
Abstract

INTRODUCTION
Hallux rigidus is a common condition characterized by first metatarsophalangeal joint (MTP) degeneration and joint pain. Joint degeneration often includes the formation of dorsal osteophytes that cause pain and limited range of motion of the hallux, mostly in dorsiflexion. Limited range of motion can adversely affect a patient's gait and can lead to pain in the forefoot.
Patients suffering from hallux rigidus most commonly report pain and stiffness in the first MTP joint. The pain is exacerbated with athletic activity and increased ambulation. Pressure from shoe wear can exist secondary to pressure from dorsal osteophytes.
Physical examination often reveals tenderness, swelling, and/or ecchymosis of the first MTP joint. The pain should be classified as dorsal, medial, and/or sesamoidal. Passive and active range of motion is decreased most notably in dorsiflexion. Sensation deficits should be recorded preoperatively, as some patients have decreased function of the dorsomedial cutaneous nerve secondary to compression against a large dorsal exostosis. Every patient should have quantification of the vascular function of the foot. Radiographic examination can show decreased joint space, joint sclerosis, subchondral cysts, and exostoses. Additionally, a loose body, often from osteophyte fracture, can often be seen in the dorsum of the joint.
Coughlin and Shurnas developed a useful clinical and radiographical classification, which helps guide treatment of patients suffering from hallux rigidus (Table 1; Figure 1). 5
Nonoperative treatment for hallux rigidus is attempted prior to surgical methods. Non-surgical treatment includes: foot orthoses with a firm support under the great toe (Morton's extension), shoe wear modification, activity modification, medical therapy, and injection therapy. Grady et al. 11 found that out of 772 patients suffering from hallux rigidus, 55% of patients were treated successfully with nonoperative measures.
For those patients who have failed nonoperative methods, there are many surgical options available. Treatment for hallux rigidus has been classified as joint sparing versus joint sacrificing. Joint sparing techniques include: cheilectomy, proximal phalangeal osteotomy, first metatarsal osteotomy and interpositional arthroplasty. Joint sacrificing techniques include implant arthroplasty and arthrodesis.
In this paper, the authors describe several surgical options for hallux rigidus, their preferred treatment options and offer some surgical techniques. A simple treatment philosophy has developed, with joint preservation a priority along with early weightbearing when possible. The simple choice of cheilectomy or fusion has been markedly expanded with the success of interposition arthroplasty procedures. Fusions are now reserved for complex revision cases, severe bone loss, rheumatoid arthritis, and severe joint instability.
CHEILECTOMY
A cheilectomy consists of excision of the dorsal osteophytes surrounding the first metatarsophalangeal (MTP) joint (Figure 2). These osteophytes often interfere with first MTP joint motion, primarily dorsiflexion. DuVries first described the cheilectomy technique in 1959. Cheilectomy has been indicated in hallux rigidus grades 1 to 3. Authors have debated regarding using cheilectomy in advanced stages of hallux rigidus.
Classification System for Grading Hallux Rigidus 5
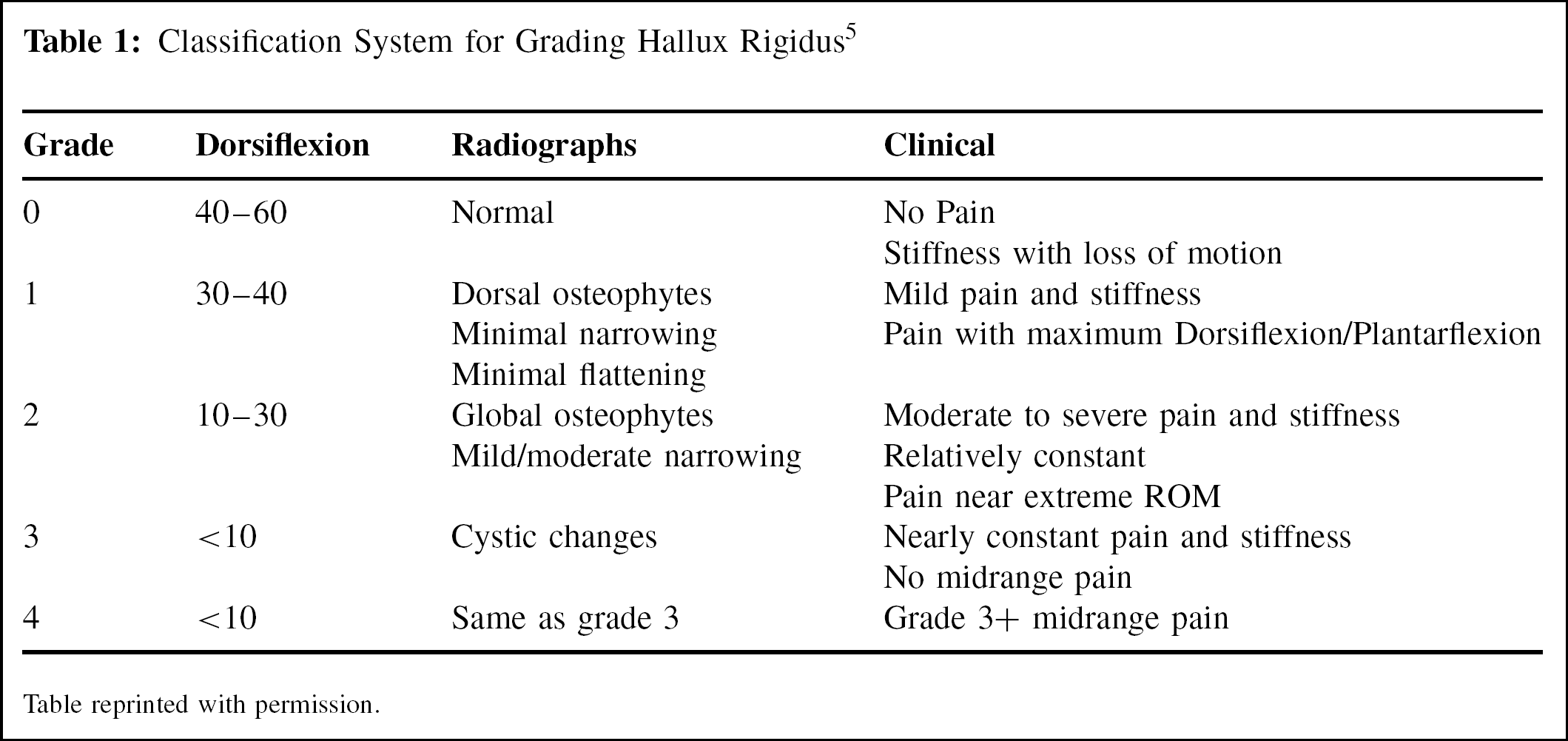
Table reprinted with permission.

AP (A) and lateral (B) views of foot with moderate arthritic changes.
