
Abstract
Background:
We compared forefoot and calcaneocuboid pressure in isolated medial column fusion (1-3 tarsometatarsal fusion) versus medial and lateral column fusion (1-5 tarsometatarsal fusion) in a neutral, inversion, and eversion loading model in stance gait phase.
Methods:
Twelve fresh-frozen cadaveric specimens were cyclically loaded to 720 N at 0.5 Hz for 30 cycles. Plantar and calcaneocuboid joint pressures were measured in neutral, inversion, and eversion in the intact foot, with isolated medial column fusion, and with medial and lateral column fusion.
Results:
Lateral pressure was higher in the medial and lateral column fusion group than isolated medial column fusion and intact in neutral (55.8 ± 14.8 versus 46.2 ± 13.6 and 45.5 ± 14.8 kPa, respectively) and eversion (80.7 ± 18.4 versus 61.8 ± 13.7 and 60.2 ± 18.2 kPa, respectively) (p ≤ 0.001). Calcaneocuboid pressure was higher in medial and lateral column fusion than isolated medial column fusion and intact in neutral (1436.7 ± 210.6 versus 1073.7 ± 282.5 and 1084.9 ± 337.6, respectively; p = 0.001) and inversion (1518.3 ± 270.5 versus 1310.5 ± 298.8 and 1237.1 ± 401.9, respectively; p = 0.02). Using combined position data, calcaneocuboid pressure was significantly higher in the medial and lateral column group than in both other groups. The isolated medial column fusion group did not differ significantly from the intact group in any measurement.
Conclusion:
Medial and lateral column fusion significantly increased lateral and calcaneocuboid pressures with loading compared with isolated medial column fusion and the intact state. No difference was observed between isolated medial column fusion and the intact state.
Clinical Relevance:
It may be advisable to avoid fusing the lateral column in tarsometatarsal arthrodesis if possible to avoid pressure increase in the forefoot and hindfoot.
INTRODUCTION
Fusion of the first, second, and third tarsometatarsal (TMT) joints, or medial column, has been an effective treatment for painful degenerative arthritis, post-traumatic arthritis, and Charcot arthropathy at these joints. In the setting of arthritis in all five TMT joints, there are conflicting data on whether to perform an isolated medial column fusion or also to fuse the lateral column, which includes the fourth and fifth TMT joints. Some studies recommend against lateral column fusion, citing subsequent metatarsalgia, unacceptable stiffness, and difficulty obtaining fusion. 3,6,7,9,12 Others consider it acceptable to fuse both the medial and the lateral column in the setting of painful arthritis or deformity. 10,11 While it is generally accepted that maintaining motion at the fourth and fifth TMT joints is preferable, the alternatives to fusion of these joints have shown limited success2 and medial and lateral fusion is indicated in significant deformity or arthritic pain in the lateral column. The biomechanical effect of medial and lateral fusion has not been investigated.
The fourth and fifth TMT joints have more motion in the sagittal plane than the other TMT joints,13 and they play a key role in accommodating to uneven surfaces. Fusion of the lateral column results in a stiffer foot8 that may be less able to adjust to uneven surfaces. It seems reasonable to assume that difficulty navigating uneven surfaces would be greater in patients with medial and lateral column fusion versus isolated medial column fusion. It could be helpful to compare midfoot plantar pressure and calcaneocuboid pressure in the two fusion scenarios using a model that simulates uneven surfaces and results in inversion and eversion of the foot.
We compared medial and lateral forefoot pressure and calcaneocuboid pressure in stance phase of gait in the intact foot, with isolated medial column fusion, and with medial and lateral fusion in a neutral, eversion, and inversion loading model. We hypothesized that medial and lateral column fusion would be associated with significantly altered forefoot and calcaneocuboid joint pressures compared with isolated medial column fusion and the intact foot and that pressures in the medial column fusion group would not differ significantly from pressures in the intact foot.
