
Abstract

INTRODUCTION
As 63% of the patients with ankle joint arthritis present with a malaligned hindfoot, 12 supramalleolar osteotomies have gained increasing popularity for the treatment of early- and midstage arthritis. Supramalleolar alignment correction in the varus and valgus type arthritis of the ankle joint (asymmetric arthritis) has shown to reduce pain, improve function and radiological signs of arthritis, as well as postpone fusion or the need for replacement surgery. 1,6,9,10 However, recent studies indicate that asymmetric arthritis of the ankle joint in a majority of cases is not only due to a single plane deformity, but may include a complex instability pattern involving the ankle joint, the neighboring joints and the stabilizing surrounding soft tissues. 3,4,6,7,10 Therefore, these patients may require a correction of the angle of the distal tibial articular joint surface (TAS) but they may also need additional procedures to the adjacent joints, ligaments and tendons.
AIMS OF SUPRAMALLEOLAR OSTEOTOMIES
Ankle joint malalignment leads to a focal static and a dynamic overload within the ankle joint. While standing, the center of force transmission is medialized in the varus ankle and lateralized in a valgus ankle (Figure 1). The forces within the joint are amplified by activation of the triceps surae: the Achilles tendon becomes an invertor in varus deformities and an evertor in valgus deformities, respectively, and thereby acts as an additional deforming force on the hindfoot (Figure 2). Therefore, the aims of a supramalleolar osteotomy are to (1) realign the hindfoot, (2) transfer the ankle joint under the weightbearing axis and (3) normalize the direction of the force vector of the triceps surae.

Illustration of the increased force (F) transfer in the medial aspect of an ankle with a varus malaligned distal tibial articular surface angle.
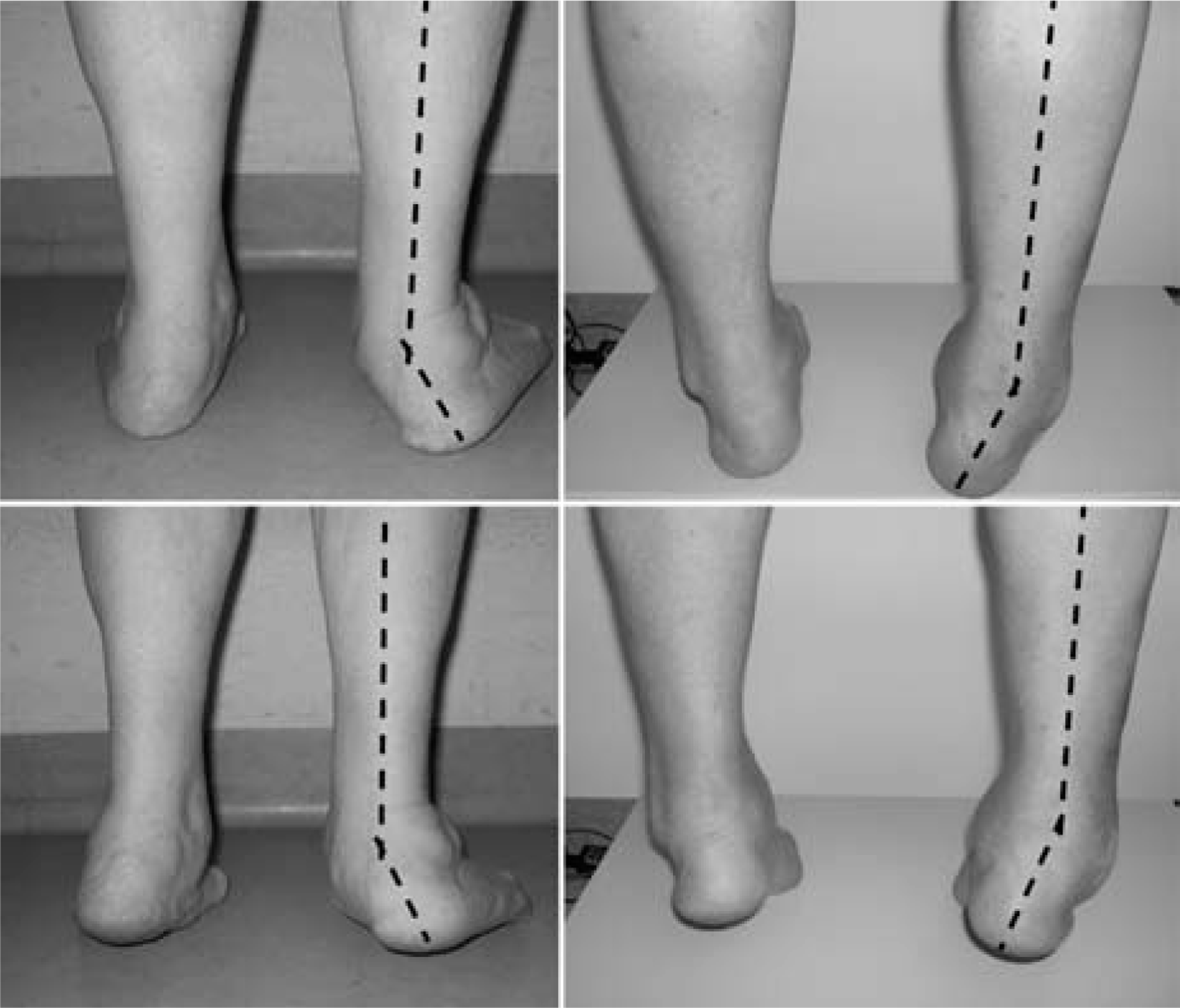
Clinical examples of a valgus (left) and a varus (right) malaligned hindfoot illustrating the aggravation of the deformity due to the force of the triceps surae when the patient rises into a tip-toe position.
ANATOMICAL AND BIOMECHANICAL BACKGROUND
The ankle joint consists of three bones: the tibia, the fibula and the talus. These bones are held together by a complex ligamentous apparatus, maintaining tight joint contact throughout the entire range of motion. Therefore the principles of corrective osteotomies of the proximal tibia, i.e. high tibial osteotomies, cannot be transferred to corrections of the ankle. In contrast to corrections of the proximal tibial articular joint surface, an isolated correction of the TAS angle may not lead to normalization of the load distribution within the ankle joint. The reason for this lies in the high congruency of the ankle joint: the fibula and the surrounding soft tissues may prevent the talus from following the tibia when changing the TAS angle (Figure 3). 8 As a consequence, an acute change of the TAS can lead to a paradoxical shift of the load; medial shifts in ankles with valgus deformity and lateral shifts in ankles with a varus deformity have been observed. 4 Furthermore, ex vivo studies have shown that changes of the TAS angle shift the load transfer not only in a medio-lateral but also in an antero-posterior direction. 4,5 Therefore the assessment of asymmetric ankle joint arthritis and the planning of corrective measures must include both the sagittal and the coronal plane.

