
Abstract
Background: Chronic lateral ankle instability is a condition of perception of giving way and persistent pain usually following multiple ankle sprains. Open reconstructive procedures carry the disadvantages of subtalar joint stiffness and potential morbidity at the harvesting site. Recently, arthroscopic treatment of chronic lateral ankle instability has been proposed in order to minimize invasiveness, reduce operating time, and allow a faster rehabilitation period. The purpose of our paper was to assess the outcomes in terms of postoperative recovery and return to sport following arthroscopic reconstruction of lateral ankle instability. Methods: Ninety patients with chronic lateral ankle instability were treated at our Department from 2004 to 2009. Mean age was 32.4 (range, 17 to 56) years. All patients underwent a four-step operative procedure, including: synovectomy, debridement of ATFL lesion borders, capsular shrinkage, and 21-day immobilization and nonweightbearing. Results: Followup examination at an average of 4 years after surgery showed significant improvement of mean AOFAS scale (preoperative, 63.5; postoperative, 92.3; p < 0.001) and average Karlsson score (preoperative, 61.8; postoperative, 88.4; p < 0.001). Mean Tegner rating changed from 3.6 preoperatively to 4.9 at followup (p < 0.001). Articular stability as assessed by Sefton scale significantly improved from a preoperative value of 4.0 to 1.8 (p < 0.001). Most patients (96.6%) rated the success of their surgery as good to excellent. Conclusion: Based on our results, we propose arthroscopic treatment as a suitable option for moderate chronic ankle joint laxity in patients with a complete ATFL lesion.
Level of Evidence: IV, Retrospective Cohort Study
INTRODUCTION
Ankle inversion sprains are common injuries in sports, and are frequently treated nonoperatively. 36 However, for 10% to 40% of cases, they are responsible for chronic lateral ankle instability. 34,55 Usually the anterior talofibular ligament (ATFL) is involved, 54 and a positive anterior drawer sign is a common finding. 23 Lesions affecting the calcaneofibular ligament (CFL), which are less frequent, 54 are responsible for a positive talar tilt test. 23 Nonoperative treatment consists of physical therapy, proprioceptive training, and bracing. If symptoms persist, surgical stabilization may be indicated. Several surgical procedures exist for the treatment of the unstable ankle.
Non-anatomic tenodesis techniques were widely used in the past. 43,45 Anatomic reconstruction of the damaged lateral ankle ligament according to the Broström technique 8 and its modification according to Gould 26 have achieved high success rates. 7,18 Tenodesis techniques which aim to anatomically restore the lateral ankle ligament complex using autografts or allografts have been proposed. 1,10,13,47 However, reconstructive open procedures carry the disadvantages of subtalar joint stiffness 12,37,42 and potential morbidity at the harvesting site. 3
Recently, arthroscopic treatment of chronic lateral ankle instability has been proposed in order to minimize invasiveness, reduce operating time and allow a faster rehabilitation period with an earlier return to work. 5,15,29,31,35,38 Arthroscopic thermal assisted capsular shrinkage is an option for the treatment of functional joint instability. Thermal energy, provided by radiofrequency and laser, produces an effective reduction in capsular volume and joint translation by shortening collagenous structures within the connective tissue. 2
The role of arthroscopy as a definitive therapeutic approach in the treatment of chronic ankle instability has been reported. 5,15,29,31,35,38 The ATFL is continuous with the joint capsule and, therefore, is readily accessible during ankle arthroscopy. Some surgeons adopted arthroscopic thermal-assisted capsular shrinkage for the treatment of functional instability. This condition, as opposed to mechanical instability, refers to a situation of subjective giving-way, persistent pain, and inability without anatomic ligamentous incompetence. 21 In fact, in most studies, the procedure has been reserved for the cases where the ATFL was attenuated, not avulsed. 5,15 Advantages of arthroscopic procedures compared to open techniques are the reduced invasiveness and surgical morbidity, less operating time and quick return to work and leisure activities. 52
The purpose of our paper was to evaluate arthroscopic treatment of chronic lateral ankle instability, assessing the outcomes in terms of postoperative recovery and return to sport. We present a four-step protocol consisting of synovectomy, ATFL remnant debridement, capsular shrinkage followed by immobilization, and bracing. Our hypothesis was that arthroscopic treatment would lead to a high success rate in patients affected by chronic lateral ankle instability with complete ATFL tear.