MATERIALS AND METHODS
Twelve fresh frozen cadaveric lower extremities were stored at −20°C and thawed to room temperature before testing. Mean age of the specimens was 73.3 (range, 43 to 97) years, and there were six male and six female specimens. The tibia and fibula were transected approximately 30 cm above the plantar aspect of the heel. Standard exposure over the first interspace was used to expose the first and second TMT joints. Access to the third TMT joint and the fourth TMT joint was gained through a second incision between the third and fourth TMT joints. A third incision was made just plantar to the lateral aspect of the proximal fifth metatarsal to allow for placement of the fifth TMT screws.
Fusion fixation was done with 4.5-mm fully threaded cannulated screws (Synthes, Inc., West Chester, PA). For isolated medial column fusion, five screws were placed. The first screw was placed across the dorsal first metatarsal to the plantar medial cuneiform. The second screw was placed across the dorsal medial cuneiform to the plantar first metatarsal. The third was placed across the medial cuneiform to the second metatarsal, and the fourth was placed across the second metatarsal into the middle cuneiform. The fifth screw was placed across the third metatarsal into the lateral cuneiform. Medial and lateral column fusion included those five screws plus a sixth screw placed across the fourth metatarsal into the cuboid. Screws 7 and 8 were placed in an axial direction from the fifth metatarsal into the cuboid. For these screws, the starting point was on the lateral apex of the triangle-shaped fifth metatarsal to obtain optimal fixation of the fifth metatarsal to the cuboid (Figure 1). The foot was in anatomic position for fusion of fourth and fifth metatarsals.
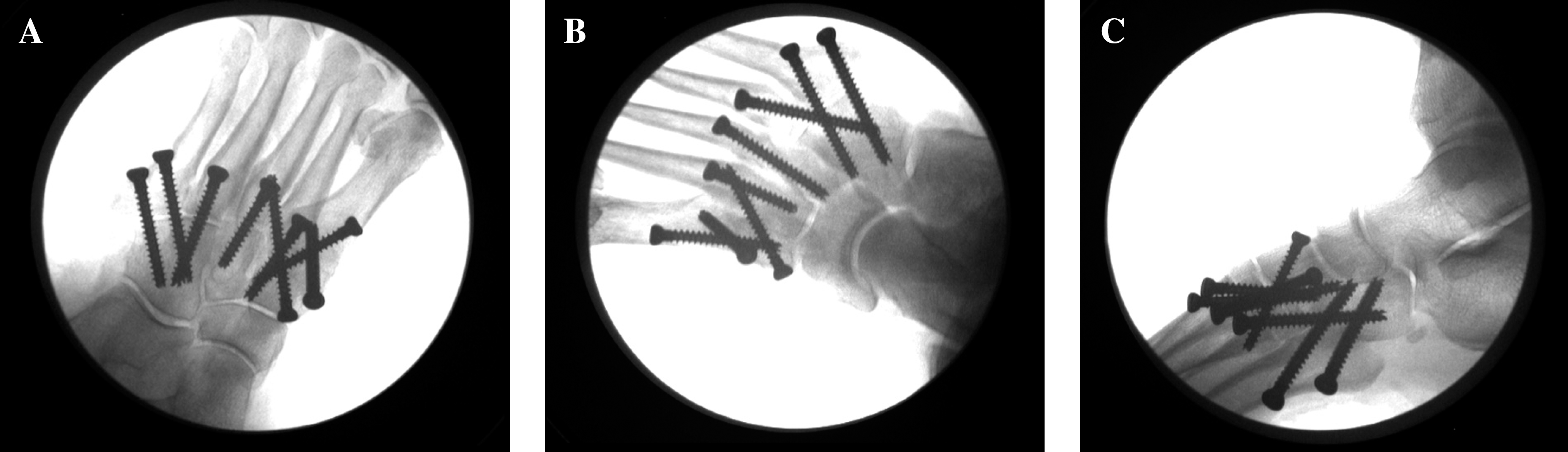
Radiographs show oblique (A), AP (B), and lateral (C) view of medial and lateral column TMT arthrodesis.