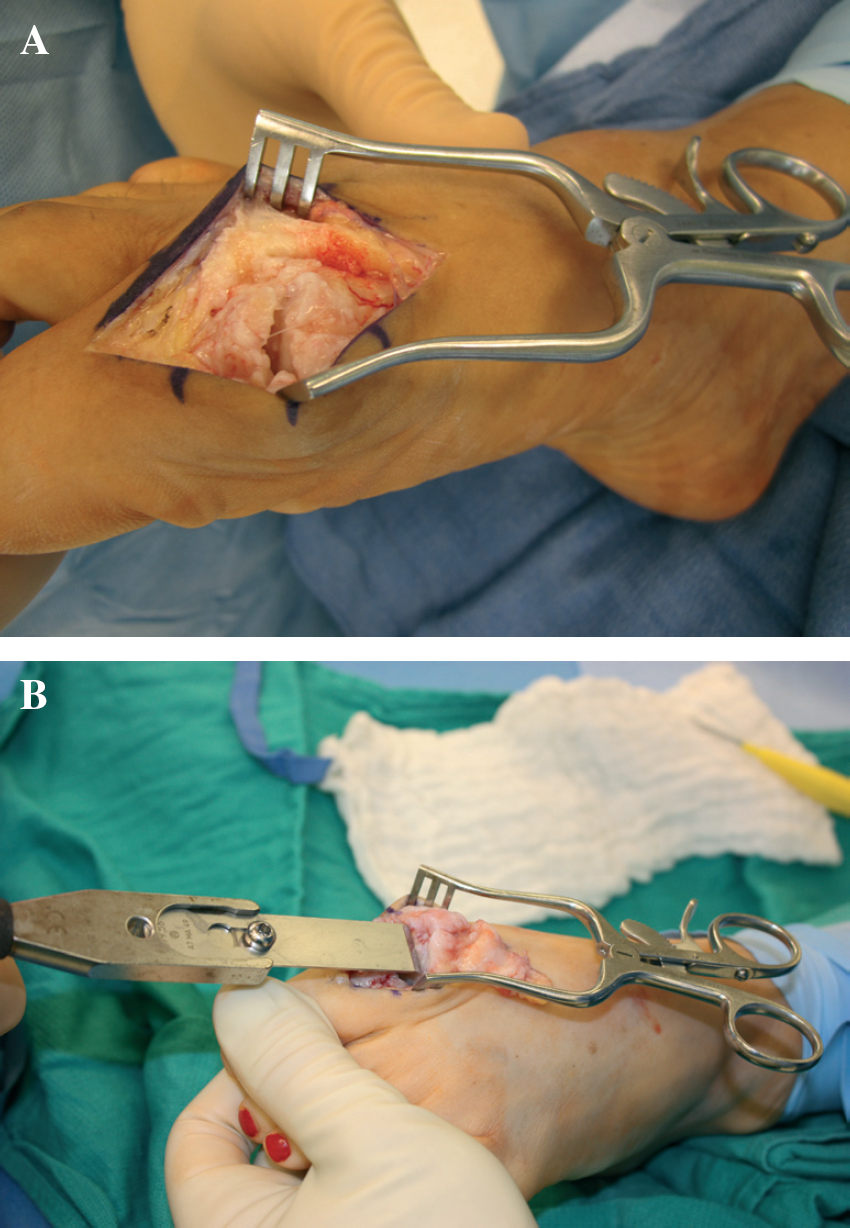
Standard cheilectomy resection of the dorsal metatarsal head may be performed with either the chisel or oscillating saw. Up to one-third of the head may be resected.
Technique
Incision: longitudinal on the dorsum of the first metatarsophalangeal joint medial to extensor hallucis longus tendon.
Dorsal medial cutaneous nerve of the toe is identified and protected.
The capsule is incised to gain access to the first MTP keeping the capsular incision away from the EHL in the attempt to prevent later adhesions to it.
A straight osteotome or power-oscillating saw is used to perform an osteotomy of the dorsal osteophytes of the first MTP joint. The direction of the osteotomy is surgeon preference with some advocating for proximal to distal to avoid notching of the metatarsal.
Once osteotomy is completed, the goal of passive dorsiflexion is approximately 70 degrees (Figure 3). 5
If continued joint impingement is noted, additional bone may be removed up to 30% of the metatarsal head.
If inadequate dorsiflexion is still not achieved, then a proximal phalanx dorsal closing wedge osteotomy (Moberg) should be considered.
Close capsule and skin.
Postoperatively, patients are instructed to ice and elevate the affected extremity as much as possible during the initial postoperative period. Dressing should be maintained until the first postoperative visit. Patients can be weightbearing as tolerated in a postoperative shoe. Crutches may be used if there is too much pain with ambulation. Patients may progress to normal shoe wear following the first postoperative visit. Active and passive early range of motion is critical to maintaining the improved range of motion. The final range of motion is usually less than was achieved intraoperatively.
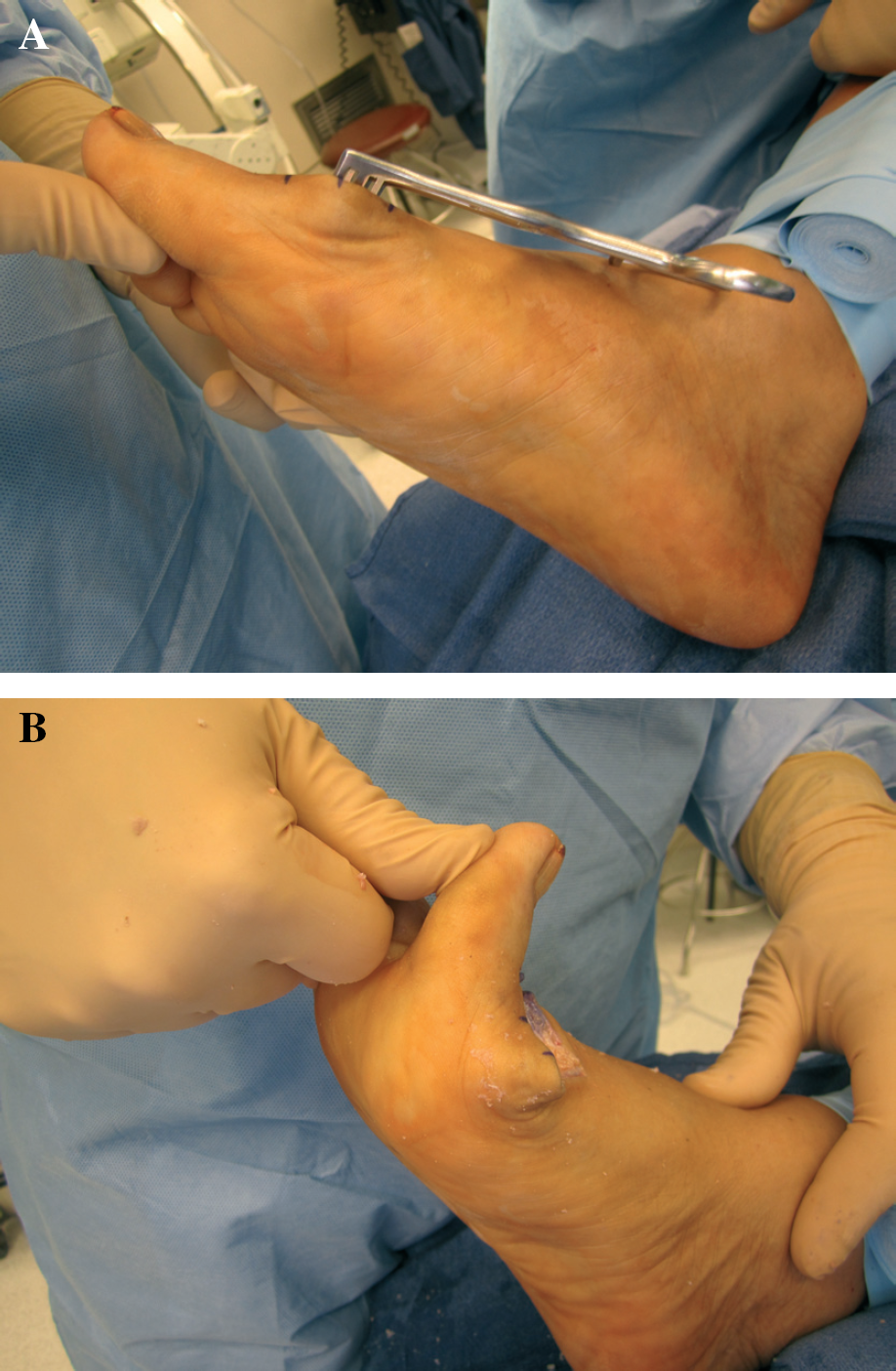
Pre- (A) and postoperative (B) dorsiflexion.
Although cheilectomy is a rather simple technical procedure, there are potential risks including recurrence of exostoses and advancement of osteoarthritis. Easley et al. reported a re-occurrence rate of 30%. 9 Coughlin et al. reported an increased rate of degeneration after cheilectomy. 5 Other possible complications of cheilectomy include infection, neuroma formation, paresthesias of the hallux, and complex regional pain syndrome.
