
Abstract
Background: Treatment of severe ankle arthritis with varus malalignment remains controversial. Methods: In 14 consecutive total ankle replacements (TAR) with tibiotalar varus malalignment of above 15 (range, 16 to 41) degrees, a complete transfer of the tibialis anterior tendon together with other soft-tissue and bony realignment measures was added to the primary procedure. Results: After mean followup time of 33.4 (range, 21 to 49) months, only one case showed minor tibiotalar tilt in the frontal plane. The overall clinical results were good to excellent in all but two cases with an average AOFAS-score of 86.4 (range, 70 to 98) points. However, three cases of tibial nerve neuropathy due to entrapment or overtensioning were observed; one of these cases developed clinical problems with incomplete recovery. Conclusion: Tibialis anterior tendon transfer can be recommended in conjunction with TAR in cases of varus malalignment with severe muscular or ligamentous imbalance with neuropathy of the tibial nerve being the main complication.
Level of Evidence: IV, Retrospective Case Series
Keywords
INTRODUCTION
Total ankle replacement (TAR) has become more popular since the evolution of implants with three component prosthetic design. According to several authors, TAR should be confined to cases without severe deformity, 10 to 15 degrees of malalignment being regarded as the upper limit of deformity. 1,14,15,16 Edge loading, malleolar fractures, loosening and higher revision rates have been described in TAR of varus ankles. 3,5,6 Other authors, however, have reported acceptable results even in patient series with more severe varus deformity if additional surgery was performed. 2,7,8,10 Osteotomy of the tibia, fibula, medial malleolus 2 and calcaneus have been described as well as deltoid ligament release, reconstruction of the lateral ankle ligaments, tenodesis procedures with a peroneal tendon 11,13 and muscular rebalancing with the posterior tibial or peroneal tendons. There are only few remarks of tendon transfer of the tibialis anterior muscle-tendon-unit in conjunction with TAR in the literature. 4,6
The author has used tibialis anterior tendon transfer in varus ankles since 2002 and published a series of ten cases in 2007, 4 most of them having been treated by split tibialis anterior tendon transfer. Because of relapse in two very severe cases, he has transferred the complete tibialis anterior tendon since 2006 in most cases of varus ankles with severe ligamentous and/or muscular imbalance. To the authors knowledge, there is no other comparable study in the literature describing results of tibialis anterior tendon transfer as an adjunct in TAR with severe varus deformity.
MATERIALS AND METHODS
From 2002 to 2009, partial or complete tibialis anterior tendon transfer was added to TAR in 30 cases of varus ankles to restore muscular balance or to compensate for concomitant major ligamentous imbalance. None of these patients suffered from a neuromuscular disorder; the term “muscular imbalance” refers to shortening or overlengthening of muscle tendon units around the ankle caused by longstanding major deformity or attenuation of the peroneal tendons, that were, however, not recorded in detail in all of the patients. In most cases the transfer was combined with the primary total ankle replacement; in four patients it was added later in case of edge loading or inlay subluxation. The criteria for inclusion into this retrospective study were: primary TAR, preoperative varus deformity of above 15 degrees, complete transfer of the tibialis anterior tendon to the midline of the foot, followup of at least 18 months. Fourteen consecutive cases met these criteria and were included (Table I), among them one of the cases (Case 1), that was already included into the study group in 2007. 4 No patient was lost to followup. Mean followup was 33.4 (range, 21 to 49) months. All patients suffered from post-traumatic arthritis either after fracture or recurrent ankle sprains. No patient with rheumatoid arthritis was in this group. All patients included into this study gave informed consent. The study was approved by an institutional review board.
