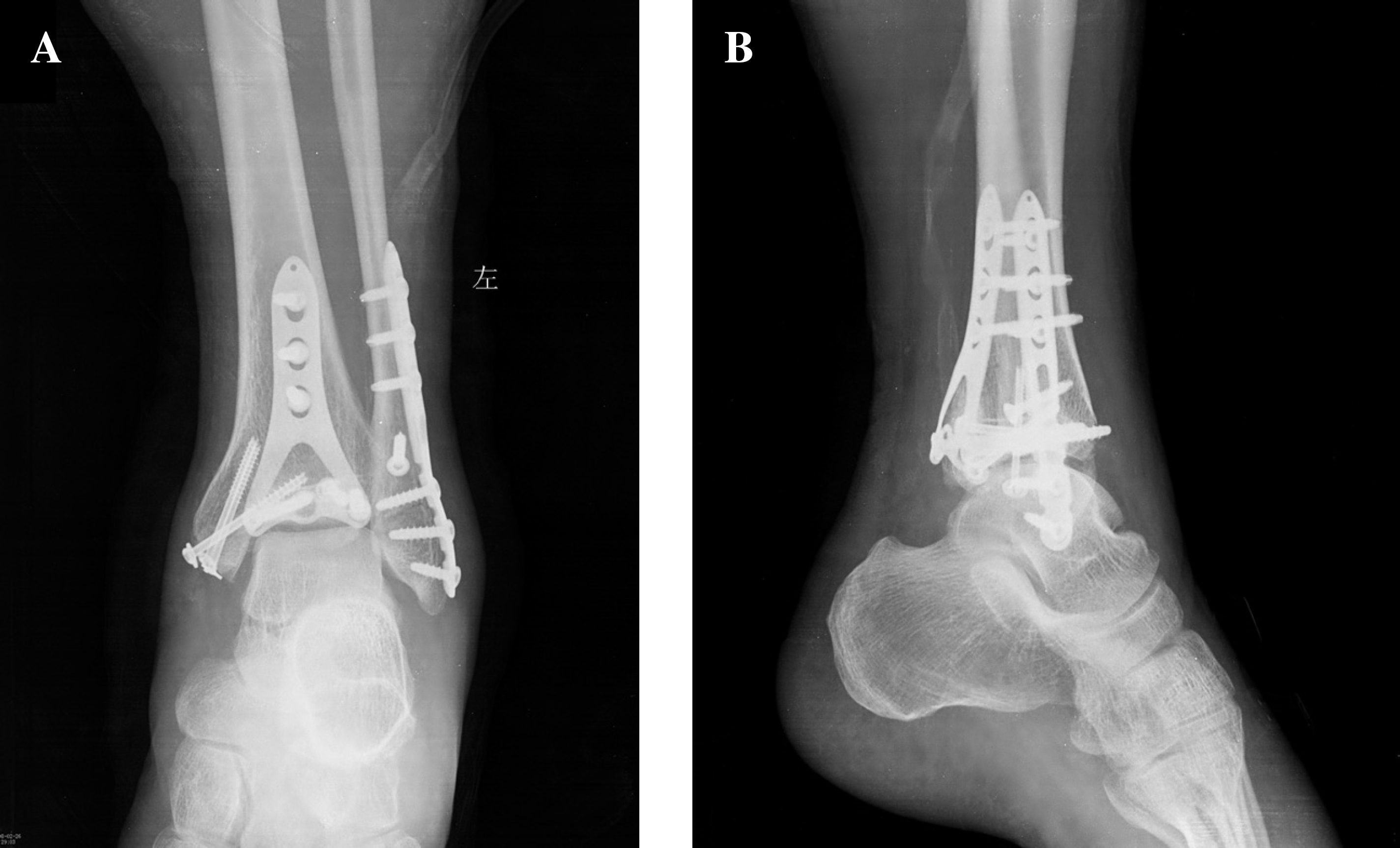
AP (A) and lateral (B) radiographs after open reduction and internal fixation. Congruency of the ankle joint was restored and buttress-plating was used to support the impacted articular surface.
Ten of 12 patients were available for followup at the average of 18.9 (range, 12 to 30) months. Both the posteromedial and posterolateral incisions healed uneventfully, and all fractures were healed by 6 to 8 weeks, without any loss of reduction of fragments or the position of the talus in the mortise. All patients returned to work in four to six months, except one patient had a stiff ankle and felt pain on walking which we attributed to poor compliance with rehabilitation. One patient complained of discomfort over the lateral plate on the fibula until the hardware was removed. Another patient had the posteromedial screws removed due to the local irritation on extensor digitorum longus. No infections or other complications occurred.
At about 1 year postoperatively, the mean OA-score was 0.8 in all 10 patients, while it was 0.7 in patients of Type 1 and 1.0 in those of Type 2. At the end of the followup, the mean score of PCS and MCS in SF-36 are 45.3 and 46.9 in all patients, while it is 46.6 in both subscales of Type 1 patients and 43.5, 47.4 in Type 2 patients, respectively. The mean score of AAOS foot and ankle core scale was 85.7 in all patients, while it was 86.1 in patients of Type 1 and 85.2 in those of Type 2 (Table 2).
