
Abstract
Level of Evidence: V, Expert Opinion
INTRODUCTION
Osteoid osteoma is a common bone tumor that comprises 10% to 12% of benign bone tumors. The tumor consists of a central vascularized nidus, up to 10 mm in size, surrounded by a zone of uniform bone sclerosis.6 Classification is based on its location in the bone, which includes cortical, medullary, or subperiosteal. Cortical tumors make up 80% of all osteoid osteomas. The tumor occurs predominantly in children and young adults and is more common in males, with a male-to-female ratio of 1.6:1 to 4:1.8 Approximately half of osteoid osteomas occur in the femur and tibia while tumors in the foot are unusual and account for about 4% of cases.14 The talus is the most common bone affected in the foot, and the tumor is usually located in the talar neck.3 Osteoid osteoma usually presents with night pain classically relieved by salicylates. The diagnosis of osteoid osteoma in the foot can be challenging because of unusual location and atypical symptoms, which may mimic more common conditions affecting the foot or ankle.
There are many potential causes of posterior ankle pain.9 These include posterior impingement syndrome, fracture of the os trigonum, Achilles tendonitis or tear, FHL tendonitis, and retrocalcaneal bursitis. Posterior impingement presents with pain at the back of the ankle during forced plan-tarflexion and can occur at night because of the natural plan-tarflexed position of the ankle whilst sleeping. The causes of this include os trigonum, enlarged talar process (Steida process), avulsion of the posterior tibiotalar ligament, prominent posterior process of the calcaneus, loose bodies, or pseudomeniscus syndrome, which impinges against the back of the tibia. The diagnosis is made when there is pain to deep palpation, which is exacerbated by heel compression in plantarflexion.