Operative technique
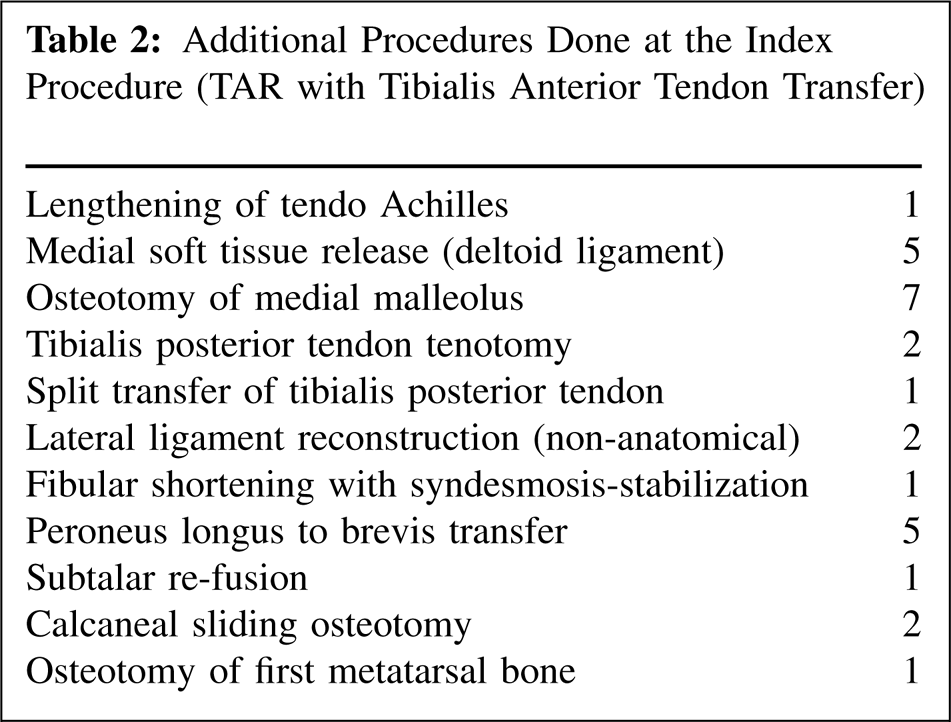
In all 14 cases a mobile-bearing STAR Ankle™-prosthesis (SBI, former LINK) was implanted as a primary procedure. Depending on the individual situation, multiple additional procedures were added (Table 2), including release of the deltoid ligament or medial malleolar osteotomy in most of the cases and transfer of peroneus longus tendon in some of the patients. Because of persistent (antero-)lateral tilting of the talar component as a sign of major ligamentous imbalance and/or malfunction of the peroneal muscles, diagnosed by preoperative muscle-testing (physical examination), tibialis anterior tendon transfer was considered and carried out. The tibialis anterior tendon was completely transected at its insertion and was transferred to the midline of the foot using the main incision; it was fixed under slight tension in a neutral position of the foot at the end of surgery, using a Biotenodesis screw (Arthrex) at the intermediate (Case 7 and 14, Table I) or lateral cuneiform bone (all the other cases), depending on the estimated tilting of the talar component. As shown in Table II further soft tissue procedures and in one case (Case 1) a split transfer of the tibialis posterior tendon were added. The tibialis posterior tendon was cut in two cases (Case 11 and 14), but was preserved in all other cases in order to prevent instability and overcorrection. In two of the patients an additional lateral ligament reconstruction was carried out (Case 13 and 14). In case of decreased dorsiflexion (10 degrees or less), a lengthening procedure at the calf muscles was added (in this group only in one case, z-lengthening of tendo Achilles in Case 14). Postoperative immobilization in a cast with partial weightbearing was continued for 6 weeks, full weightbearing was allowed at 8 weeks because of uncemented fixation of the implant.
Pre- and postoperative evaluation
Preoperative clinical evaluation included a thorough examination by the author with a special focus on ligament-stability of the ankle joint and peroneal muscle function. In cases of suspicion of partial or complete peroneal tendon rupture, imaging by ultrasound and/or MRI was added. Transfer of the tibialis anterior tendon only was considered in cases with an active and strong tibialis anterior muscle. At the followup examination, special emphasis was given to hindfoot alignment and muscle function during the swing phase of gait. Postoperative strength of the tibialis anterior muscle was not calculated exactly as other muscle units assist in dorsiflexion and isolated testing is not easy after transfer of the tendon; however, the muscle belly of the tibialis anterior muscle was palpated and overall power in dorsiflexion was monitored by physical examination. Global foot function was measured with the AOFAS score. Additionally, the exact range of motion of the upper ankle joint, walking distance, capability to walk on the forefoot and to climb up and down stairs with both legs alternately was recorded. Last, the patient was asked to which extent (in percent) his former foot problem (100%) appeared to be solved from his own point of view.