Initial measurements with loading were obtained with medial and lateral column fusion on a neutral (flat) surface (Figure 2) and using a 15-degree wedge to simulate eversion and inversion (Figure 3). Next, the screws securing the fourth and fifth metatarsal were removed to simulate isolated medial column fusion and loading was repeated. Finally, all screws were removed and loading was repeated to provide intact data. This order was used to avoid taking the specimen off the loading device between testing phases.

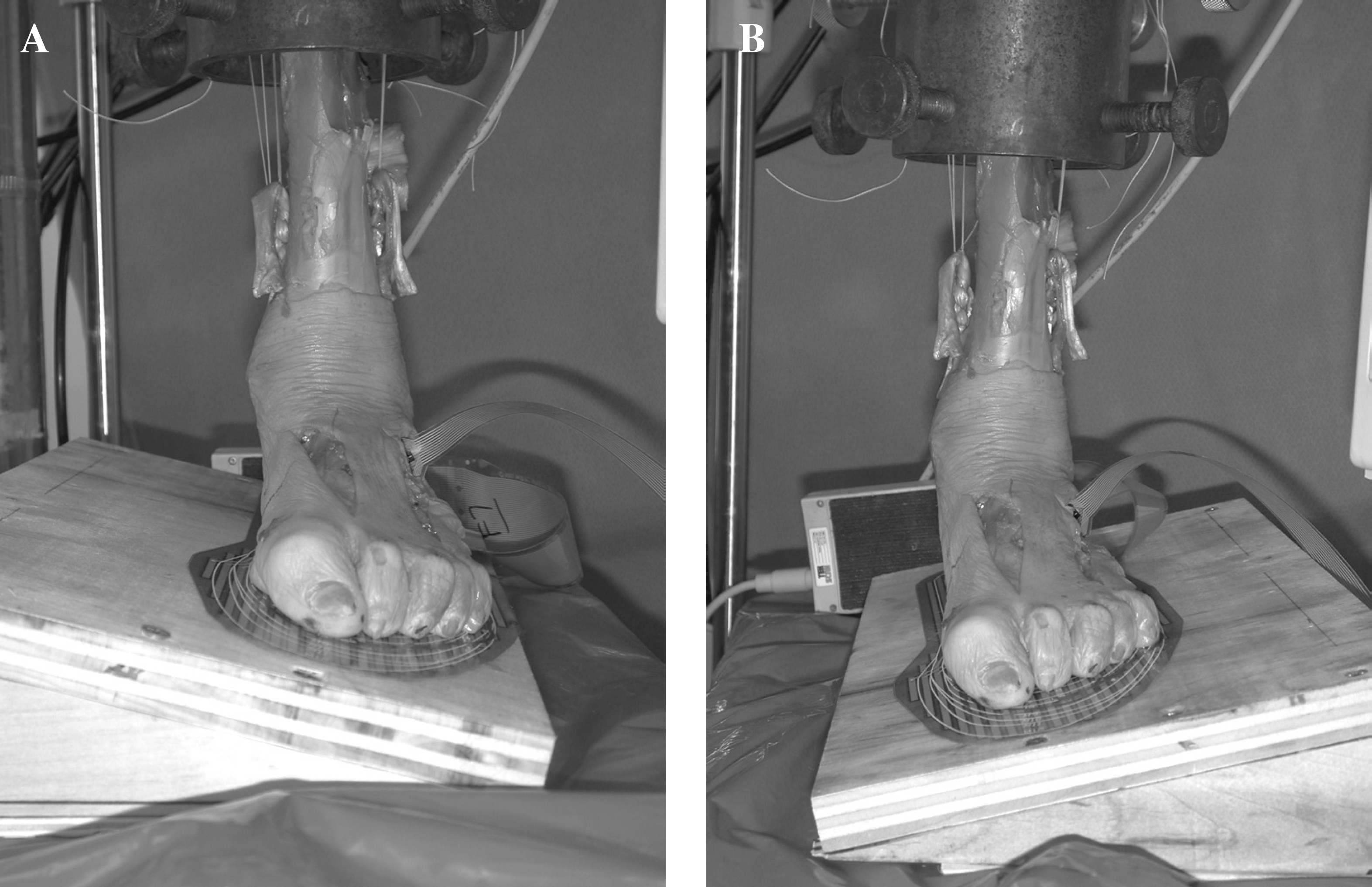
Photograph shows placement of specimen in load frame with tendons sutured for loading with simulated muscle forces.