MATERIALS AND METHODS
Patients recruitment
We evaluated a continuous series of 90 patients with chronic lateral ankle instability treated at our Department from 2000 to 2009. Operative treatment was proposed to subjects with ankle giving-way symptoms unresponsive to at least 6 months of nonoperative treatment including physical therapy and proprioceptive training. Only patients with positive anterior drawer sign were enrolled. Associated presence of a positive talar tilt test was an exclusion criterion. Both anterior drawer and talar tilt tests were performed manually by the same investigator. The test was considered either positive (maximum manual translation more than 5 mm) or negative (manual translation less than 5 mm). Magnetic resonance imaging (MRI) scans were taken in order to document the occurrence of a past sprain. The finding of an either thickened or attenuated ATFL was considered compatible with a traumatic basis of the disease.
All the operations were performed by the same experienced senior surgeon (A.V.). Fifty-two were male and 38 female. Mean age at surgery was 32.4 (range, 17 to 56) years. The right side was involved in 56 cases, the left ankle in 34 cases. All subjects met the following inclusion criteria: age 18 to 45 years, absence of previous ankle surgery, absence of multiple ligament insufficiency, and cartilage defects less than Grade III according to Outerbridge. 39 Thirty-nine patients practiced contact sports at the time of surgery (martial arts, rugby, soccer, basketball, etc), 42 non-contact sports (running, swimming, tennis, etc). Twenty-three practiced sport at competitive level, 68 were amateurs. Nine subjects were sedentary.
Surgical technique
Arthroscopies were performed under regional anesthesia (bier-block) with patients supine on the operating table and with slight elevation of the ipsilateral buttock. A tourniquet was positioned around the upper thigh. A standard anteromedial portal was established medial to the tibialis anterior tendon; an anterolateral portal was placed lateral to the extensor digitorum communis tendon, with care taken to avoiding the superficial branch of the peroneal nerve. No joint distraction was applied.
Preliminary arthroscopic inspection was performed with a 4.0-mm 30-degree scope in order to confirm the diagnosis and to detect the presence of any concomitant synovitis, cartilage, or ligament injury. Attention was then given to the assessment of the ATFL. Patients were excluded from the study when intraoperative findings did not match inclusion criteria.
Cartilage defects (grade I or II chondral lesions according to Outerbridge) were treated with the use of a motorized 4.0-mm shaver (Tomcat, Stryker Endoscopy, San Jose, CA; Formula, Stryker Endoscopy, San Jose, CA).
Associate procedures, such as removal of loose bodies or osteophytes, were performed if required.
Synovectomy was performed for hypertrophic or hemorraghic synovitis. The shaver then addressed the ATFL lesion borders in order to debride the ligament remnants.
The VAPR system (Mitek, Westwood, MA) was used to perform all thermal capsular shrinkage procedures. VAPR T Side Effect Thermal Electrode with a 3.5-mm tip at dessication mode was used with a temperature setting of 70°C and maximum power of 50 W.
The shrinkage procedure was performed with the ankle placed in an everted position starting at the ATFL remnants and progressing onto the adjacent capsule. The probe was swept serially until all the area was treated based on visual observation of the macroscopic tissue contraction. The thermal probe was then directed from the posterolateral to the anterolateral aspect toward the capsule with a constant sweeping motion in order to reduce the time of exposure and the stress applied to the treated tissue.
Rehabilitation protocol
Immediately after the operation, an ankle brace was applied (Air-Stirrup, Aircast Inc., Summit, NJ). For the first 3 weeks patients were instructed to walk without weightbearing with the use of two crutches. After the removal of the brace, patients were encouraged to begin weightbearing as tolerated and instructed in physical rehabilitation protocol including proprioception and complete active and passive ankle range of motion exercises. Return to sport was permitted 12 weeks postoperatively.