Intraoperative images of a patient undergoing corrective osteotomy for valgus malalignment. After correction of the distal tibial articular suface angle (medial closing wedge osteotomy) the talus remains tilted / lateralized in the mortise (left) and joint congruency is not restored until the length and position of the fibula is corrected (right).
Next to malalignment, ligamentous instability has been shown to be a major risk factor for the development of ankle joint arthritis. 12 Different types of instability patterns can occur around the ankle joint. It is important to distinguish between isolated ankle joint instability and instability patterns involving not only the ankle joint but also the subtalar joint and / or the talonavicular joint. This ‘balance board instability' may lead to a complex peritalar instability pattern (Figure 4).

SPECT-CT image of a patient with a ‘zig-zag’ deformity due to destabilization of the peritalar joints: tibotalar valgus tilt, subtalar varus tilt.
SURGICAL TECHNIQUE
In case of anterior ankle impingement, advanced stages of arthritis (Takakura stage 3) and ankle joint instability, surgical reconstruction is begun with an ankle arthroscopy.
Next, the axis of the distal tibia is corrected with a supramalleolar osteotomy. Varus feet are addressed with a medial opening wedge osteotomy or a lateral closing wedge osteotomy. Valgus feet are corrected with a medial closing wedge osteotomy. 2,3 If the talus is extruded anteriorly out of the mortise, the correction is conducted in a biplanar fashion, e. g. additional anterior opening or posterior closing wedge, to improve talar coverage in the anteroposterior direction. 1 In all osteotomies, the aim is an overcorrection of the TAS angle of 3 to 5 degrees.
After completion of the tibial osteotomy, the ankle mortise is checked under fluoroscopy. In case of joint incongruence due to an inadequate length / position of the fibula, or if the talus did not follow the medial malleolus, the fibula is osteotomized and the position and length of the fibula adjusted (Figure 3).
After the supramalleolar correction, the alignment of the heel is reassessed clinically. The aim is to achieve a heel with 1 to 5 degrees valgus. The remaining deformity is addressed with an osteotomy of the calcaneus. In tilted ankles, the indication for an additional calcaneal osteotomy is set more aggressively.
Ankle instability is addressed using ligament reconstruction. Reconstruction consists of ligament suture and augmentation with the extensor retinaculum. In cases with a flattened longitudinal arch, corrective fusions (naviculo-cuneiform joints) or plantarflexion osteotomies (medial cuneiform or first metatarsal) are performed (valgus feet). 3
RISK FACTORS FOR FAILURE
Advanced stages of arthritis, ankle joint instability and joint incongruency are the main risk factors for early failures after alignment surgery. Particularly ankle varus with the talus additionally tilted within the mortise and degenerative changes located in the medial gutter has been found to lead to inferior outcome. 11 Inadequate position / length of the fibula after isolated correction of the TAS is another main risk factor.
CONCLUSION
A majority of patients with post-traumatic arthritis of the ankle joint present with a malaligned hindfoot. Correction of supramalleolar malalignment helps normalize the intra-articular load distribution and thereby diminishes excessive asymmetric cartilage load. Furthermore, correction of the hindfoot axis prepares the alignment of the ankle joint for a second surgery. For example, fusion or joint replacement procedures are known to profit from a well-aligned hindfoot.
However, due to the complex nature of the ankle joint, normalization of intraarticular load distribution may not only require the correction of the distal tibial articular surface angle, but also additional procedures such as sagittal plane correction and adjustment of the fibular length and orientation.
Footnotes
ACKNOWLEDGMENT
The author wishes to thank Lilianna Bolliger, MSc, for assistance in the preparation of this article.