Photograph shows platform used for simulated inversion (A) and eversion (B).
After screw fixation, the specimens were mounted onto a holding device to maintain consistent vertical alignment during testing. Holes in the top of the device allowed passage of cables connecting tendons to pneumatic actuators. The device was attached to a Mini Bionix load frame (MTS Systems Corporation, Eden Prairie, MN) (Figure 3). The posterior tibialis, flexor digitorum longus, flexor hallucis longus, peroneus longus and brevis, and Achilles tendons were stripped of muscle and sutured using a Roman sandal technique with braided 65-lb test (290 N) Stealth fishing line (Spiderwire, Spirit Lake, IA). The peroneus longus and peroneus brevis were sutured and loaded as one unit. Each specimen was examined in a quasi-dynamic state simulating two-legged stance using axial compression of 720 N with the addition of simulated muscle forces: Achilles, 400 N; posterior tibial tendon, 40 N; flexor digitorum longus, 20 N; flexor hallucis longus, 20 N; and peroneus longus/brevis, 80 N.15
For each measurement an external 72 N to 720 N straight axial force was applied cyclically at 0.5 Hz for 30 cycles while the muscle forces were kept constant. The base plate was fixed, and the foot was in neutral position. Forefoot medial and lateral plantar pressure measurements were obtained using the F-Scan computerized pressure measurement system (Tekscan, Inc., South Boston, MA). The sensor pad has a spatial resolution of four sensels per square centimeter. Calcaneocuboid joint pressures were obtained with the 6900 I-scan sensor (Tekscan). The I-Scan sensor areas are 14 mm × 14 mm with a sensel density of 62 sensels per square centimeter. These pressure measurements were obtained for all three surfaces (neutral, everted, and inverted) and all three constructs (medial and lateral column fusion, isolated medial column fusion, and intact). Three hundred scans were captured on both the F-scan and I-Scan measuring devices, and the peak pressures were averaged by the software. A new F-Scan and 6900 sensor pad was used for each specimen. Sensors were kept in place on each specimen throughout testing.
F-scan sensors were calibrated with each medial and lateral column fusion specimen in the MTS loading frame using a force and time duration like that used in testing. I-scan sensors were calibrated using a known load between two high-density polyurethane plates. We confirmed the calibration by confirming that the load measured by the pressure sensors during testing was within 8% of the applied load.4 A similar calibration method has been reported previously with Tekscan software in a study of patellofemoral contact pressure across the trochlear surface.1 The inferior portion of the extensor digitorum brevis and dorsal portion of the lateral calcaneocuboid ligament were transected to slide the sensor into the joint. Only one of the four available 6900 sensor pads was used due to the small surface area of the calcaneocuboid joint. Average peak pressures were determined for the calcaneocuboid joint.
Three replicates were conducted on one specimen to determine whether the pressure measurements were repeatable and whether order of the procedures had an effect on the pressure measurements. Initial measurements were done with no fixation, and measurements were repeated after all five metatarsals (both columns) were locked. The lateral column was then unlocked and measurements taken, and finally all hardware was removed and a last pressure measurement was taken. This was repeated three times. The specimen was cycled 30 cycles in between each replicate. The coefficients of variation for the initial and locked-unlocked conditions were 0.06 and 0.04, respectively, and the coefficient of correlation between the initial and locked-unlocked conditions was 0.945.