In this article, we report on two unusual cases of osteoid osteoma in the posterior talar body presenting with classical symptoms of posterior impingement.
CASE REPORTS
Case 1
A 46-year-old woman presented with a 15-month history of posterior ankle swelling, with pain at rest and night with no history of trauma. She had no response to physiotherapy but some relief with aspirin. Physical examination revealed soft-tissue swelling anterior to the Achilles tendon, pain-limited plantarflexion, and a strongly positive posterior impingement test.
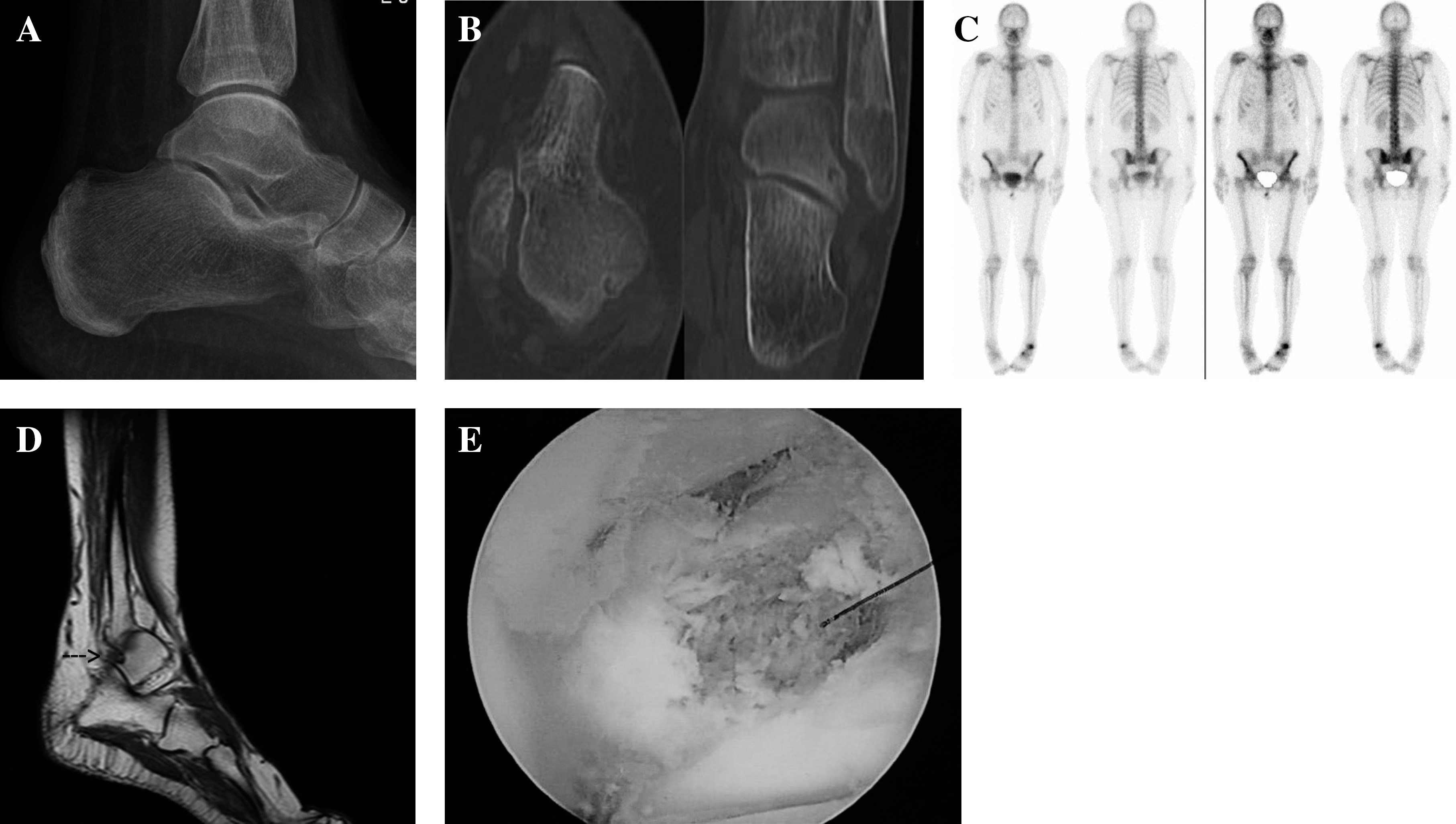
Plain radiographs were normal. CT scan demonstrated a cystic lesion surrounded by a sclerotic zone in the posterior body of the talus. The ankle was further investigated with isotope bone scan and MRI (Figure 1, A to D). The bone scan showed increased uptake in the posterior talus while the MRI showed a small focus of low-signal nidus in the posterolateral talus with surrounding marrow edema on the T1-weighted images. The patient underwent arthroscopic excision through standard portals using curettes and a burr (Figure 1E). Radiofrequency ablation was not available at the hospital. Arthroscopic shavings were not sent for histology. The patient had immediate relief of symptoms, with no recurrence at 4-month followup.
(
Case 2
A healthy 19-year-old woman presented with a 3-year history of spontaneous onset posterior ankle pain. The pain was activity related and associated with posteromedial swelling. Physical examination revealed soft tissue swelling posterior to the medial malleolus, pain-limited plantarflexion and symptoms of posterior impingement.