Clinical and Radiological Outcomes on Followup
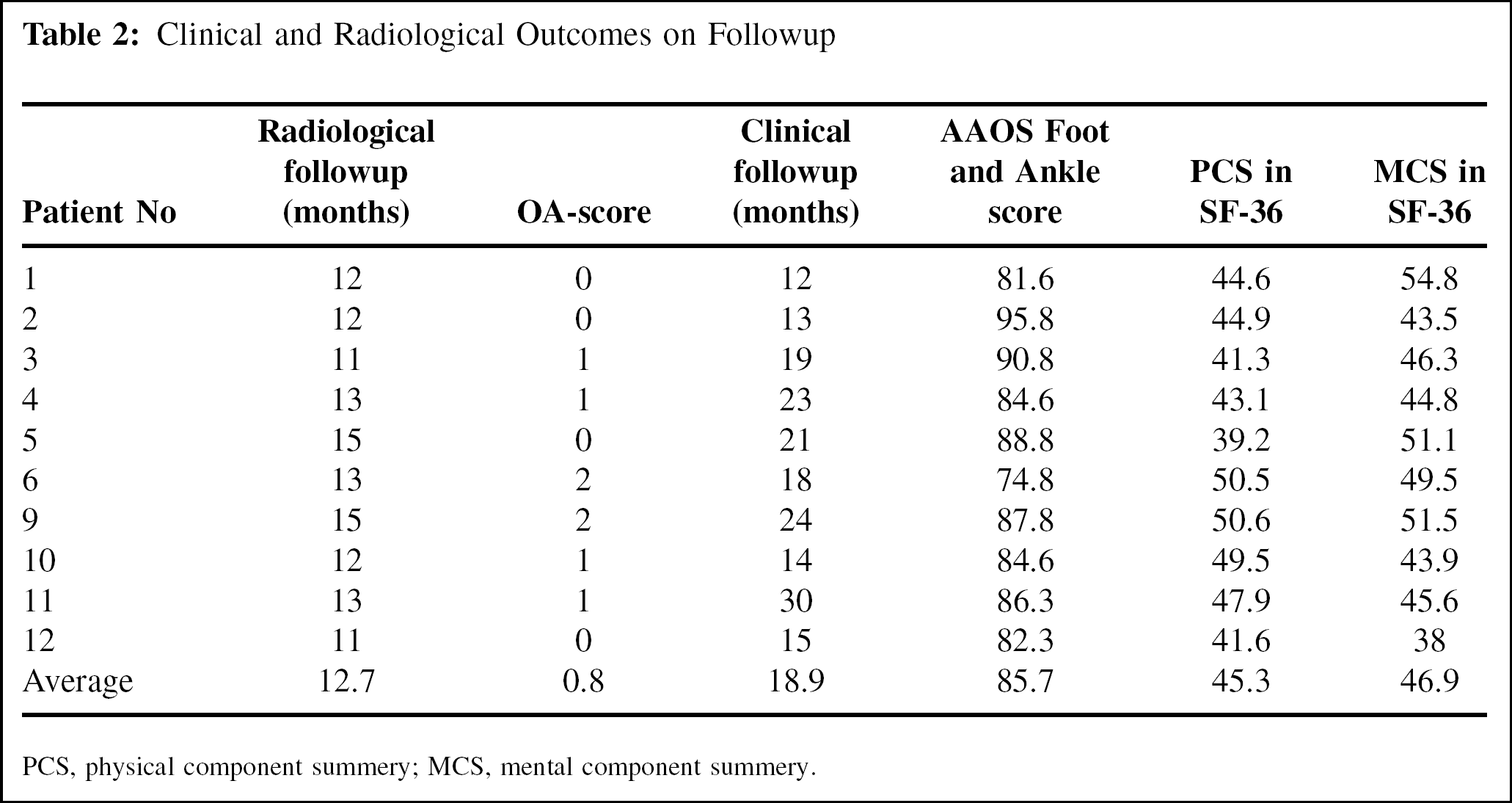
PCS, physical component summery; MCS, mental component summery.
DISCUSSION
The characteristic of this cohort was the fracture of entire posterior tibial plafond, producing a posterolateral fragment and a posteromedial fragment. It had been reported to have an incidence of about 6% to 8% of ankle fractures undergoing surgical treatment, 8,16 or 19% of ankle fractures with a posterior malleolar fragment. 10 Of 107 consecutive patients with an ankle fracture at our institution, 12 patients had this special pattern, suggesting a relative frequency of about 11%.