Power analysis showed that nine specimens in each group would give 90% power to detect a difference if it existed at an alpha level of p = 0.05. Pressure comparisons were done using one-way analysis of variance. A Scheffe post hoc test was used if analysis of variance showed a significant difference. A p level of ≤0.05 was considered significant.
RESULTS
Using the 15-degree wedge in the intact foot, medial pressure in inversion was significantly higher than in neutral and eversion (Table 1). Lateral pressure in the intact foot was significantly higher in eversion than in inversion. We did not observe differences in calcaneocuboid pressure in eversion or inversion compared with neutral in the intact group.
Medial and Lateral Forefoot and Calcaneocuboid Joint Pressure in Neutral, Eversion, and Inversion
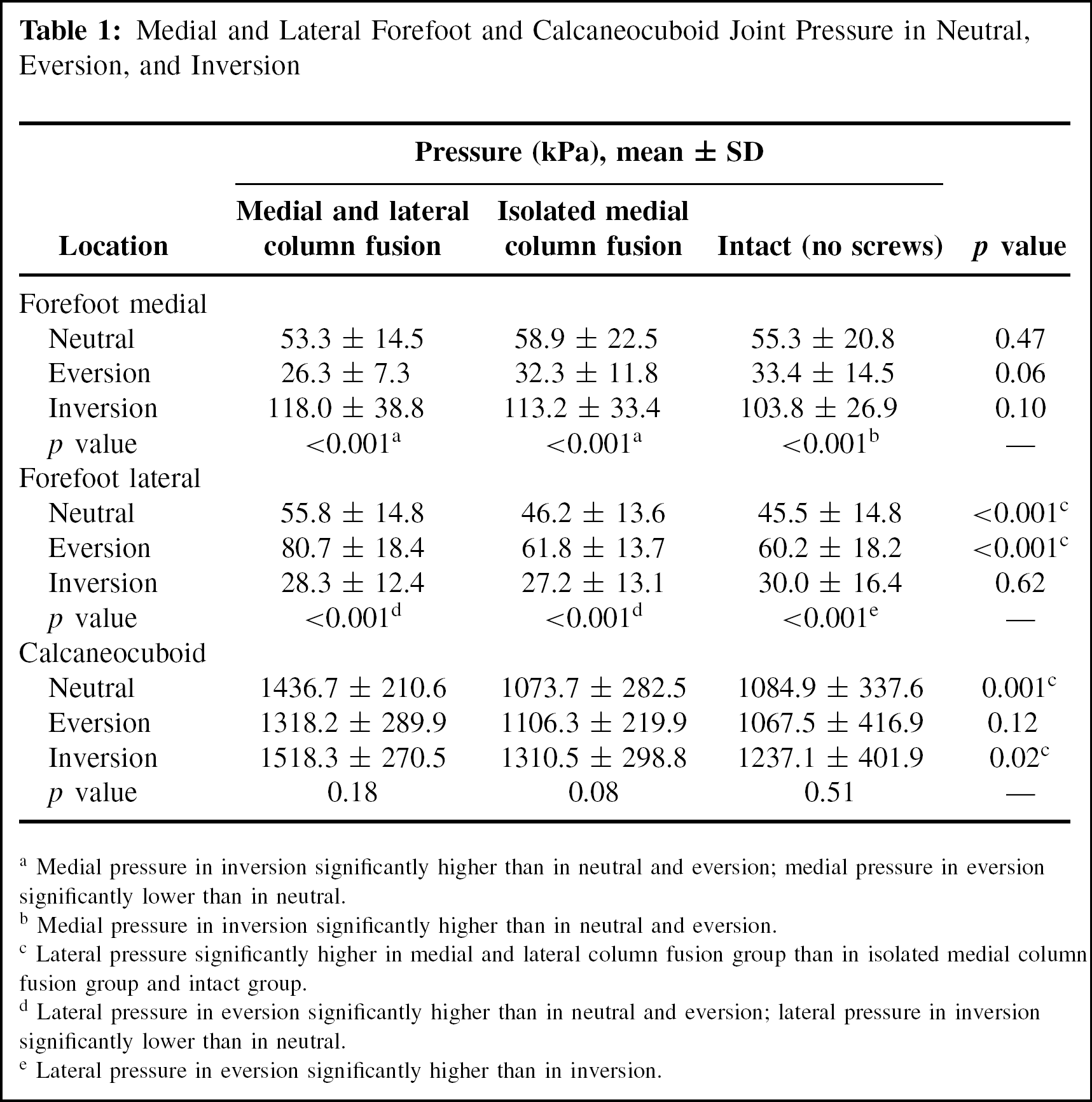
Medial pressure in inversion significantly higher than in neutral and eversion; medial pressure in eversion significantly lower than in neutral.