Cheilectomy of the first MTP joint has yielded favorable results for patients with earlier stages of hallux rigidus. Multiple studies have examined the use of cheilectomy in the treatment of hallux rigidus, and its use has been supported, mostly by Level IV studies. Cheilectomy can be performed with predictable success to treat grades 1 and 2 hallux rigidus, and select cases of grade 3. 5
Mann and Clanton reported that 22 out of 25 of their patients had adequate or complete relief of pain after cheilectomy, and no patient returned to the operating room. 19 Seibert et al. stated that cheilectomy remains the “gold standard” for patients suffering from mild to moderate hallux rigidus. 27 Lau et al. compared patients with grade 2 hallux rigidus to those suffering from grade 3. Grade 2 patients received a cheilectomy and grade 3 patients were treated with an interpositional arthroplasty. Those who underwent cheilectomy had increased satisfaction scores and increased function in some regards. 17 Additionally, Coughlin et al. stated that although cheilectomy does not alter the degeneration process, it does allow patients increased comfort. 5
Cheilectomy has been indicated as a first line surgical treatment option for patients suffering from hallux rigidus, grades 1 to 3. Although the results of this procedure have been successful, there are instances where it fails, resulting in the progression of first MTP joint degeneration and pain. Reasons for failed cheilectomy include inadequate osteophyte/bone resection which causes impingement. Second, there may be too much bone resection which causes MTP joint instability. Also, performing the procedure on patients with advanced stages of hallux rigidus will lead to inadequate pain relief. The salvage procedure for patients having failed cheilectomy would include a first MTP fusion, as recommended by Coughlin and Shurnas in 2004. 6 Additional Level IV studies investigate the use of first MTP arthrodesis as a salvage procedure. Brage et al. published a study in 2002 stating that a first MTP joint arthrodesis is the treatment of choice in young, active patients that have failed cheilectomy. 4 Myerson and Schon et al. performed first MTP fusions on patients with subsequent shortening and metatarsalgia after first ray surgery, including cheilectomy. Results stated that there is an increased risk of non-union, but an arthrodesis with bone graft may be successful in restoring first ray length. 23
Even though cheilectomy is a successful treatment option, there have been other joint sparing procedures described. It is the opinion of Coughlin et al., that patients with advanced grade 3 and those with grade 4, hallux rigidus should be treated with advanced joint sacrificing techniques. 5 The authors of this paper concur with these findings, often making a decision to progress to more aggressive treatment depending upon intraoperative findings of osteoarthritis.
PHALANGEAL OSTEOTOMY
In patients suffering from early stage hallux rigidus, osteotomies may be used as joint sparing procedures, with hopes to increase the amount of dorsiflexion of the first metatarsophalangeal joint. Proximal phalangeal osteotomy is performed to provide more dorsiflexion. The arc of motion of the first MTP joint is translated from plantar to dorsal, which increases the functional range of motion and decompresses the painful/arthritic joint. Moberg popularized the proximal phalanx osteotomy, and his name is commonly associated with the procedure. In 1979, Moberg introduced his technique, performed on eight patients, and the results were satisfactory. 21
Moberg technique
Isolate dorsal first proximal phalanx.
Guide wire is placed at the proposed site of osteotomy to confirm extra articular placement and adequate proximal fragment for osteotomy fixation.
Dorsal-based wedge osteotomy averaging 3 mm, cut two-thirds of the way across phalanx, and then green stick the plantar cortex.
Fixation can be tension band with suture capable of withstanding high tension (wire or polyethylene), metal staple, small bone screw, or Kirschner wire.
Complications of the Moberg may include loss of fixation, floating toe, accelerated arthritic degeneration from an intraarticular perforation of the osteotomy, and non-union.
Citron and Neil stated, in their study of young women, that dorsal phalangeal osteotomy provides long lasting benefits. They performed an osteotomy in eight patients, and found that after 22 years, three patients were symptom free, and only one patient required a revision in the form of a fusion. 7
Level IV studies have shown that a dorsal proximal phalangeal osteotomy is beneficial when combined with a cheilectomy. Blyth et al. performed combined procedures in 18 patients suffering from hallux rigidus, grades 1 through 3. Results indicate that 14 patients had good or excellent results after an average 4-year followup. 3 Thomas et al. found that patient satisfaction with combined osteotomy and cheilectomy was 96% versus 73% in the cheilectomy only group. 29 Additionally, Lau et al. stated that management of moderate hallux rigidus with a cheilectomy and phalangeal osteotomy is a reliable method of relieving pain and improving function. 17 In a 2009 review article, Seibert et al. reiterated that a proximal phalangeal osteotomy is not recommended as a solo procedure, but should be combined with a cheilectomy. 27 The authors of this article occasionally use a Moberg in conjunction with cheilectomy.
METATARSAL OSTEOTOMY
An alternative technique to decompress the hallux metatarsophalangeal joint is to perform a metatarsal osteotomy. It has been proposed that hallux rigidus may be caused by disorders of the first metatarsal, including possible metatarsus primus elevatus and a too long first metatarsal. Metatarsal osteotomies are performed to theoretically unload the first MTP joint by shortening it and re-orienting the joint surface. Osteotomies of the first metatarsal allow extra-articular correction that which prevents stiffness of the first MTP joint. Proximal and distal osteotomy techniques have been described thoroughly in the podiatric literature. Techniques have been limited in discussion among the orthopedic literature.
YOUNGSWICK-AUSTIN
The Youngswick-Austin procedure allows increased plantarflexion of the first ray without excessive shortening of the first metatarsal. The procedure involves a chevron-type osteotomy with the addition of a proximal dorsal metatarsal osteotomy. The metatarsal head can then be oriented plantar and proximally. 30
Technique
A thigh tourniquet is applied so that excursion of the extrinsic tendons is not limited, which could alter the intraoperative motion at the first MTP joint.
A standard dorsal skin incision is made just medial to the EHL tendon.
Care is taken to protect the dorsomedial cutaneous nerve.
A dorsomedial longitudinal incision is made in the joint capsule and the capsule is reflected laterally.
The joint surface is inspected for evidence of arthritis.
A “V” type of osteotomy is created in the head of the first metatarsal with the apex distal and the dorsal arm proximal at approximately 60 degrees (measured from the reference line up) and plantar arm proximal at approximately 30 degrees (measured from the reference line down). A parallel osteotomy to the dorsal arm is made creating a predetermined segment of bone.
The capital fragment is distracted and plantarflexed on the metatarsal shaft correcting the sagittal plane deformity (lateral shift will allow for transverse plane correction if necessary).
The segment of bone from the dorsal cut is retrieved and placed plantarly into the osteotomy gap.
A 0.045-inch Kirschner wire is then utilized as temporary fixation across the osteotomy site from proximal to distal.
Osteotomy screw fixation is from dorsal distal to plantar proximal.
Capsulorrhaphy may be performed as needed.
Postoperatively, patients are instructed on minimal weight-bearing or heel weightbearing in a postoperative shoe and are followed up in 3 to 5 days. Physical therapy consisting of active and passive range-of-motion exercises is often prescribed beginning 2 to 3 weeks postoperatively. Serial radiographs are performed and the patient is returned to regular shoes in 4 to 6 weeks depending on trabeculation and healing across the osteotomy and graft.
WATERMANN/GREEN-WATERMANN
The Watermann, described in 1927, removes a trapezoidal shaped wedge from the dorsum of the metatarsal head, aiming to rotate the healthier, plantar-based cartilage up to re-establish a healthy joint surface. The procedure can be used as a primary correction or in combination with a proximal osteotomy. The modified Green-Watermann osteotomy includes a chevron-type osteotomy in addition to the resection of a small dorsal segment of bone. The goals of the modification include first ray shortening in order to relieve tension on the flexor structures, and to shift the metatarsal head plantarly.
Technique
A thigh tourniquet is applied so that excursion of the extrinsic tendons is not limited, which could alter the intraoperative motion at the first MTP joint.
A standard dorsal skin incision is made just medial to the EHL tendon.
Care is taken to protect the dorsomedial cutaneous nerve.
A dorsomedial longitudinal incision is made in the joint capsule and the capsule is reflected laterally.
The joint surface is inspected for evidence of arthritis.
Dorsal cheilectomy.