Radiologic evaluation
Pre- and postoperative AP and lateral X-rays in a weightbearing condition were analyzed. The tibio-talar alignment (TTA, “ankle alignment” according to Kim et al., 10 i.e., angle formed by the longitudinal axis of the distal tibia and talar surface in the AP-view, see Figure 1B) and talar tilt (TT, angle formed by tibial and talar joint line or component) were measured. The definition of tibio-talar alignment (TTA) is the same used by other authors to describe angular deformity in the frontal plane. 2,8,17 Gross malalignment in the sagittal plane (lateral view), osteolytic changes at the implant-bone-interface, signs of implant loosening and cystic lesions were also recorded.
RESULTS
At the last followup, all patients had improved markedly in comparison to the preoperative status. The clinical and radiographic results are shown in Table I. The mean AOFAS-score was 86.4 (range, 70 to 98) points. The mean pain score was 31.4 (range, 25 to 40) points. The range of motion, measured with a goniometer, was 34.2 degrees on average, the walking distance recorded by the patient 5.9 km on average. All patients were able to climb up and down stairs with both legs alternately; 12 patients could walk several steps on their forefeet at followup. From the patients' point of view, 84.5% of the preoperative overall foot problem seemed to be solved.
In one patient (Case 14), a tarsal tunnel decompression was necessary three days after the index procedure because of a sensory deficit. No other patient has needed a second procedure. There was one patient (Case 8) with skin necrosis at the medial edge of the incision that healed uneventfully after 3 months. In three cases, slight hindfoot varus without deterioration over time was found on clinical examination. Function of the transferred tibialis anterior tendon was sufficient in all patients and the palpation of the muscle belly showed no sign of weakness or atrophy in any patient. In some cases, slight forefoot pronation as a result of tibialis anterior tendon transfer could be observed, especially in the swing phase of gait; however, this seemed not to be of major concern for these patients and they merely recognized it by themselves. No patient complained of muscle weakness or dropfoot gait. Although the tendon was fixed with tension in a neutral position of the ankle, there was enough plantarflexion at the follow up examination from a functional point of view (20 degree or above except one patient (Case 4), who had only 15 degree of plantarflexion). Two patients had AOFAS-scores below 80 points with a considerable amount of overall disability. One of them (Case 10) suffered from persistent tibial nerve problems (see below) and talocalcaneal arthritis, the other one (Case 13) was still painful, probably because of problems with the arthritic subtalar joint.
Patient List
In three patients, postoperative neuropathy of the tibial nerve or one of its branches was observed. The first patient (Case 10) suffered from postoperative pain after cessation of regional postoperative anesthesia and showed complete loss of sensation on the sole of his foot. He refused surgical revision of the tibial nerve. Slow, incomplete recovery of the nerve was found at the last follow up about 26 months postoperative. The overall functional result was limited markedly, which is obviously due to the nerve damage (AOFAS score 70 points, pain-score 25 points). The second patient (Case 11) presented with sensory loss on the lateral part of his sole (lateral plantar nerve) at 23 months postoperative. As this condition does not cause any discomfort to the patient, there is no need for surgical intervention up to now. The third patient (Case 14) with postoperative tibial nerve damage was revised on the third postoperative day. This patient showed an extreme amount of varus deformity (Figure 1) preoperatively (41 degrees tibio-talar angle). An entrapment phenomenon was observed and treated three days after the index procedure at the entrance of the tibial nerve below the adductor hallucis muscle, followed by slow but finally complete recovery of the sensory function of the nerve at the forefoot at follow up at 23 months. In all these three cases, direct violation of the nerve was excluded and tensioning or secondary entrapment were regarded as probable reasons. Because of this possible complication, prophylactic release of the tibial nerve now is considered in further varus cases.
Additional Procedures Done at the Index Procedure (TAR with Tibialis Anterior Tendon Transfer)

(Case 14) Severe varus deformity with major ligamentous instability and 41 degree frontal plane deformity (A to C). Tibialis anterior tendon transfer, lengthening of tendo Achilles and tibialis posterior tendon with lateral ligament reconstruction and osteotomy of the first metatarsal bone was done simultaneously with total ankle replacement. The overall clinical short-term result was very good, the radiologic result after 23 months showed full correction (D and E).