Medial pressure in inversion significantly higher than in neutral and eversion.
Lateral pressure significantly higher in medial and lateral column fusion group than in isolated medial column fusion group and intact group.
Lateral pressure in eversion significantly higher than in neutral and eversion; lateral pressure in inversion significantly lower than in neutral.
Lateral pressure in eversion significantly higher than in inversion.
Lateral pressure in neutral and eversion was significantly higher in the medial and lateral column fusion group than in the isolated medial column fusion group and the intact group, and calcaneocuboid pressure was significantly higher in the medial and lateral column fusion group than in both other groups in neutral and inversion (Table 1). No differences were observed in medial pressure with inversion between the medial and lateral column fusion group and the other groups. No significant differences in forefoot or calcaneocuboid pressure were observed between the isolated medial column fusion group and the intact foot.
When neutral, inversion, and eversion data were combined to obtain an approximation of effect of range of foot position in stance position of normal gait, calcaneocuboid pressure was significantly higher in the medial and lateral column fusion group than in the other two groups (Table 2). There were no differences between the groups in medial or lateral pressure.
Pressure Comparisons With Combined Neutral, Eversion, and Inversion Pressure Data
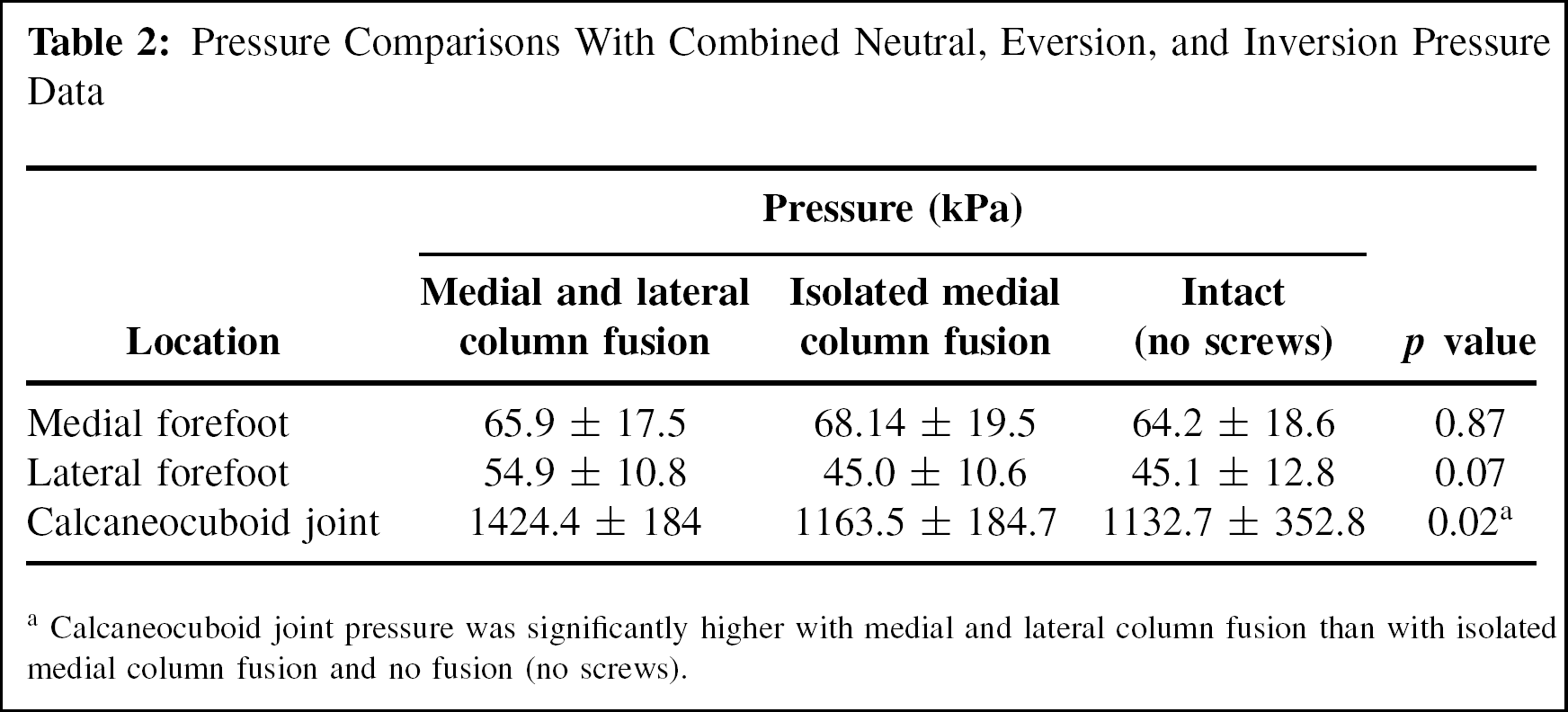
Calcaneocuboid joint pressure was significantly higher with medial and lateral column fusion than with isolated medial column fusion and no fusion (no screws).
DISCUSSION