A medial-to-lateral osteotomy from proximal plantar to dorsally and distally into the metatarsal head.
The degree of osteotomy will determine the ratio of metatarsal shortening to plantar transposition.
Detach saw blade to prepare for two dorsal ostetomies.
A rectangular or trapezoidal section of bone in the dorsal one-third of the metatarsal head is resected, maintaining a perpendicular relationship to the weightbearing surface.
The section of bone is removed to allow shortening, and the capital fragment is slid proximally and plantarly along the plantar slope of bone.
Lateral transposition of the capital fragment if necessary.
Osteotomy fixation with threaded Kirschner wire or cancellous screw.
Capsulorraphy if needed.
Postoperatively, patients are instructed on minimal weight-bearing or heel weightbearing in a postoperative shoe and are followed up in 3 to 5 days. Physical therapy consisting of active and passive range-of-motion exercises is often prescribed beginning 2 to 3 weeks postoperatively. Serial radiographs are performed and patient is returned to regular shoes in 4 to 6 weeks depending on trabeculation and healing across the osteotomy and graft (Figure 4).
Level IV studies claim that a first metatarsal osteotomy may yield increased patient satisfaction, as well as increase in range of motion. In 2002, Dickerson et al. 8 looked at patient outcomes 4 years after a Green-Waterman osteotomy. Results showed that 94% of patients had decreased pain (Level IV). In 2002, Roukis et al. conducted a Level III, prospective study comparing 50 feet that had undergone decompression of the first metatarsal via an osteotomy. Results indicated that there was improvement in pain, function, and alignment; however there were associated complications of medial column instability due to first metatarsal shortening. 24 Kilmartin et al. conducted a Level V study investigating outcomes between patients undergoing phalangeal or metatarsal osteotomies in the treatment of hallux rigidus. Results showed that dorsiflexion of the first MTP joint was increased, but there were complication risks with the procedures. The phalangeal group fared better in the study with regard to patient satisfaction and complications, but neither procedure was recommended as a definitive treatment of hallux rigidus. 16
The Level IV studies that support the use of a first metatarsal osteotomy also discuss the risks for complications. Coughlin and Shurnas believed that metatarsus primus elevatus rarely needs to be corrected with an osteotomy and that a cheilectomy may be a simple enough procedure to correct the deformity. 5
There is evidence, as reported by Seibert and Anish, to refute the first metatarsal osteotomy as a treatment for hallux rigidus. They cautioned that osteotomies yield increased risks, which may affect outcomes. 27 First metatarsal osteotomies may over shorten and provide sesamoid overload and pain. 12 In 2010, Roukis performed a Level I systematic review revealing high incidence of complications regarding first metatarsal osteotomies in the treatment of hallux rigidus. Of the 93 cases evaluated, 22.6% of patients had to undergo revision surgery. Additionally 30.5% of patients had been diagnosed with a first metatarsal stress fracture or metatarsalgia. In concluding his study, Roukis discredited the use of isolated periarticular osteotomies of the first metatarsal in the treatment of hallux rigidus. 25

Postoperative AP (A) and lateral (B) views of a first metatarsal osteotomy.
In conclusion, proximal phalangeal osteotomy has been seen as beneficial in the treatment of hallux rigidus especially when combined with a dorsal cheilectomy. First metatarsal osteotomy has been shown to be effective in the short term with long-term data showing increased incidence of complications. These authors rarely use a shortening osteotomy of the first metatarsal, essentially because of limited expectations of long-term success.
CAPSULAR INTERPOSITION ARTHROPLASTY
Grade 3 and 4 hallux rigidus demonstrates inferior results when treated with a cheilectomy procedure. 5 Surgical options in patients with advanced hallux rigidus have traditionally included arthrodesis and implant arthroplasty. While arthrodesis offers good clinical outcomes, patients sometimes find it less desirable secondary to prolonged weight bearing restrictions postoperatively and shoe wear limitations once the arthrodesis has healed. Implant arthroplasty has been shown to have a high complication rate and is not recommended by many orthopedic surgeons. 10,28 For these reasons, interposition procedures have been advocated.
Hamilton described a modified technique whereby the proximal phalanx resection is smaller than the original resection proposed by Keller, and the short flexor is released from the base of the proximal phalanx and sutured to the short extensor to provide tissue interposition in the joint. 13 This resection is a minimally morbid technique with easy fusion salvage option unlike joint replacement options. Early results were good, but at least one long-term study showed problems with toe strength and demonstrated unfavorable outcomes when compared to simple cheilectomy. 17 Mroczek and Miller published their technique of dorsal capsular interposition while preserving the attachments of the FHB and plantar plate in the base of the proximal phalanx. 20 This is accomplished with an oblique resection of the dorsal base of the proximal phalanx, leaving the plantar aspect of the phalanx intact in order to avoid sacrificing intrinsic muscle attachments. Most of the data is Level IV evidence, but several studies have been published that document good clinical outcomes using the modified Keller technique of Mroczek and Miller. Kennedy et al. reviewed 18 patients who had an FHB preserving capsular interposition arthroplasty and noted good results with improvement in range of motion and AOFAS scores. All but one patient stated they would have the procedure again. 15 Another Level IV study reported on 11 patients with an average of 27-month followup and noted good or excellent results in all patients. 1 One Level III study compared the FHB preserving capsular interposition arthroplasty to arthrodesis. Overall clinical outcomes were similar between groups but the motion preserving procedure had more normal plantar pressures with ambulation. 18 Sanhudo et al. recently published Level IV followup on 25 feet with grade 3 or 4 hallux rigidus that underwent FHB sparing dorsal capsule interposition arthroplasty, noting good results in the majority of the cases. 26
Here we describe a technique of dorsal capsular interposition arthroplasty that preserves the FHB and plantar plate attachments to the proximal phalanx.
Technique
A thigh tourniquet is applied so that excursion of the extrinsic tendons is not limited, which could alter the intraoperative motion at the first MTP joint. Alternatively, the ankle Esmarch bandage can be released when assessing range of motion.
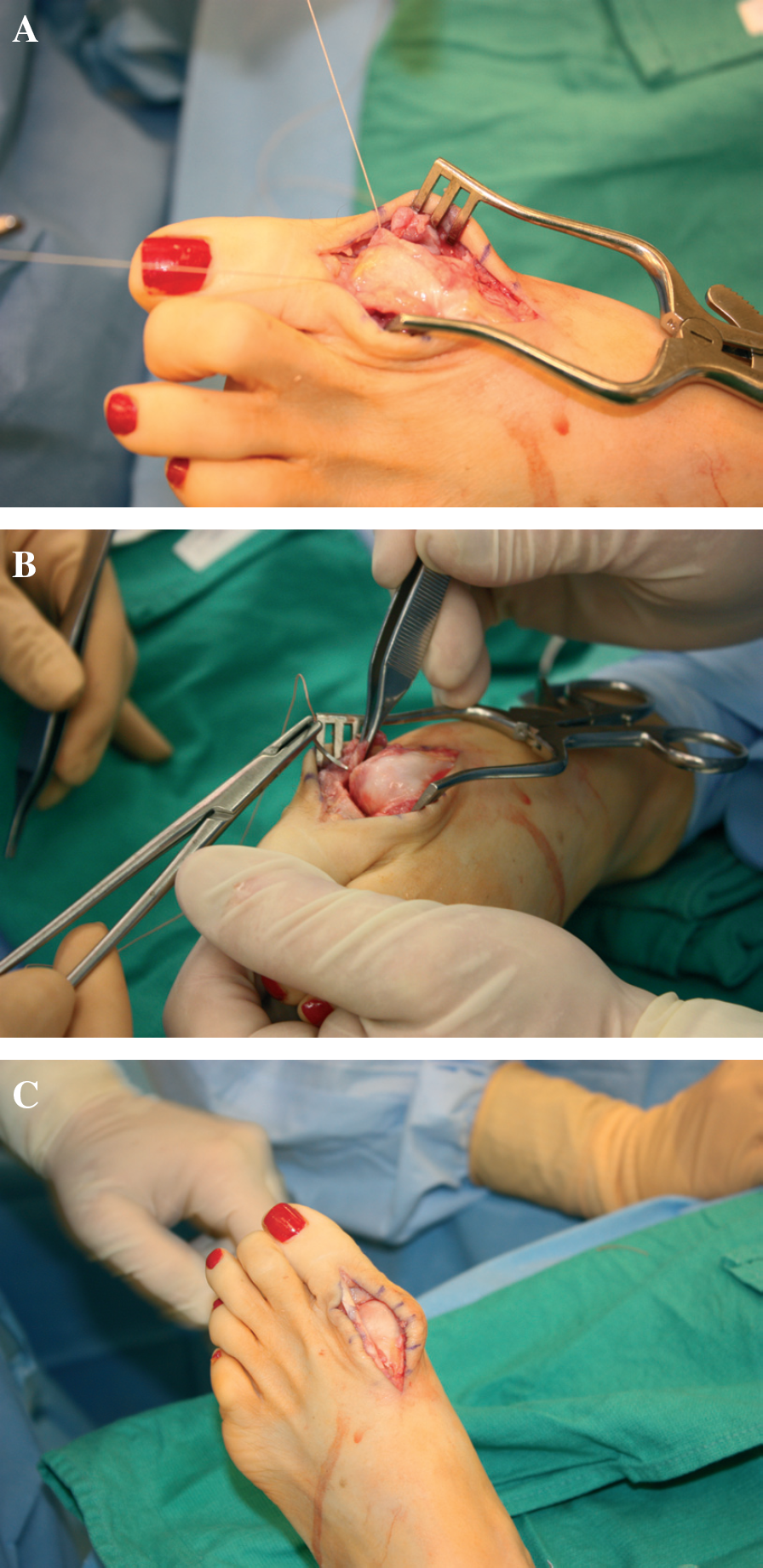
A standard dorsal skin incision is made just medial to the EHL tendon (Figure 5).