Followup
Patients were examined preoperatively and followed for an average time of 4.2 (range, 1.1 to 9) years Clinical assessment included the American Orthopaedic Foot and Ankle Society (AOFAS) ankle and hindfoot scoring system, 32 Karlsson and Peterson scale, 30 Tegner activity level, 51 Sefton articular stability scale, 44 and objective examination including range of motion (ROM), anterior drawer sign, and talar tilt test. Patients were also asked to rate the success of their surgery as poor, fair, good, or excellent and to indicate if they would undergo surgery again.
Statistical analysis
Data were analyzed using the program SPSS Version 17.0 (SPSS Inc., Chicago, IL, USA). Paired t-test (two sided test and α = 0.05) was utilized to compare the preoperative and followup status. Differences with a p value less than 0.05 were considered statistically significant.
RESULTS
Two patients were excluded as they underwent further lower limb injury (one malleolar fracture, one talar fracture) that could have biased the outcomes, thus 88 ankles were considered at followup.
Three patients suffered further sprains on the operated ankle, which were treated nonoperatively. Due to persisting symptoms of giving way six months after the arthroscopic procedure, one patient required further operative treatment consisting of open tenodesis. Reoperation was considered a treatment failure.
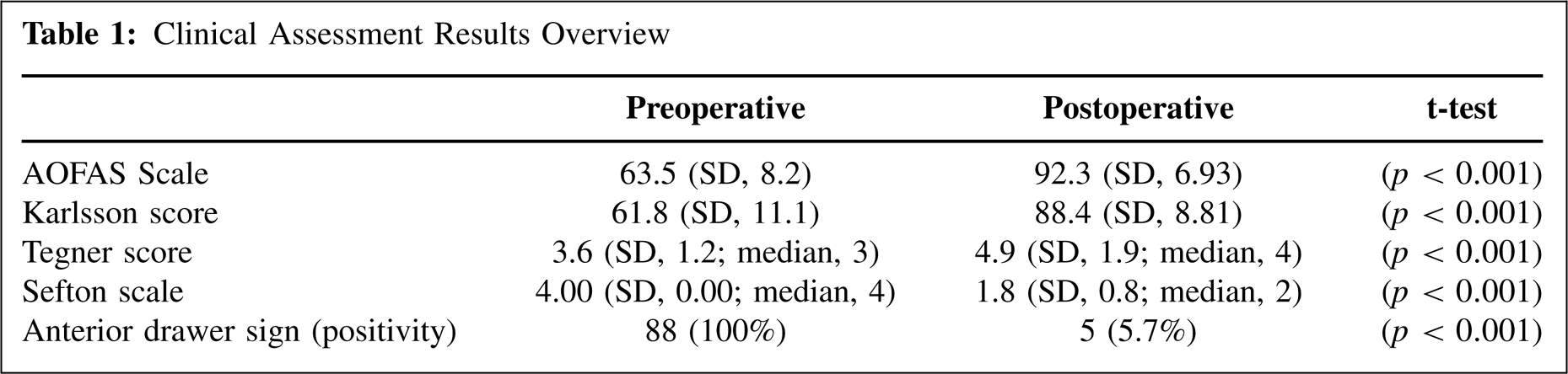
Mean Tegner, Karlsson, and AOFAS scores significant increased at followup. All patients were able to return to work. Articular stability as assessed by Sefton scale and anterior drawer sign documented a significant improvement (p < 0.001) from preoperative status. A detailed overview of the results is presented in Table 1.