In this inversion/eversion model, we observed significant change in medial and lateral forefoot pressure with foot position change with eversion and inversion of the intact foot. When compared with a neutral (flat) platform, the medial wedge (inversion model) demonstrated increased medial forefoot pressure and decreased lateral forefoot pressure and the lateral wedge (eversion model) demonstrated decreased medial forefoot pressure and increased lateral forefoot pressure. The significant differences in forefoot pressures allowed a preliminary examination of the effect of eversion and inversion on these pressures in the different treatment groups.
The isolated medial column fusion group did not differ significantly from the intact group in any comparison measured, but the medial and lateral column fusion group had significantly higher lateral forefoot pressure in eversion and neutral compared to the other two groups. The medial and lateral column fusion group also had significantly higher calcaneocuboid pressure than the other groups in neutral and inversion. These findings suggest that fusion of all five TMT joints results in altered foot biomechanics, whereas isolated medial column fusion is not associated with substantial change compared with the intact state. When data for foot positions was summed, calcaneocuboid pressure was higher in the medial and lateral column fusion group than both other groups, whereas no significant differences were observed in forefoot pressure. This finding suggests that on uneven surfaces or when foot position is altered from neutral, the calcaneocuboid joint may be more affected than the forefoot joints. Although the significant differences identified in this study may not represent important clinical differences in that pressure varied between groups by only 10% to 15% in some cases, these biomechanical results could indicate the potential for increased stress reaction at the fifth metatarsal and/or fifth TMT symptoms with medial and lateral column fusion. The higher calcaneocuboid pressure found with medial and lateral column fusion suggest potential for additional stress on the calcaneocuboid joint with fusion of the fourth and fifth TMT.