Care is taken to protect the dorsomedial cutaneous nerve.
A dorsomedial longitudinal incision is made in the joint capsule and the capsule is reflected laterally. This incision contrasts with a standard central capsular incision, since a capsular flap might be needed.
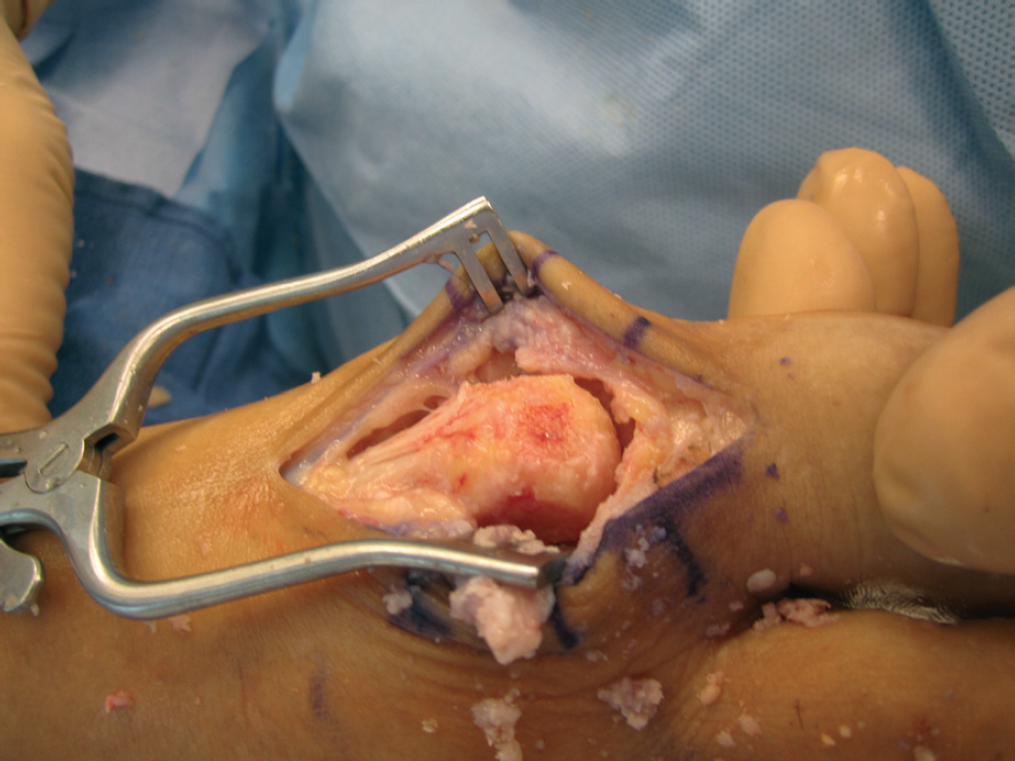
The joint surface is inspected for evidence of arthritis. If the cartilage is intact then a simple cheilectomy can be performed. If the joint is degenerated then the surgeon can proceed with the capsular interposition arthroplasty (Figure 6).
The EHL tendon is mobilized and retracted laterally.
The dorsal capsule at the level of the midportion of the proximal phalanx is incised horizontally, and another longitudinal capsular incision is carried down the dorsolateral aspect of the MTP joint (Figure 7).
The capsule is reflected proximally, leaving the proximal base intact on the metatarsal neck.
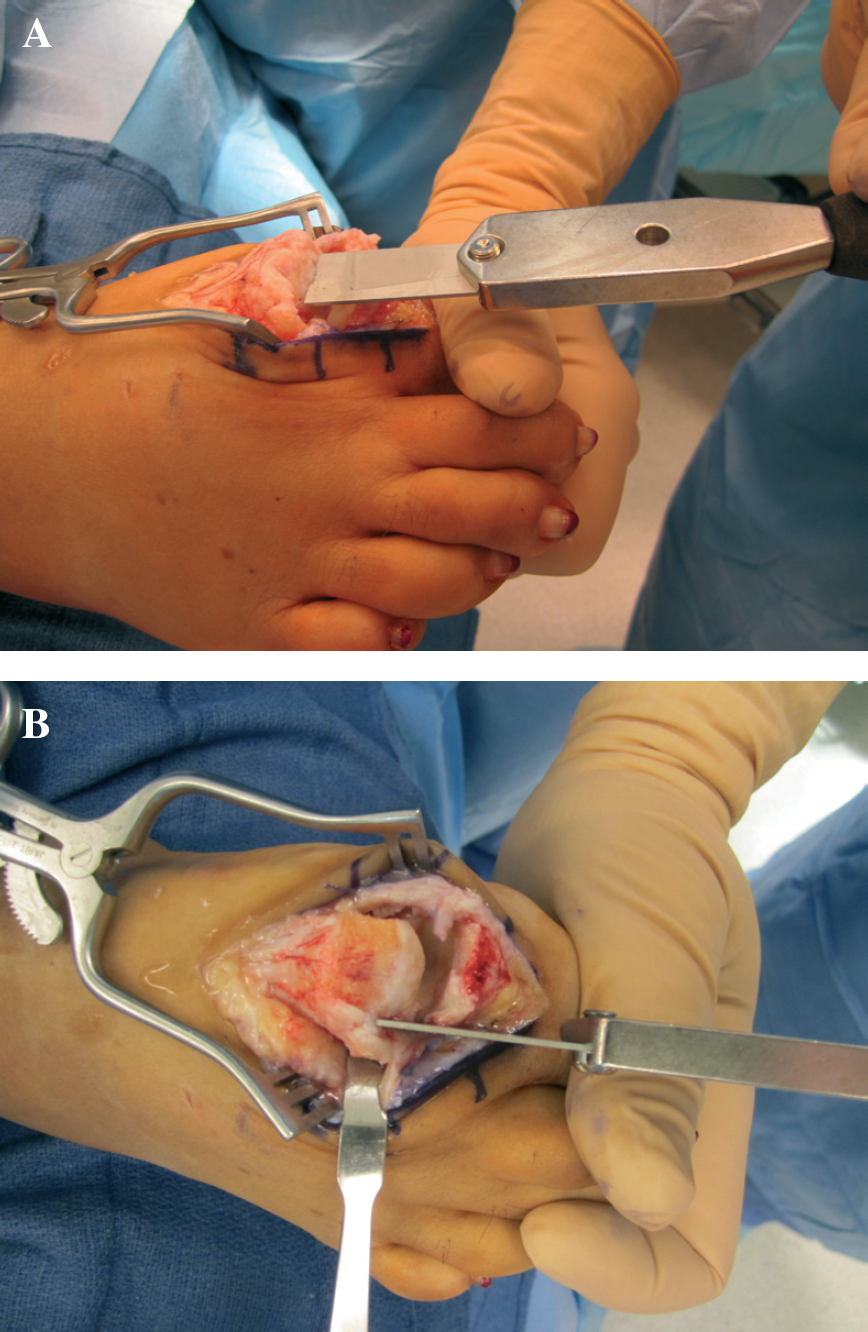
Cheilectomy of up to one-third of the diameter of the metatarsal head is performed with a microsagittal saw or chisel. Medial and lateral exostectomies are similarly performed on the metatarsal head (Figure 8).