Clinical Assessment Results Overview
Sagittal ROM was full in 85 cases: two patients experienced 10 degrees dorsiflexion limitations and one patient 15 degrees less compared to the contralateral side. None reported swelling. Intraoperatively, synovitis was detected in all patients (100%), chondral injuries (I to II according to Outerbridge) were observed in 72 cases (82%), loose bodies in 26% (23 patients) and ossicles were detected in 34 subjects (38.6%). Concomitant tibiotalar bony impingement was detected in 18 cases (20.4%). Mean operation time was 25 minutes (SD, 14.8)
Complications which persisted at followup were permanent altered sensation in the anterolateral aspect of the foot in five patients. Electromyography documented the presence of damage to a superficial branch of the peroneal nerve in three subjects which patients referred to as altered sensation in the anterolateral aspect of the foot. In two cases, deep peroneal injury occurred.
Eighty-five patients (96.6%) rated the success of their surgery as good to excellent. Only two patients judged the result as fair. All these patients stated they would have undergone surgery again. The outcome of the patient who underwent reoperation was considered poor.
DISCUSSION
The most important finding of the present study was that our arthroscopic four-step treatment was a valid therapeutic option for the treatment of moderate chronic ankle instability in patients with isolated, complete ATFL lesion, since we found subjective and objective clinical improvement over a period of up to 9 years after surgery.
Previous studies have shown improvement of ankle instability after arthroscopic thermal assisted capsular shrinkage (Table 2). In previous reports the shrinkage procedure has been adopted for the treatment of functional ankle instability without ligamentous incompetence, 31,38,35 and the procedure has been reserved to the cases when the ATFL was attenuated, not avulsed. 5,15,29,31,35,38 We extended arthroscopic treatment also to the condition of isolated ATFL complete tear. We proposed a four-step operative procedure including synovectomy (Figure 1A), debridement of ATFL lesion borders (Figure 1B), capsular shrinkage (Figure 1C), and immobilization and nonweightbearing for 21 days (Figure 1D).
Previous Studies of Arthroscopic Thermal Shrinkage Procedures for Chronic Ankle Instability
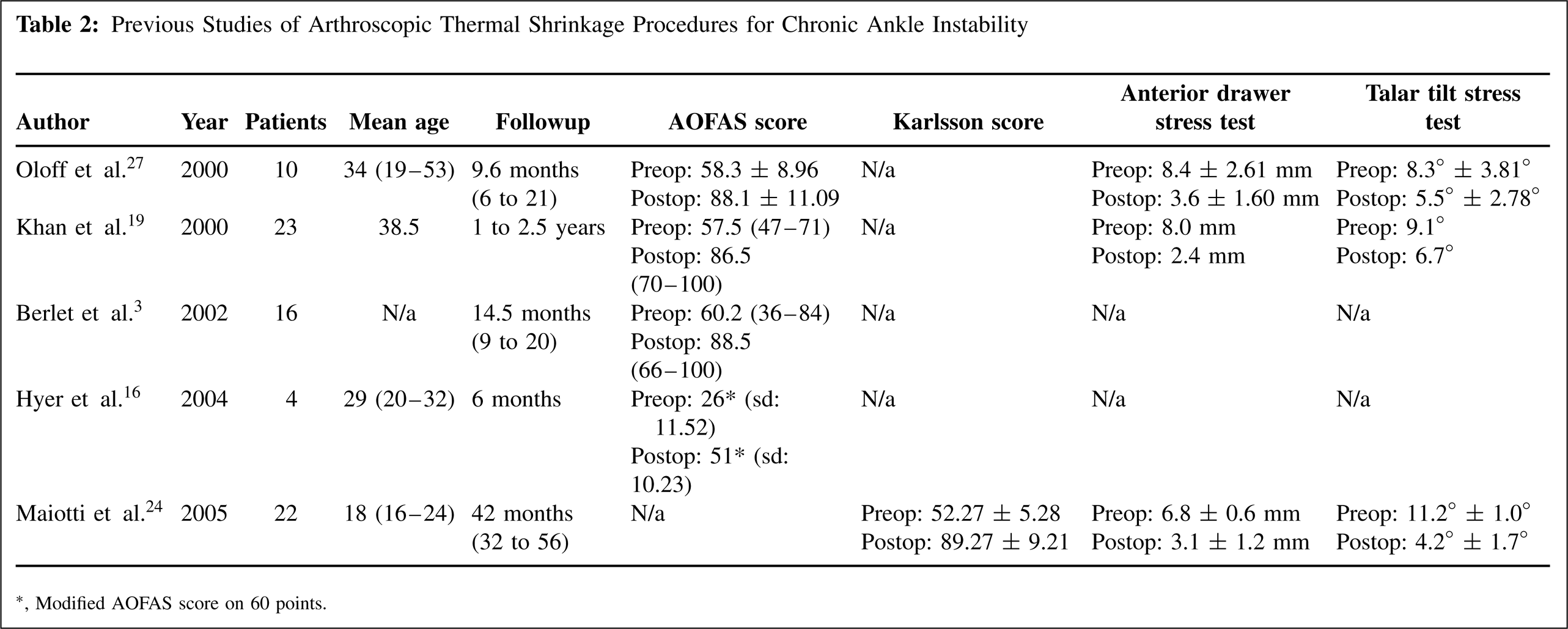
Modified AOFAS score on 60 points.