Outcomes in patients receiving medial and lateral column TMT fusion have not been studied definitively. In a study of 32 patients receiving TMT fusion, Komenda et al.6 reported that two patients who underwent fusion of all five TMT joints required subsequent osteotomies to alleviate metatarsalgia. These authors recommended against fusion of the fourth and fifth TMT, stating that they believed arthritis in the fourth and fifth TMT joints is well tolerated and that motion at the fourth and fifth TMT is important for optimal function. One series of 16 patients with TMT fusions, four with fusion of all five joints, found no difference in clinical outcome.12 Raikin and Schon10 reported good results including fusion of the fourth and fifth TMT in patients with pain at those joints, 22 with neuroarthropathic rockerbottom deformity and six with painful arthritis involving the lateral joints. In 20 patients with severe post-traumatic arthritis in the fourth and fifth TMT joint, Rammelt et al.11 reported no difference in outcome between patients treated by isolated medial column TMT fusion and those with medial and lateral column TMT joints. These small studies report improvement in patient satisfaction after surgery, but it is not known whether specific aspects of complete fusion of the TMT joints, such as difficulty with uneven surfaces, remain a concern after surgery. It seems reasonable to assume that fusion of all TMT joints can be managed well clinically, but the current biomechanical results suggest that excluding the lateral column from fusion if possible may be worth consideration.
Moderately successful results with short-term follow-up have been reported for alternatives to fusion of the lateral column. Berlet and Anderson2 reported improvement in a series of eight patients with average 25-month followup treated with a hemiresection and soft-tissue interposition arthroplasty in patients with fourth and fifth TMT arthrosis. Shawen et al.14 reported improvement in patients at 34 months after treatment using an interpositional ceramic ball to treat arthritis in the fourth and fifth TMT joints. These investigators reported strong improvement in AOFAS midfoot scale score but only moderate improvement in visual analog pain score.14 The current biomechanical study shows that isolated medial column TMT arthrodesis unloads the fourth and fifth TMT joints, but we could not investigate possible lateral pain relief from this procedure. It is not yet known whether the best course for lateral pain relief in the setting of medial column TMT fusion is to leave, resect, or fuse the fourth and fifth TMT joints.
We did not look at medial hindfoot pressures in an effort to avoid destabilizing the foot with additional dissection. Future testing in the naviculocuneiform and talonavicular joints may provide useful information about what occurs medially in these fusion constructs. Mann et al.7 reported that the naviculocuneiform joint was the most common adjacent joint to have radiographic degenerative changes in association with TMT fusion. Further biomechanical study should investigate whether isolated medial column TMT fusion puts a more mildly degenerative joint, such as the naviculocuneiform joint, at risk for progression of arthritis.
This study was limited in that it is a cadaver study and does not exactly simulate the clinical setting. The specimens did not have the pathology typically found in patients undergoing the tested procedures. Cyclic tendon loading was not done, and the model does not reflect all the loading positions found in a normal adult. To obtain maximum control of variables by not removing the specimen from the load frame, we started with medial and lateral column fusion but did not resect the joint surfaces and removed screws to simulate isolated medial column fusion and then the intact state. The intact state therefore reflected the manipulation of joints by insertion and removal of screws for the previous treatments and does not exactly simulate the intact state clinically. However, pilot testing showed the order of procedures did not affect the results. Also, each specimen served as its own control and we were able to compare specimens using a consistent approach. Use of a simple wedge to simulate inversion and eversion did not simulate the complex process of ambulation but provided a means to consider the effect of uneven surfaces on the foot.
CONCLUSION
Medial and lateral column TMT fusion significantly increased lateral and calcaneocuboid pressures with loading compared with isolated medial column fusion and the intact state. No difference in these pressures was observed with isolated medial column TMT fusion compared with the intact state. These results may support avoiding fusion of the lateral column fusion when possible.