
Abstract
Level of Evidence: V, Expert Opinion
INTRODUCTION
Metatarsal neck fractures are injuries that often result from a direct blow of heavy objects to the metatarsal head or an indirect force twisting the forefoot. 2,13 Several surgical methods have been introduced to treat displaced fractures when satisfactory reduction and stability could not be obtained by closed reduction techniques. 1,4,6,10,12,14 However, when closed treatment is unsuccessful, open reduction is recommended. 4,5,12 But in many cases, there is soft tissue compromise of the dorsal skin due to a direct blow by a heavy object which may lead to a wound problem after opening the fracture site. Stripping the soft tissue may increase the risk of devascularization.
We have treated displaced metatarsal neck fractures with a closed antegrade intramedullary nailing technique using a prebent Kirschner wire. With this technique, the displaced metatarsal neck fractures were easily reduced without opening the fracture site and at the same time were firmly fixed without impinging on the MTP joint, which allowed immediate motion of the joint.
OPERATIVE TECHNIQUE
The patient is placed on the operating table in supine position under regional anesthesia. Kirschner wire 1.6 mm in width is prepared with 3 mm and 12 mm of the distal end bent 5 degrees (Figure 1). The metaphysis of the affected metatarsal base is exposed through a dorsal incision 1 cm distal to the tarsometatarsal joint. The soft tissue is dissected taking care not to injure neurovascular structures and extensor tendons (Figure 2). An entry hole is made with a 2.0 mm drill bit and one of the prepared Kirschner wires is inserted into the hole and advanced into the intramedullary canal (Figure 3A) until it reaches the fracture site (Figure 3B). Then the Kirschner wire is rotated along its long axis so that the prebent distal end points toward the displaced metatarsal head. The Kirschner wire is advanced into the subchondral bone of the metatarsal head with a gentle tap on the proximal end of the wire with a mallet, taking care not to perforate the joint (Figure 3C). Then the Kirschner wire is rotated along its long axis to reduce the displaced fracture (Figure 3D). The proximal end of the Kirschner wire is cut and left outside of the wound for later removal. Fluo-rocopic images of the procedures are shown on Figure 4. For multiple metatarsal neck fractures with displacement, we attempt to reduce and fix the most displaced one first. After the reduction and fixation of the most displaced fracture, sometimes adjacent fractures become reduced and stable within an acceptable range that did not need additional fixation. We assume this happens because of the intermetatarsal ligaments connected to the adjacent fractured head. When the most displaced fracture is difficult to reduce, then we