The base of the proximal phalanx is removed with an oblique cut from dorsal and distal to plantar and proximal, taking care to preserve the plantar plate and the insertion of the FHB in the base of the proximal phalanx. The authors now advocate resection with a convex MTP reamer at an oblique angle, thus maintaining a curvature at the proximal phalanx.
Should the capsule be extremely thin or not intact, or if the sesamoid articulations are severely damaged, the surgeon may choose to progress to an extracellular tissue matrix interpositional arthroplasty.
The joint is now assessed for passive range of motion. At least 90 degrees of passive dorsiflexion is required. If adequate dorsiflexion is lacking then slightly more phalangeal bone can be removed.
The EHB tendon is transected more proximally which allows the dorsal capsular flap to be mobilized and brought over the head of the first metatarsal.
The lateral corner and the medial corner of the dorsal flap are sequentially secured to the plantar plate with 2–0 vicryl horizontal mattress stitches. This remains a difficult part of the procedure. The interposition flap is then sewn to the medial and lateral dorsal capsular tissue to further increase stability of the interposition (Figure 9).
Joint motion is reassessed (Figure 3B). The wound is thoroughly irrigated and hemostasis is achieved.
The wound is then closed in layers (subcutaneous tissues and skin) and sterile soft dressing is applied.
Patient is instructed to weightbear as tolerated in a stiff postoperative shoe.
Ice and elevation is encouraged to minimize swelling.
At the first postoperative visit the dressing is removed and the patient is able to shower. The patient then begins passive range of motion of the MTP joint, and may begin to wean to regular shoes.
Full recovery may take several months for vigorous physical activities.

Incision is medial to extensor hallicus longus tendon.

After the arthrotomy, the metatarsal head can be visualized. In this case, the damage is too extensive for performance of a simple cheilectomy.

The distal portion of the capsular flap can be marked and cut, usually midway on the proximal phalangeal shaft length. The lateral segment of the capsular flap can be incised, thus creating a proximally based flap.
A, Standard cheilectomy resection of the dorsal metatarsal head may be performed with either the chisel or oscillating saw. Up to 1/3 of the head may be resected.
EXTRACELLULAR MATRIX INTERPOSITION ARTHROPLASTY
The interest in preserving motion of the first MTP joint remains strong from a patient perspective, especially since many joint-preserving procedures allowing early weight-bearing. As mentioned in the previous section, the capsular interposition arthroplasty described by Mroczek and Miller has shown excellent results for hallux rigidus that is not amenable to cheilectomy. 1,15,18,22 However, sesamoid pain remains a contraindication for the procedure. If the sesamoids hurt, then increased motion may worsen the pain. The surgical options will be limited to fusion or interpositional arthroplasty using a regenerative tissue matrix. The latter provides a good solution to grades 3 and 4 hallux rigidus with sesamoid involvement and results at 5 years are encouraging, though all evidence at this point in time is Level IV. 2,14 Mark's concept of a concentric phalanx osteotomy, the COBRA, makes sense but the curvilinear oscillating saw is not a common tool in many operating rooms. 18 A modification to a more anatomic resection of the metatarsal head and proximal phalanx using conical reamers has made the resection easier and more reproducible.
A, Stitch into the lateral aspect of the interposition flap while preparing to drive the needle through the plantar plate to secure the interposition flap.
Here we describe a technique for interpositional arthroplasty using a regenerative tissue matrix. This technique is ideal for cases of severe hallux rigidus in the setting of sesamoid pain and when a good capsule to interpose might not be available.
Technique
The incision is a dorsal midline approach medial to the EHL tendon.
The dissection is carried deep with Steven scissors to the capsule; attempt should be made to leave the EHL sheath intact.
The capsule is incised longitudinally leaving enough capsule to close without involving the EHL sheath (Figure 5).
The entire head is exposed and the plantar scar tissue proximal to the sesamoids is released on the metatarsal, often with a McGlamry elevator.
The dorsal half of the proximal phalanx is exposed.
The metatarsal head dorsal one-third is removed with an osteotome (Figure 10). The medial eminence just medial to the sagittal groove and prominent lateral osteophytes are also resected (Figure 11).
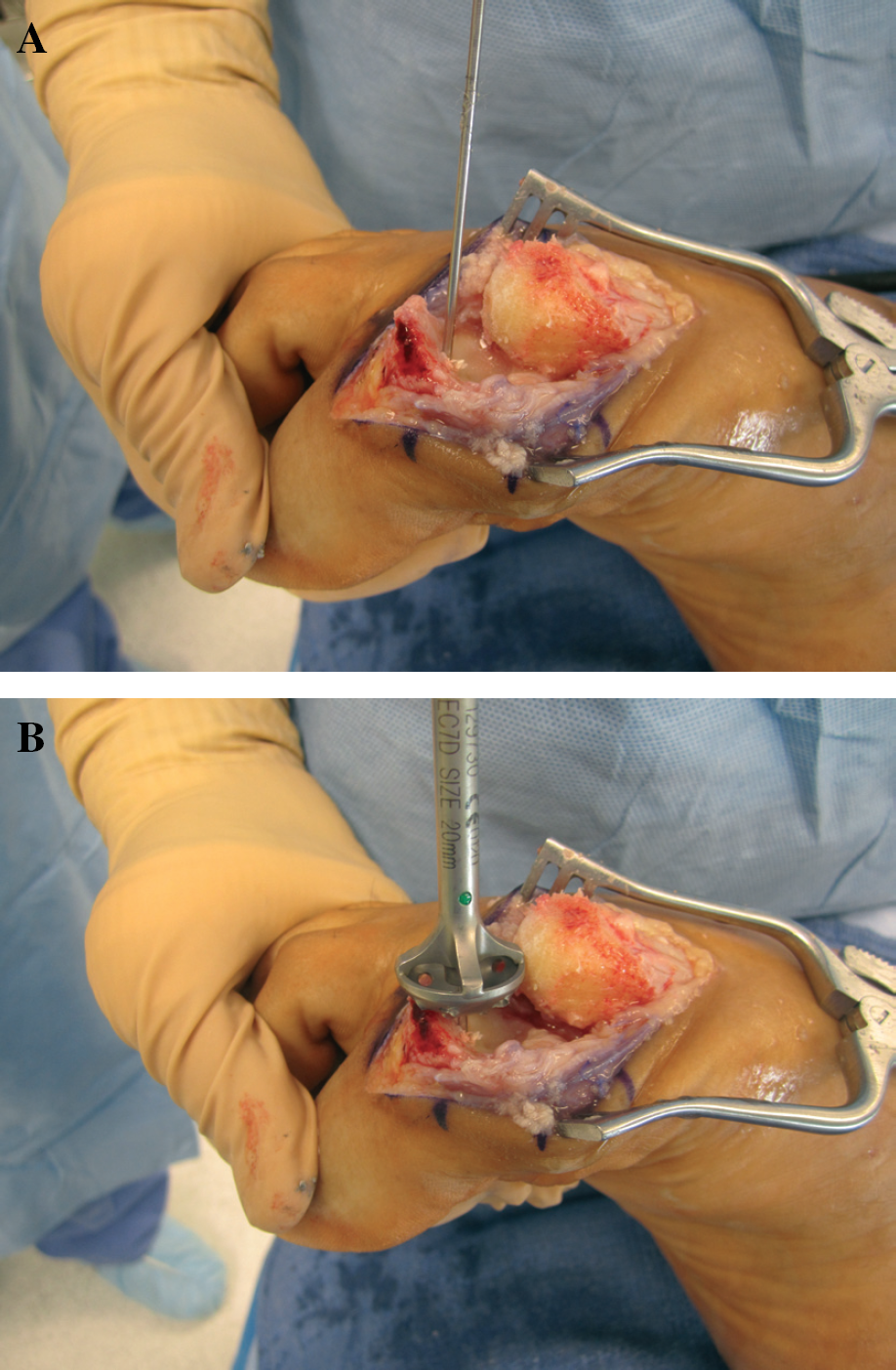
A conical reamer from the MTP Fusion tray is used to pare the cartilage and some subchondral bone on the metatarsal head.