(Case 3) Pre- and postoperative X-ray 44 months after total ankle replacement with tibialis anterior and peroneus longus tendon transfer, deltoid ligament release and sliding osteotomy of the calcaneus with good clinical and radiologic result.
The radiologic evaluation was focused on the alignment in the frontal plane. The preoperative varus deformity was 23.8 (range, 16 to 41) degrees tibio-talar malalignment (TTA) on average with a talar tilt (TT) of 16.0 (range, 0 to 34) degrees on average. The group consisted of congruent and incongruent and mixed cases, as seen comparing tibio-talar malalignment and talar tilt (Table I).
The tibio-talar alignment improved from 23.8 degrees preoperative (range, 16 to 4 degrees) to 2.4 (range, 0 to 6) degrees of varus alignment. Two of the most severest cases are shown in Figure 1 and 2. Talar tilt (average 16.0 degrees preoperative) was eliminated completely in all but one patient (Case 4), who still had 3 degrees of talar tilt 41 months after surgery without progression of tilting over time. There were no signs of component loosening, radiolucent lines at the interface or gross malalignment in the sagittal plane. However, four patients had a possible cystic lesion in the talar body.
DISCUSSION
There are different pathogenic pathways that can lead to a severe varus ankle deformity. Multiple ankle sprains may cause ligamentous imbalance with subsequent degeneration of secondary restraints, especially the peroneal tendons. Peroneal muscle dysfunction (split lesion of peroneus brevis tendon and compensatory overactivity of the long peroneus muscle) may result in forefoot pronation and hindfoot varus. Pre-existing cavovarus deformity and/or asymmetric weight distribution at the upper ankle joint may contribute to varus ankle malalignment.
Correction of major varus deformity always will create a muscular imbalance because of changes in the resting length of the muscle-tendon-units of the lower leg. The preexisting condition of these muscles (weakness, atrophy) and tendons (split lesion, complete rupture, elongation) will further contribute to this imbalance. As a result, the subtalar joint complex may get into an inverted position and/or an unstable ankle joint may be driven into varus. Edge loading, increased polyethylene wear, inlay dislocation and malleolar fracture may lead to failure of the TAR. It should be mentioned here, that fusion of the upper ankle joint in severely deformed cases would necessitate restitution of muscle balance around the subtalar joint complex as well in order to achieve long-lasting realignment.
The tibialis anterior muscle predominantly is active during swing-phase of gait. Additionally, it has a decelerating effect after initial heel contact by eccentric contraction. Depending on instantaneous foot position, it produces a strong inversion force on the subtalar joint complex and the ankle joint in case of instability. In pediatric and neurologic conditions, transfer of the tibialis anterior tendon traditionally is used with good success especially if the peroneal muscles are weak. 9,12 This experience constituted the rationale to apply this procedure in TAR of severe varus ankle. Tibialis anterior tendon transfer was added in those cases of varus deformity in the presented series, where after insertion of the implant and appropriate medial release procedures (and transfer of the peroneus longus tendon in some cases) a certain amount of (antero-) lateral instability was observed. One important further criterion for the decision to transfer the tibialis anterior tendon was the condition of the peroneal tendons evaluated in the preoperative examination. In case of severe attenuation or rupture of one or both peroneal tendons, this seemed to be a strong argument for the transfer of the tibialis anterior tendon. The author stopped using split tibialis anterior tendon transfer in 2007 because of unpredictability of the outcome. In some cases the inversion power of the tibialis anterior muscle seemed not to be completely eliminated, resulting in persistent varus deformity, in some other cases only the transferred part of the muscle seemed to be active and there was some concern for overcorrection. Therefore it appeared to be superior to transfer the complete tendon, the point of insertion (intermediate or lateral cuneiform bone) influenced by its effect in clubfoot surgery.
Many authors do not recommend TAR in severe frontal plane malalignment. Wood et al. 15 published a series of 200 replacements with a mean followup of 88 months. In cases of deformity above 15 degrees (39 patients), loosening, edge-loading and late malleolar fractures were observed in a high percentage. The authors did not recommend TAR for major deformities any more.