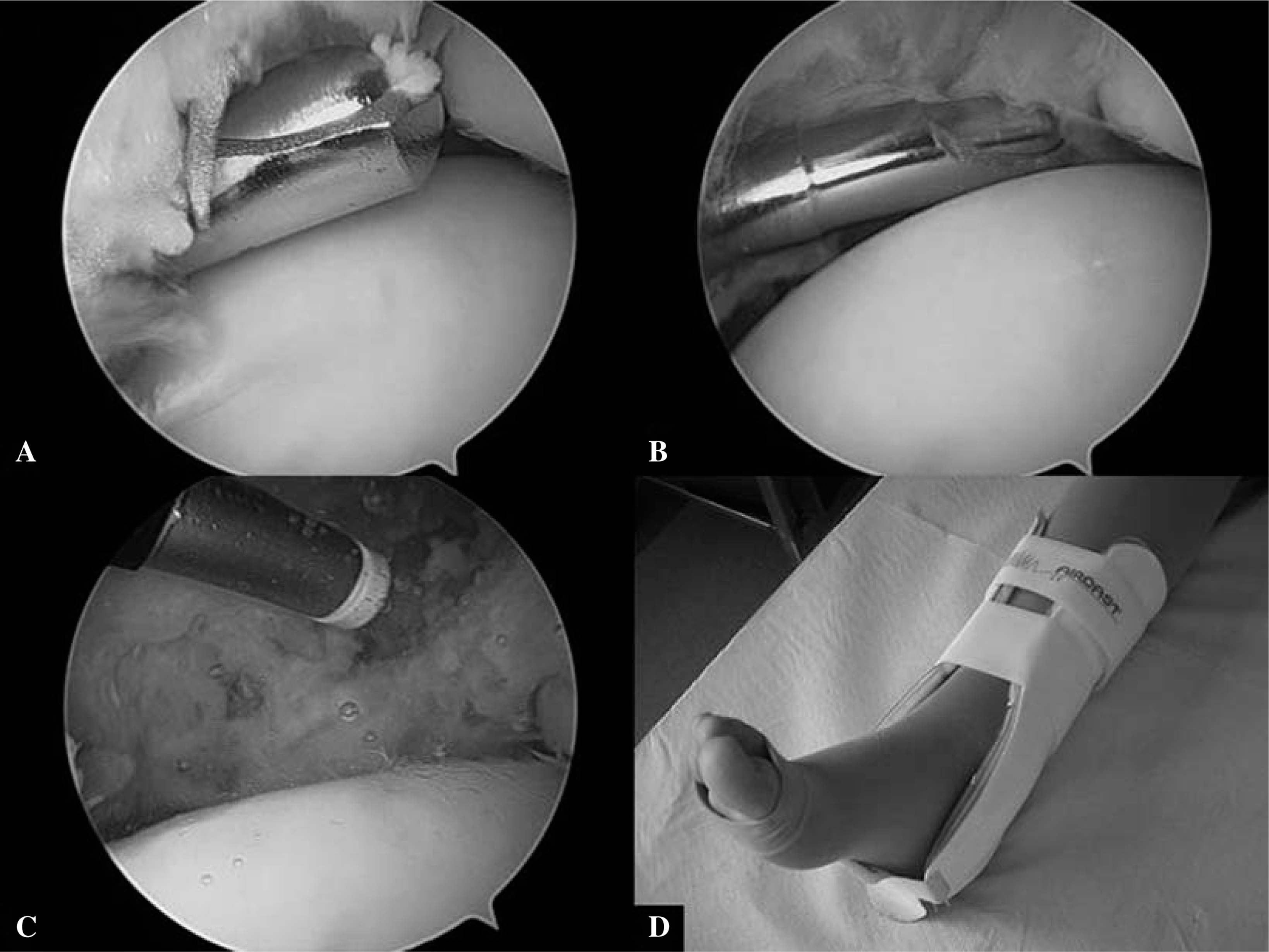
Four-step operative procedure, including: synovectomy (A), debridement of ATFL lesion borders (B), capsular shrinkage (C), and immobilization and nonweightbearing for 21 days (D).