The guide pin is placed in standard fashion in the middle of the metatarsal head and an appropriate sized reamer used, usually 18 mm (Figure 12).
The guide wire is placed in the dorsal one-quarter and angled plantar (Figure 13A). The phalanx is then reamed but in an oblique fashion (Figure 13B). The same sized matching convex reamer is then used to remove the dorsal portion of the proximal phalanx, care being taken to avoid damage to the plantar aspect of the joint and the short flexor tendon attachments. Alternatively, some may choose to leave the phalanx cartilage intact.
Once the resection is complete, the joint should have “play” or “shuck” and be loose enough to allow extension to at least 90 degrees.
While preparing the joint, a 4 cm × 7 cm tissue matrix graft should be soaking in saline. The implant is then prepared by placing two sutures of 0 Vicryl in the base (Figure 14).
A Kirschner wire or drill bit can be used to drill two holes in the metatarsal neck from dorsal to plantar, the proximal aspect of which should be proximal to the sesamoids and large enough to accommodate a suture passer (Figure 15).
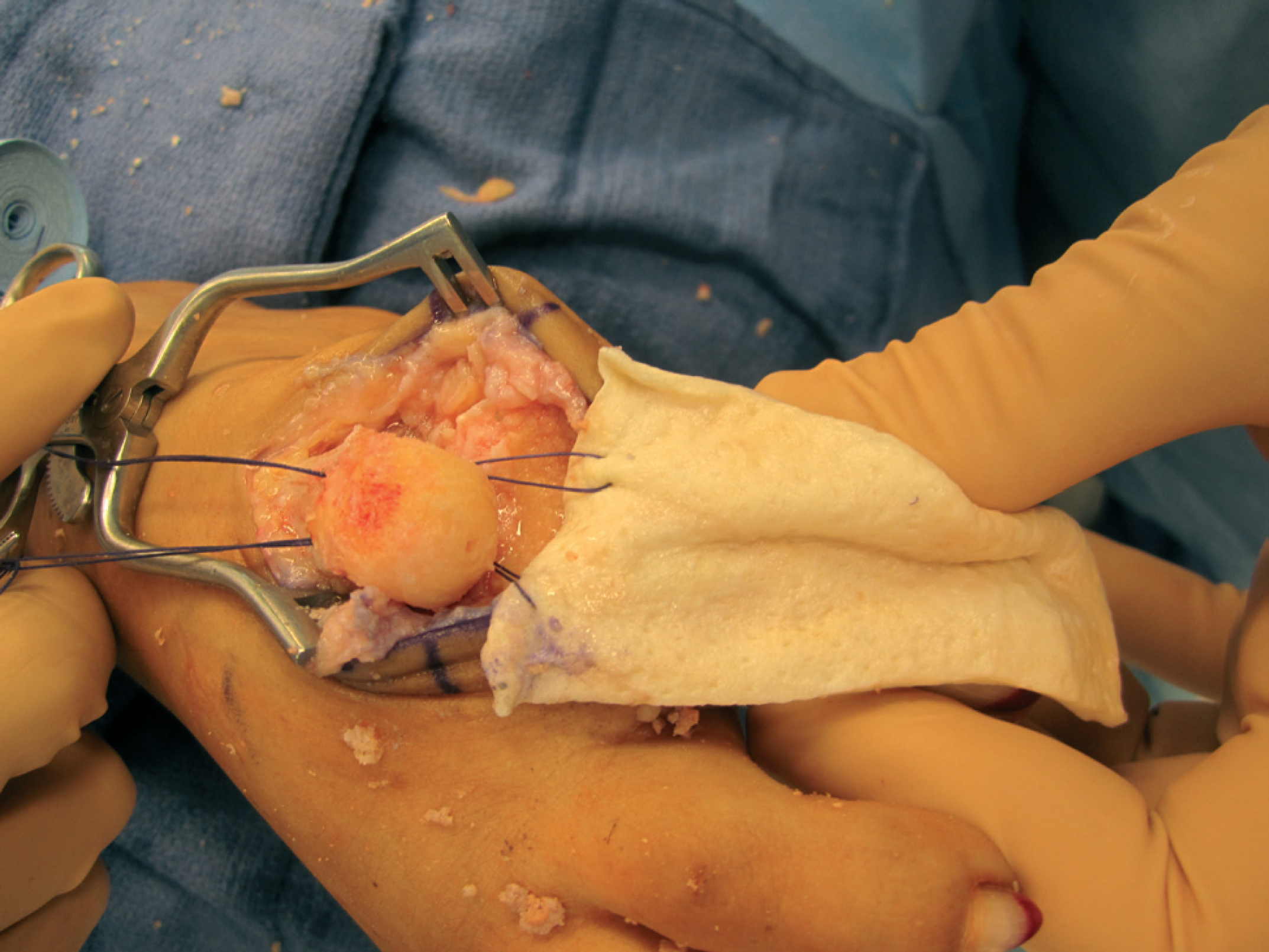
The implant is then applied to the metatarsal head. A suture passer can then be used to pull each of the 0 Vicryl sutures through the bone from plantar to dorsal (Figure 16).
A free needle is used to bring the suture through the other side of the implant on the dorsum, applying some tension to the graft to keep it secured to the metatarsal head.
A new suture of 0–0 Vicryl can be used to further secure the medial and lateral sides of the implant to itself, further securing a “cloak” or “hood” to the metatarsal head (Figure 17).
Once complete, the interposition arthroplasty should be tested in dorsiflexion to at least 60 degrees.
The wound should be irrigated well and then the capsule closed with 2–0 Vicryl. The subcutaneous closure is typically with 4–0 Vicryl and the skin with interrupted 4–0 Monocryl horizontal sutures.
The foot is dressed with a soft compressive dressing (4 × 4 gauze and Coban) and placed in a postoperative shoe.
Two days of elevation is encouraged with frequent application of ice to the foot. Weightbearing as tolerated is allowed in the postop shoe.
The patient is seen at 7 to 10 days post-op and the dressing changed. A progressive wean to regular sandals and then shoes is encouraged. The patient is encouraged to range the toe, especially in dorsiflexion to pain tolerance.

The entire head is exposed. The dorsal one-third of metatarsal head is removed with a chisel.
The medial eminence just medial to the sagittal groove and prominent lateral osteophytes are also resected.

The guide pin is placed in the metatarsal head and an appropriate sized reamer used, usually 18 mm.
A, The guide wire is placed in the dorsal one-quarter of the phalanx and angled plantarly.