We do not feel this type of fracture should be included in the Lauge-Hansen classification system. 8,16 Based on the fracture extension of the posteromedial malleolar fragment, we classified it further into two types. Type 1 is the same pattern as those reported previously, which included a high spiral fracture of the fibula, vertical shear fracture of the posterior colliculus from the medial malleolus, and posterolateral malleolar fracture. 8,9,16 In this series, we found the patients with such a fracture type were relatively low-energy injuries, and mostly without osteochondral impaction on the posteromedial corner of the tibial plafond. Gardner et al. had reported 7 cases of ankle fracture with posteromedial malleolar fragment, 8 three of which had a Weber C fibular fracture. Osteochondral impaction was seen only in one case, which was similar to our Type 1 fractures. So the mechanism of injury for this fracture pattern required external rotation of the foot initially, to position the posterior talar body posteromedially under the mortise, followed by forced plantarflexion of the foot to produce a vertical shear fracture of the posteromedial tibia plafond. 8 Type 2 had not been previously described with the fracture line of the posterome-dial fragment in the transverse plane anteriorly and in the coronal plane posteriorly. Therefore, the posteromedial part of the tibial plafond and the whole medial malleolus are in one piece. We propose the mechanism of Type 2 fracture is that the foot is externally rotated in a pronated position initially, producing the avulsion of the entire medial malleolus first, then a sudden instability in external rotation leads to a vertical shear fracture posteromedially and an oblique fibular fracture of AO-type B, with osteochondral impaction of the talar body. The occurrence of dislocation or sublux-ation of the ankle joint and osteochondral impaction of the tibial plafond in Type 2 were higher than those in Type 1, which implied a higher energy injury.
Although AOFAS scoring system is widely used for the measurement of clinical outcome, it has been found recently to have poor construct validity. 13 The combination of Short Form-36 (SF-36) and standardized AAOS foot and ankle questionnaire has been recommended to measure outcomes in orthopaedic patients with lower-limb conditions comprehensively and efficiently. 12 The mean AAOS foot and ankle score and SF-36 score in physical component summary scale were both higher in Type 1 than in Type 2, while the OA-score showed less degenerative changes of the ankle joint in Type 1 than in Type 2. We consider it the result of the relatively high-energy injury and complex mechanism in Type 2 fracture, which is supported by a previous long-term study that fracture-dislocation of the ankle joint was associated with a larger posterior malleolar fragment which resulted in worse outcomes than nondislocation. 4
The most popular theory on the cause of post-traumatic arthritis is that the articular incongruity will reduce the tibio-talar contact area and increase contact stress. But recently, Fitzpatrick et al. had found in a biomechanical experiment of a trimalleolar fracture model that the contact stress had shifted onto the articular cartilage which was not accustomed to bearing stress. 6 Van den Bekerom et al. suggested that it was more important to restore the medial and lateral constraints of the ankle than to restore the anatomic congruity. 15 Recently, Stufkens et al. 14 reported that only 79.3% of the optimally reduced fractures show good to excellent long-term outcomes. The remainder might have developed joint degeneration because of other factors, just like the initial cartilage lesions, hindfoot alignment, etc. In this series, we had anatomically reduced the medial and lateral malleolar fracture in all cases, and restored the articular congruity by elevating the impacted articular cartilage on the posteromedial corner in three cases. Moreover, the syndesmotic stability was further confirmed by Cotton test during the operation. Postoperatively, all the patients except one were satisfied and went back to work within half a year. At one-year followup, the mean OA-score was 0.8, most of patients showed congruent ankle joints with no obvious degenerative changes.
Different operative techniques have been reported for reducing the impacted osteochondral fragment of the posteromedial corner of the tibial plafond. Amorosa et al. performed a posterior arthrotomy through the posteromedial approach. 1 Using a universal distractor to further facilitate the exposure, the marginal impaction might be reduced directly, but the centrally located osteochondral impaction was still difficult to visualize and directly reduce. Through the posteromedial approach, Bios et al. also suggested that the medial malleolus may be reflected distally to expose the tibiotalar articulation and permit direct reduction of the joint surface. 2 But in Weber's opinion, 16 the turnover of the posteromedial fragment through a posteromedial approach, may carry the talus posteriorly with the deep part of the deltoid ligament, therefore hindering the reduction of the impacted osteochon-dral fragments. The technique we used here is the same as that described previously. 16 Through the posterolateral approach instead of posteromedial approach, the osteochon-dral impaction in one patient of Type 1 and two patients of Type 2 were anatomically reduced.
The posterolateral approach is commonly used on displaced posterior malleolar fractures. It provides good exposure and visualization of the fragment, which may lead to few complications and good clinical outcomes. 7 Meanwhile, the lateral malleolar fracture can be reduced and fixed through the same incision. If the fracture extends to the posteromedial tibial plafond, a posteromedial approach may satisfy the direct exposure and stable fixation of the displaced fragment instead. 2 Here we report a combined approach (posterolateral and posteromedial), through which the exposure of the entire posterior distal tibial plafond after the flexor digitorum longus and the neurovascular bundle were retracted posteriorly. The blood supply of the Achilles tendon and soft tissue between the two incisions was preserved. 3,5
The study however has some limitations. First, the incidence of this special type of trimalleolar fracture is low so sample limitation is inevitable. We believe both of the two types occurred in hyperplantarflexion, but a further biome-chanical experiment in a cadaveric model is necessary to verify it. Using the operative technique we described above, the short-term outcomes of this series was satisfactory.