Synovitis is often characterized by swelling of the ankle joint, with or without associated pain, and a feeling of constant or periodic discomfort. In the ankle affected by chronic instability, synovitis is a common finding as it represents the reaction to an injury of the lateral ligament complex. 4 In our case series, synovitis was detected and treated in all patients, demonstrating a strong association between instability and synovial hypertrophy. Apart from treating synovitis itself, arthroscopic debridement permits better visualization and allows treatment of the underlying factors responsible for the inflammation of the synovial lining (soft-tissue injuries, osseous pathology or degenerative arthritis). 4
Among the lateral ankle ligaments, the ATFL is the only one which is continuous with the joint capsule and therefore is easily accessible during arthroscopy. 49 The resection of the borders of the avulsed ligament and the debridement of the adjacent area allow the stimulation of fibrous tissue formation and enhancement of the healing process of the surrounding capsule. In this way they act in the same fashion as in the debridement of cartilage lesions. 17 In our case series, most patients reported complete ATFL tears. Thus in the majority of cases the ligament remnants and the adjacent capsule were debrided, and the tissue around the defect created by the ATFL tear was subjected to capsular shrinkage (Figure 2).
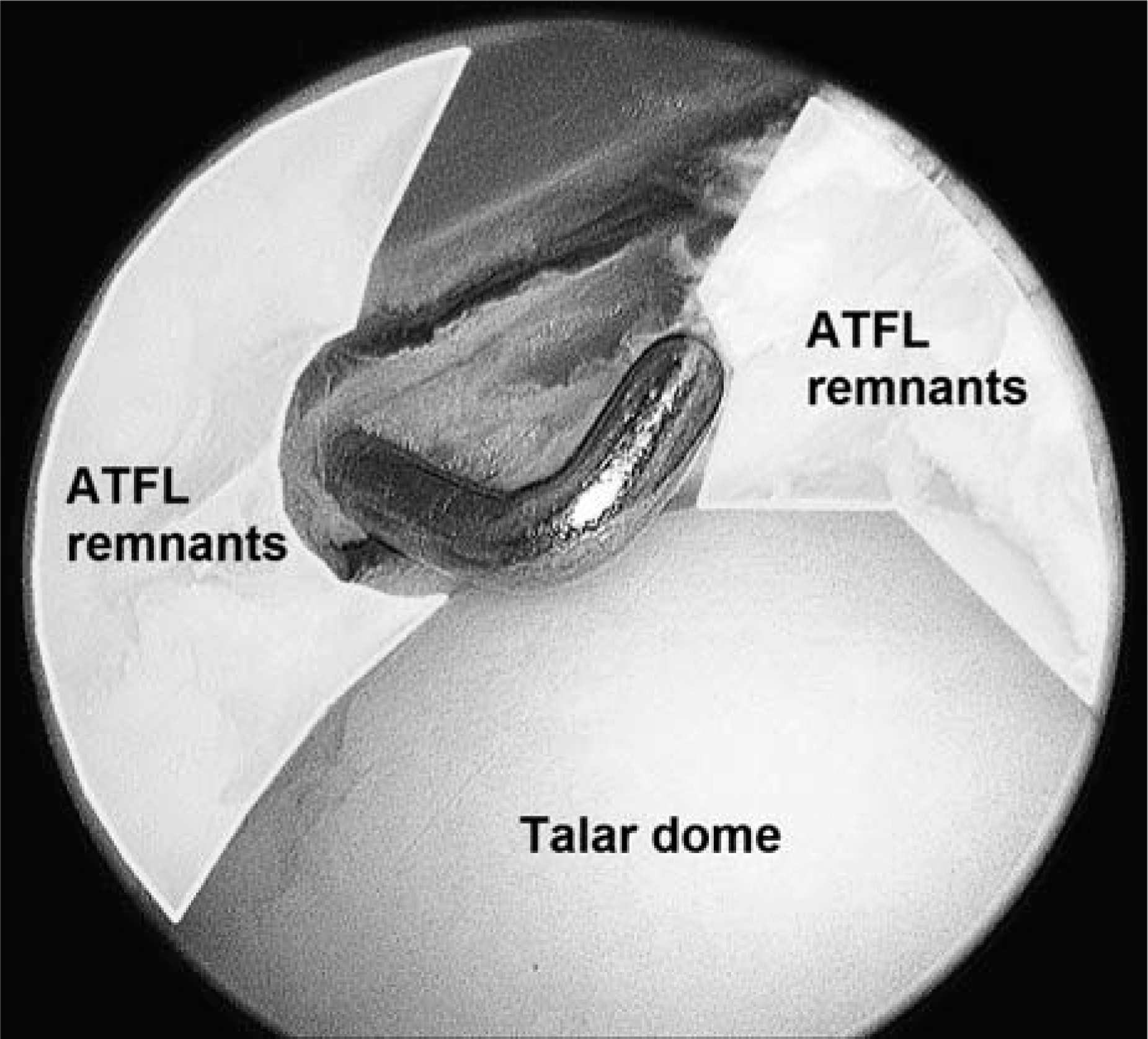
Diagram showing the area (enlightened) subjected to debridement and thermal shrinkage.