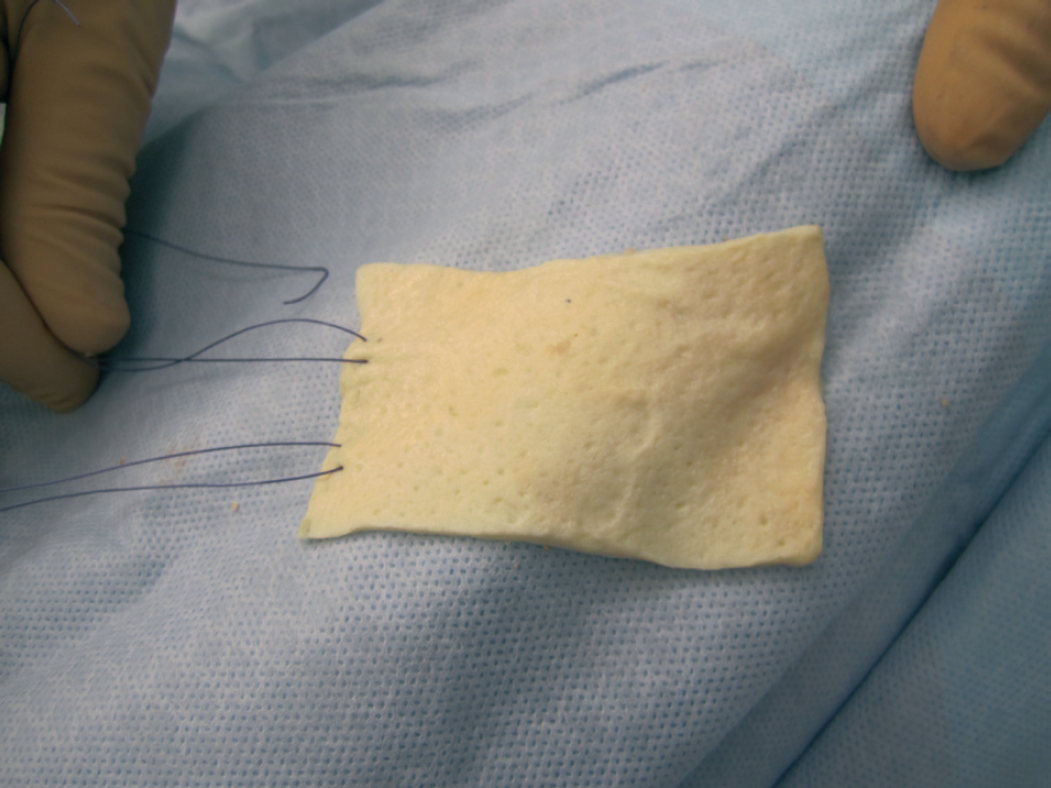
The implant is then prepared by placing two sutures of 0 Vicryl in the base.

Drill holes created in the metatarsal neck to allow passage of suture passer. Place holes from dorsal to plantar, the proximal aspect of which should be proximal to the sesamoids.
Sutures pulled through in order to fix graft to the metatarsal head.
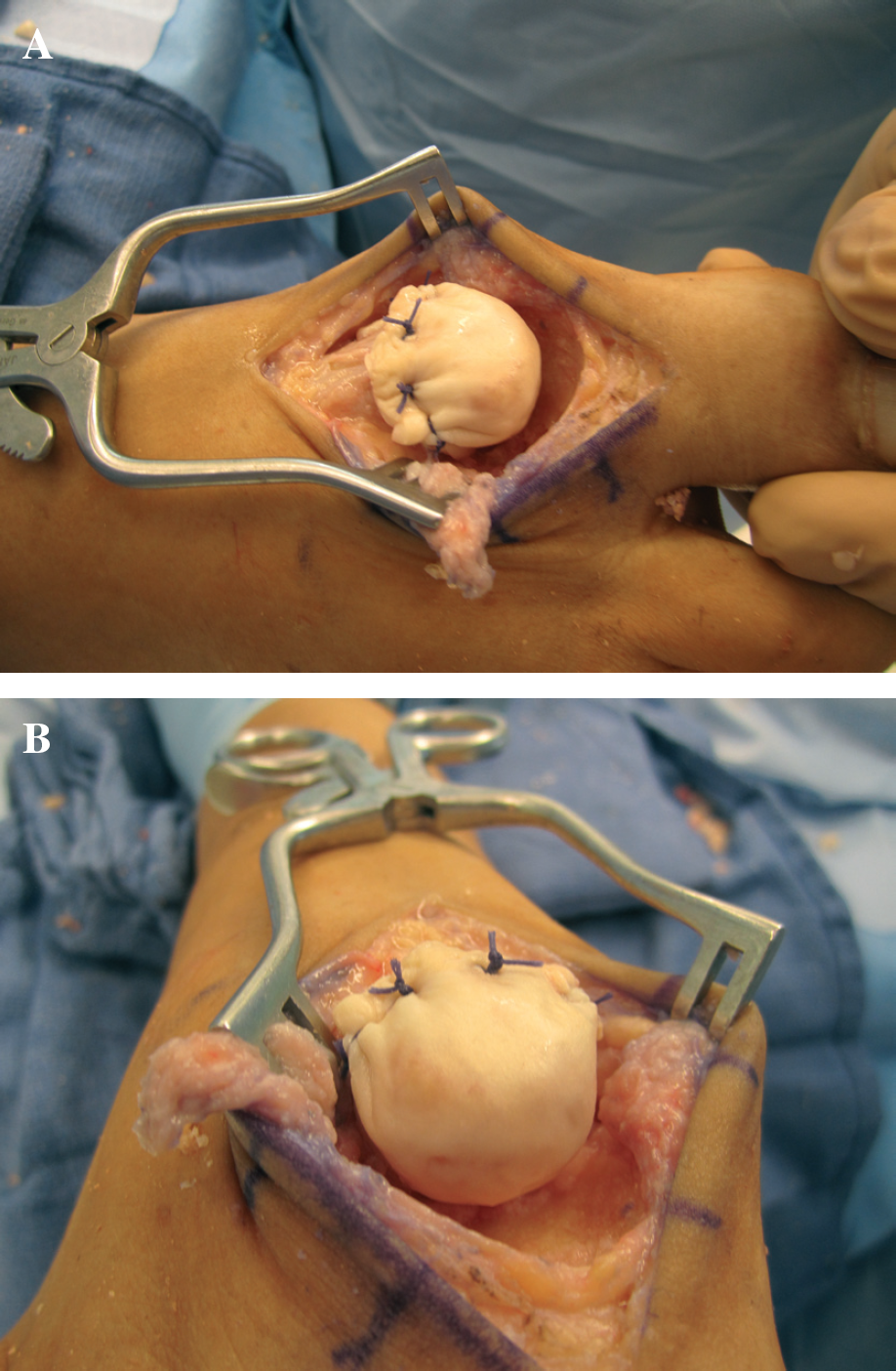
Graft is secured to the medial and lateral sides of the implant to itself (A), further securing a “cloak” or “hood” to the metatarsal head (B).
Hyer et al. conducted a Level IV case series of six patients who underwent a regenerative tissue matrix inter-positional arthroplasty of the first MTP joint using the technique described above. No patient had a subsequent fusion or additional procedure performed on their first MTP joint. Average preoperative AOFAS scores were 38, modified specifically for pain and function. Average postoperative AOFAS scores were 65.8, out of a total possible score of 68 points. All patients were satisfied with their results. The authors concluded that interpositional arthroplasty of the first MTP joint using a regenerative tissue matrix lead to reliable pain relief, preserved function, and patient satisfaction at an average 5.4-year followup in six patients. 14
CONCLUSION
Patients who fail conservative measures in the treatment of hallux rigidus can be treated surgically, depending on which stage of hallux rigidus is present. Treatment options are either joint sparing or joint sacrificing. Cheilectomy remains the gold standard in the treatment for the early stages of hallux rigidus. Research has supported the use of cheilectomy in combination with a proximal phalangeal osteotomy, which increases hallux range of motion. First metatarsal osteotomies have been described, but long-term data yields increased risks of complications. Patients suffering from advanced stages of hallux rigidus may be treated with a joint sacrificing procedure, an alternative to arthrodesis and implant arthroplasty. Interpositional arthroplasty has shown excellent results for hallux rigidus that may not be amenable to joint sparing techniques, while preserving motion of the first metatarsophalangeal joint. The Regenerative Tissue Matrix inter-positional arthroplasty, is an ideal technique for cases of severe hallux rigidus in the setting of sesamoid pain, and has yielded successful short-term results. Treatment options for hallux rigidus are based upon the patient's clinical stage and functional status and definitive treatment should be individualized.