fix the less severe fracture first, which makes it easier to reduce the most severe one. Postoperatively, we allowed immediate motion of the MTP joint and partial weightbearing in a stiff soled shoe. Full weightbearing is allowed 6 weeks after the operation. The Kirschner wire is removed when there is no pain, which is usually at 6 to 8 weeks.
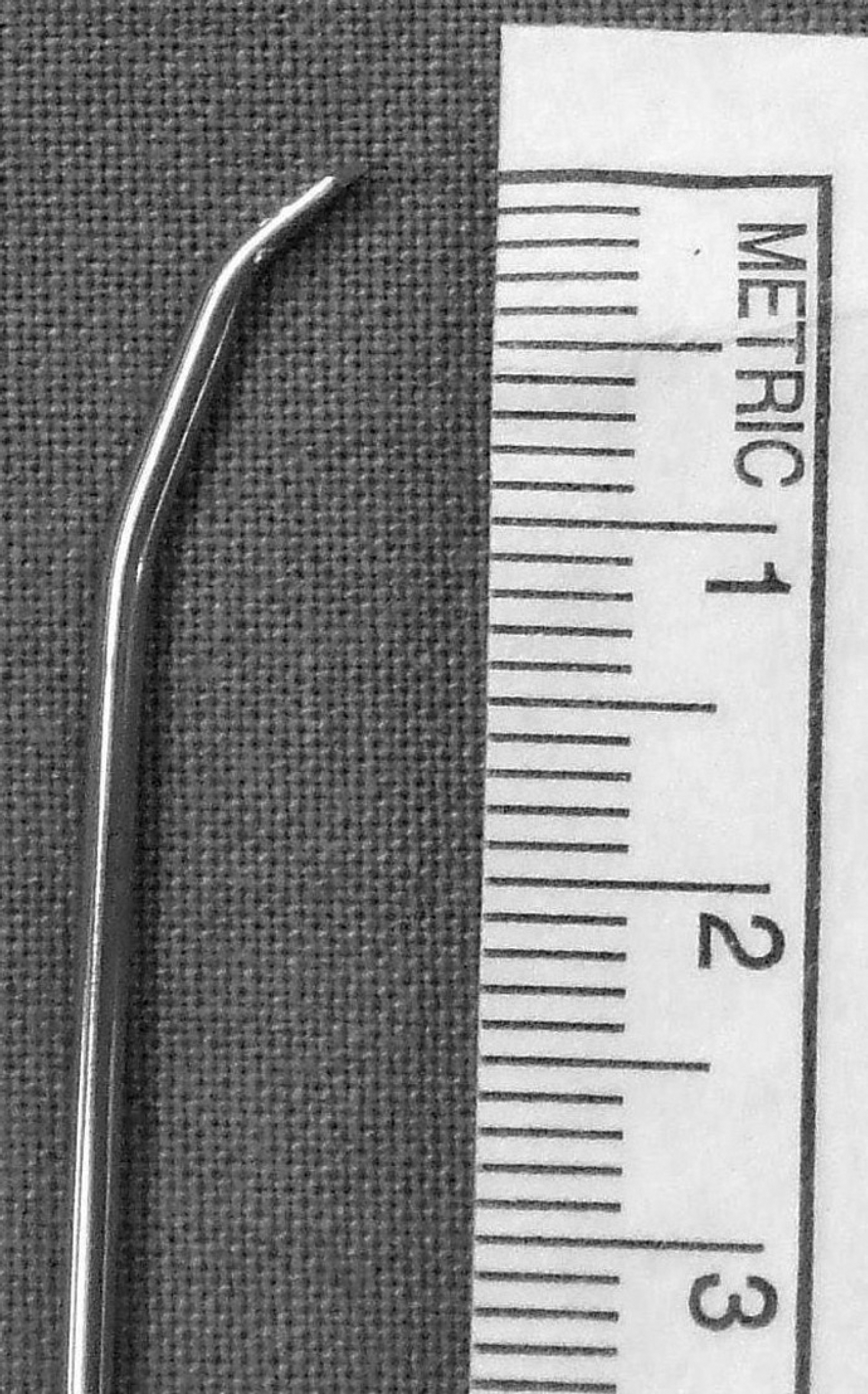
Photograph showing 1.6 mm K-wire with its 3 and 12 mm of the distal end bent 5 degrees.

The metaphysis of the affected metatarsal base is exposed through a dorsal incision 1 cm distal to tarsometatarsal joint. The soft tissue is dissected taking care not to injure neurovascular structures and extensor tendons.
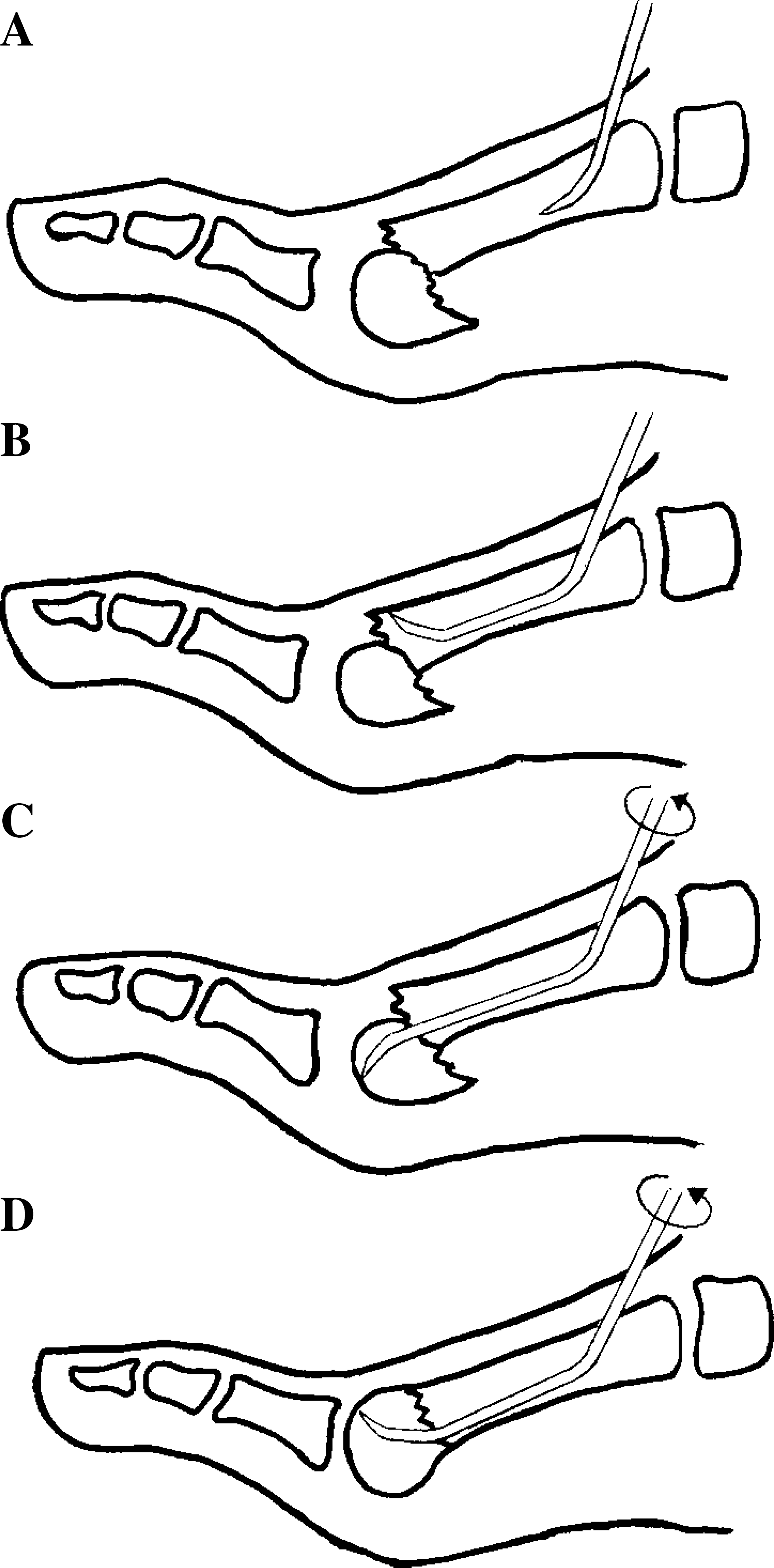
Diagram showing reduction and internal fixation of metatarsal head and neck fractures.
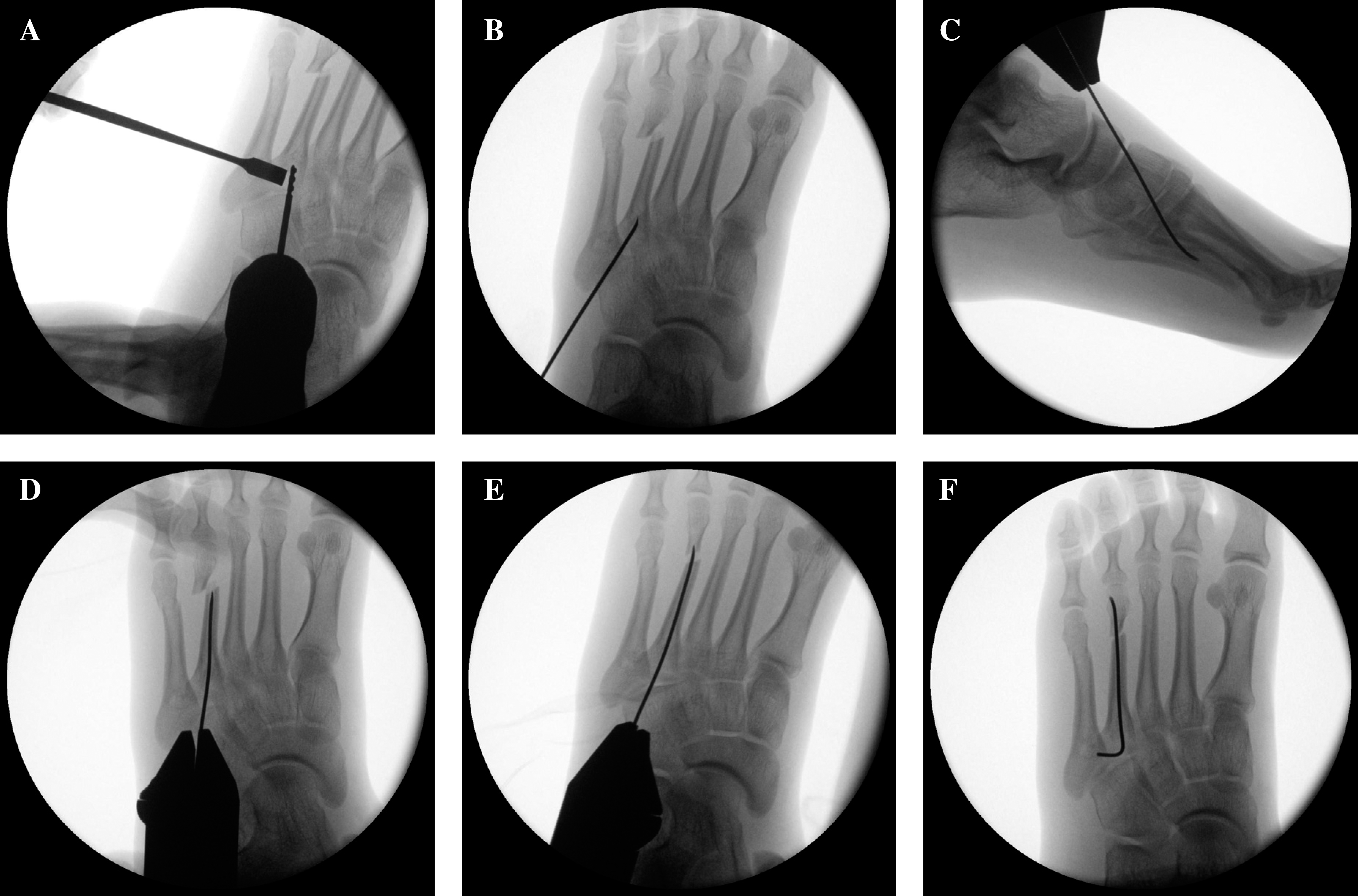
Intraoperative fluoroscopic images showing reduction and internal fixation of the second metatarsal neck fracture.
DISCUSSION
For undisplaced metatarsal neck fractures, immobilization and avoidance of weightbearing pressure in a short leg cast or stiff soled shoe is the generally accepted treatment. 6,12,13 But displacement more than 3 to 4 mm or angulation more than 10 degrees in the sagittal plane needs reduction. 8,12 One of the widely used methods is retrograde percutaneous pinning.12 Without opening the fracture site, the fractured metatarsal head is not easy to control and the reduction is not easy to achieve. Early motion of the joint and early weightbearing are not allowed until the Kirschner wire is removed. Sammarco et al. reported risks of infection, soft tissue damage, and a possibility of metatarsophalangeal joint stiffness with this technique.11 If open reduction becomes necessary, a Kirschner wire can be inserted in an antegrade fashion through the opened fracture site into the distal fracture fragment and to the proximal phalanx, followed by reduction and retrograde insertion back over the fracture site into the proximal fragment.6 However, this technique impinges on the MTP joint and opening of the fracture site which may lead to nonunion.
There are reports showing good results using closed antegrade intramedullary nailing for the reduction and fixation of metacarpal neck fractures. 3,7,9 This technique is based on the principle that the stability is achieved by using the elastic properties of the rod. With this technique, the fracture site is not opened and the articular surface and the capsulo-ligamentous structures are not injured, which allows early motion of the joint. We have used this technique to reduce and fix metatarsal neck fractures with full weightbearing started at an average of 6 weeks and union was obtained at an average of 7 weeks. Early motion of the joint was possible and no stiffness or residual pain was noted.