Thermal energy, provided by radiofrequency and laser, produces an effective reduction in capsular volume and joint translation by shortening collagenous structures within the connective tissue. 2 The shortening of collagenous fibers within the connective tissue leads to an effective reduction in capsular volume and allows enhanced joint stability. 11,33 In order to obtain denaturation of collagen with subsequent shrinkage of the fibers, the optimal temperature range required should be 65°C to 70°C. 20
The use of thermal energy has been employed in the capsular shrinkage of the glenohumeral joint capsule for the treatment of shoulder instability. Although initial results were promising, high failure rates and chondrolysis have been reported. 25,53 In our practice, in order to avoid potential deleterious effect of temperature on chondrocyte viability and the potential full thickness loss of articular cartilage secondary to inappropriately high power settings, we recommend using the lowest possible temperature required to afford the desired surgical result. 31
Our rehabilitation protocol consisted of brace immobilization in a neutral position with nonweightbearing for 3 weeks. Other studies have had patients nonweightbearing for 2 to 3 weeks. 5,29,31,35 An exception is de Vries et al. 15 used a compression bandage only for 3 to 5 days and early weightbearing was allowed 5 to 7 days postoperatively. Immobilization with cast or brace and nonweightbearing are important in order to prevent lengthening of the treated tissue and to allow the healing and reconstitution process to occur unimpeded. 5,11 Patients should be instructed to avoid premature return to sport activity that could affect the outcome and lead to ankle instability.
Three patients experienced dorsiflexion stiffness. Articular stiffness in these cases was related to prolonged brace immobilization and delayed functional rehabilitation program.