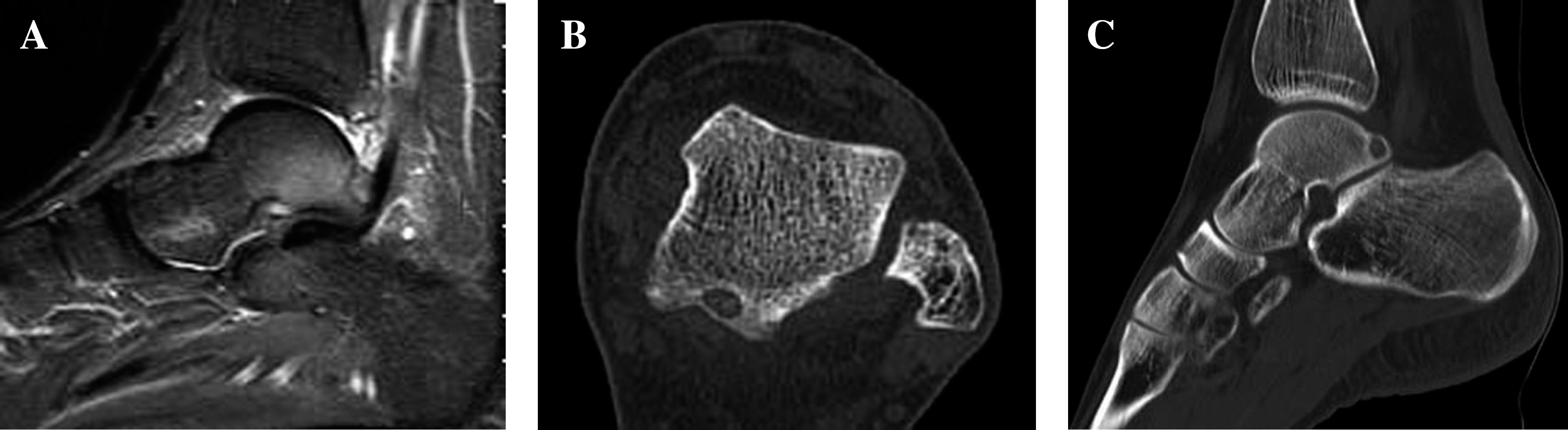
Plain radiographs were normal. An MRI revealed subcortical marrow edema in the posteromedial talus with adjacent soft-tissue swelling and an ankle joint effusion. A CT scan was performed which showed a lucent nidus adjacent to the FHL in the talus with a small amount of rim sclerosis (Figure 2). The patient underwent open excision through a postero-lateral approach. Radiofrequency ablation was not available at the hospital. Histopathology specimens were consistent with osteoid osteoma. The patient made a rapid recovery and was pain-free at 2-week followup, with no recurrence of pain 2-years post-surgery.
(
DISCUSSION
Osteoid osteoma is an unusual tumor in the foot which typically involves the subperiosteal region of the talar neck. There are no reports in the literature of posterior talar body tumors, although Sanhudo13 reported a case of calcaneal osteoid osteoma presenting as posterior impingement. The diagnosis is often delayed because of atypical symptoms which may mimic more common conditions of the foot. Snow et al.15 reported an average delay of 2.5 years in the diagnosis in his series of five talar neck osteoid osteomas.
Usual investigations include plain radiographs, crosssectional CT, bone scan and MRI.1 CT scans can demonstrate the low-attenuation nidus with possible calcification surrounded by a zone of sclerosis. On MRI, the nidus of the tumor shows low or intermediate signal intensity on spinecho T1-weighted images and usually high signal intensity on T2-weighted images and enhancement. 2,5 The extensive changes can be misleading and suggest the diagnosis of osteomyelitis, stress fracture, inflammatory arthritis or a more aggressive bone tumor. Isotope bone scans may show a cold nidus surrounded by intense uptake in the sclerotic region.
The high levels of prostaglandin in the nidus are thought to be the cause of the peritumoral edema and the reason salicylates classically result in relief of pain. 7,17 Treatment with anti-inflammatories is often effective but requires prolonged use. Kneisl and Simon10 found that treatment had to be continued on average for 33 months in their six patient series. The use of radiofrequency ablation and surgical excision is more predictable. Clinical success rates for radiofrequency ablation range from 76% to 100%;4 it is more effective in older patients and with multiple needle passes.16 Surgery remains the standard in cases where histology is in doubt, neurovascular structures are within 1.5 cm or in the repeated failure of ablative techniques and has a success rate of 88% to 100%.4 The above authors also reported complete sustained pain relief in all 15 patients who underwent surgical excision while Yildiz et al.18 had success in 91 of the 104 patients treated with surgery. Lindner12 reported a 95% success rate with initial treatment using CT guided radiofrequency ablation in 58 patients. Laser interstitial thermal therapy has similar success to radiofrequency ablation but is not as readily available. Cryotherapy and ethanol therapy remain second-line therapies.
CONCLUSION
We reported two cases of osteoid osteoma in the posterior part of the body of the talus, presenting as posterior impingement. Although rare in the foot, osteoid osteoma should be considered in the differential diagnosis of foot and ankle pain in children and young adults with no preceeding history of injury, normal inflammatory markers and a history of pain relief from anti-inflammatory drugs.