In the literature there are several more studies dealing with results of TAR in varus malalignment, describing inferior results in comparison with neutral ankles. Not all of these studies are comparable as to the amount of preoperative deformity, because the exact angle of deformity is either not described in detail or not presented exactly; however, TTA as described above is the most common way to measure overall varus deformity in total ankle replacement. 2,8,10,17 Henricson et al. 6 reported on 55 TAR with 5 to 30 degrees preoperative varus deformity. Twenty-nine of their patients still showed some varus alignment at followup despite different bony and soft-tissue realignment procedures having been added. After a mean followup of 4.2 years, the revision rate for this group was almost twice as high as in neutral ankles. Hobson et al. 8 presented a group of 24 TAR using the same implant as in the study presented here with preoperative varus malalignment between 10 to 30 degrees without quantifying the exact average deformity. During a mean followup of 4 years, they observed a higher rate of failures in patients with more than 20 degrees of preoperative deformity, instability being the most frequent cause.
Other authors proposed different additional surgical steps to deal with ankle varus alignment. As in the study presented here, it is difficult to determine the effect of different procedures performed simultaneously. Kim et al. 10 recommended medial soft tissue release together with lateral ligament reconstruction with a Brostrom-type reinforcement in incongruent varus deformity and asymmetrical resection in case of congruent varus deformity of the distal tibial region. In their varus group (23 patients), which had less deformity (17.1 degrees preoperative deformity) than the patient group presented here, they observed 83.2 points in the AOFAS-score with no significant difference to the results in another group of patients without deformity.
Doets et al. 2 invented medial malleolar osteotomy in TAR of varus ankles. Although the 15 patients had much less severe varus malalignment (14.9 degrees in the average) in comparison to the cases described here (23.4 degrees in the average), three cases of persistent or recurring hindfoot varus deformity had to be reoperated on. In the patient group described here, medial malleolar osteotomy was added in half of the cases. It was found to be a useful procedure to rebalance ligamentous stability; concomitant muscular imbalance, however, could not be restored thereby.
Peroneus longus to brevis transfer has been recommended by some authors 6,7,10 and has been administered also in five cases here, especially in cases of preexisting forefoot pronation due to overactivity of the long peroneal muscle. Slight pronation of the forefoot due to tibialis anterior tendon transfer has been observed in some patients. Although it has had no important adverse effect so far, it may be of concern for the patient later. Probably a simultaneous transfer of the long peroneal tendon to the short peroneal tendon could be considered in conjunction with tibialis anterior tendon transfer for all patients in the future to deal with this potential adverse effect.
A clear limitation of the study presented here is the pre- and postoperative quantification of hindfoot alignment, using only standard AP X-rays in a weightbearing position and clinical assessment of hindfoot position. Neither long leg views nor Saltzman view pictures were taken. As Hobson et al. 8 remarked, measurement of lower leg alignment is a complex matter, especially in the postoperative evaluation, that might not be reflected sufficiently by the means administered here. A further limitation of the study is that the strength of the transferred tibialis anterior muscle could not be measured exactly. It is well-known that tendon transfer may result in loss of muscle strength and this may be the case in the patient group described here to a certain degree. However, it seemed not to be of clinical relevance so far.
The main complication in this study group was damage to the tibial nerve. The author's awareness of this specific complication arose during the last years and interruption of the Nervus ischiadicus pain block at the first postoperative day (“wake-up-test”) now is administered with surgical revision of the nerve, in case of any sensory loss. In extreme severe varus deformity release of the tibial nerve at the index procedure should be considered routinely. No further case of persistent tibial nerve dysfunction was observed after introducing this strategy in the 11 cases operated on since 2009. Nevertheless, patients are informed about this possible complication preoperatively.
CONCLUSION
To the author's knowledge, the patient group with ankle replacement presented here had the highest preoperative level of frontal plane deformity published so far. According to the early results, it seems possible to carry out successful TAR even in cases with major varus malalignment thereby avoiding fusion. Tibialis anterior tendon transfer which had not yet been described in combination with TAR may play an important role along with other forms of soft tissue rebalancing for these patients. However, it seems too early to establish complete guidelines especially as to the differential indication of deltoid ligament release, medial malleolar osteotomy, reinforcement of lateral ligaments and tibialis anterior tendon transfer. Furthermore a longer observation time will be necessary to evaluate the long-term effect of tibialis anterior tendon transfer as an adjunct in the treatment of varus deformity with total ankle replacement.