In our patient group the positive results observed in subjective perception and functional scales were also confirmed by objective examination. At final followup, all patients reported a reduction of pain and functional improvement. These results are in agreement with previously reported results. 5,15,29,31,35,38
Intra-articular abnormalities are responsible for ankle pain and swelling and are frequently present in conjunction with chronic ankle instability. 16,48 Arthroscopy alone or in association with open procedures allows their treatment along with ligament stabilization. 27
Chondral injuries (I to II according to Outerbridge) were observed in 82% of patients. Similarly Taga et al. found chondral injuries in 95% of ankles with lateral instability. 46 Since we excluded patients with chondral injuries greater than Grade 2 according to Outerbridge, we actually had a higher percentage of patients with cartilage lesion of the talus.
Tibiotalar bony impingement was detected in one fifth of patients. An association between lateral ankle instability and tibiotalar bony impingement has been previously reported. 8
Reports concerning arthroscopic treatment of ankle instability routinely have made use of joint distraction. 9 In contrast, performing ankle arthroscopy without joint distraction allows the surgeon to fully dorsiflex the ankle joint by leaning against the patient's foot. 52 Dorsiflexion expands the anterior working area and allows easier access to anterolateral ankle problems and to remove loose bodies and osteophytes which are usually located in the anterior compartment of the ankle joint. 52 Similarly, although the use of a 2.7-mm diameter arthroscope has been previously reported, 9 we found that the ankle joint was easily addressed using a regular diameter 4.0-mm scope.
The complication rate has been found to be 9% with ankle arthroscopy, with neurologic injury being the most common occurrence. 19 We reported five cases (5.7%) of surgery-related complications which persisted at followup: damage to a superficial branch of the peroneal nerve in three subjects and deep peroneal injury in two cases. However, these complications did not adversely affect the overall functional outcome.
Deep peroneal nerve injury can be related to capsular penetration following anterior orientation of a motorized shaver during synovectomy. 41 Alternatively it can result from malpositioning of the trochar prior to joint penetration. To try to prevent neurologic injuries, it is important to carefully consider neural structures close to the ankle joint capsule.
Due to persistent symptoms of giving way 6 months after our arthroscopic procedure, one patient required an open tenodesis with a long extensor tendon allograft. This technique was an option after failed arthroscopic treatment, as it allowed restoration of ankle function avoiding potential morbidity at the harvesting site.
Such an arthroscopic approach requires highly selective indications as proper selection of eligible patients is crucial. However, the wide range of values in normal and injured ankles makes manual laxity tests inadequate to diagnose chronic ankle instability. A previous study has found that anterior drawer sign has a sensitivity of 50% and talar tilt test of only 36%. 24 Thus manual tests are reliable in identifying ankle instability, since specificity of both is 100%, 24 but they are not able to exclude the presence of ligament injury. Instrumented anterior ankle testing devices have been found unreliable in detecting increased ligament laxity. 14 Also talar tilt and anterior drawer stress X-rays are not reliable enough in the diagnosis of lateral ankle instability 28 and their diagnostic accuracy precludes their routine use. 22
MRI can provide useful information on the integrity of the ATFL, CFL, muscle tendon units and cartilage lesions on the talar dome. However, 2D MRI images in most cases of chronic instability do not assess precisely the extent of the ligament lesion and do not give information on the degree of joint instability. 40,50 This lack of reliable diagnostic instruments makes arthroscopy quite helpful as it offers the surgeon the possibility of making a diagnosis.
Although our observational cohort study lacks a control group, the followup of up to 9 years and the number of patients to our knowledge are greater than in any other paper addressing the same issue.
In conclusion, we believe arthroscopic thermal assisted capsular shrinkage itself to be insufficient for the treatment of chronic ankle instability with an ATFL lesion. On the basis of our results, we propose our four-step arthroscopic treatment as a suitable option to treat moderate chronic ankle laxity in patients with a complete ATFL lesion. Such an approach has multiple advantages in comparison to common open reconstructive techniques (low complication rate, less operative time, no donor site morbidity) and offers similar results compared to those obtained with more invasive procedures.