
Abstract
Background: The TightRope® is a relatively new device designed to stabilize ankle syndesmotic injuries. There are no studies evaluating the clinical effectiveness of this technique and few reports addressing complications and potential modifications to the surgical technique reported in this article. Materials and Methods: A retrospective review of 102 cases of traumatic ankle syndesmotic stabilization using the TightRope device is presented. Patients were followed up for a median of 85 days after surgery. Results: Eight patients subsequently had the TightRope removed. This was performed for four reasons: osteomyelitis surrounding the implant, painful aseptic osteolysis surrounding the implant, failed stabilization of the syndesmosis, and unexplained pain. Conclusions: On the basis of experience, the authors recommend meticulous attention during the surgical technique. To prevent skin irritation and stitch abscess formation leading to osteomyelitis, the FiberWire loop is best cut with a knife at least 1 cm beyond the knot, allowing the sharp end of the FiberWire to lay flat adjacent to the fibula. Painful aseptic osteolytic reaction to the TightRope necessitates removal. To prevent rediastasis, a small medial incision is recommended for endobutton positioning directly abutting the tibial cortex without soft tissue interposition. Inserting the TightRope through a fibula plate prevents lateral button pull-through and rediastasis.
Level of Evidence: IV, Retrospective Case Series
INTRODUCTION
The conventional management approach to treating unstable ankle syndesmotic injuries has been to achieve stabilization through screw fixation. 3 However, this approach has not been established beyond question with the literature supporting nonoperative management 10 and other alternative methods of surgical treatment such as fine wire ring fixators 11 and bioabsorbable screws. 7 The perceived advantage of using bioabsorbable screws is to avoid the need for a secondary operation to remove hardware transfixing the syndesmosis. Similarly, the TightRope® (Arthrex, Naples, FL) is a relatively new device, 12 which has been designed to obviate the need for hardware removal and to allow continued rotational and longitudinal movement at the distal tibiofibular joint during ankle plantarflexion and dorsiflexion. 2 Early biomechanical assessment has shown that the TightRope does provide less rigid fixation than screws and it is therefore assumed that this provides a more physiological type of healing. 8 However, no prospective, comparative studies of clinical effectiveness have been published using this technique that substantiate its efficacy.
Complications specific to the device and the surgical technique are not widely documented. However, it has been reported that proximity of the lateral knot to the skin can be troublesome, 6 that infection is associated with the implant, 1 that inflammatory responses occur in the absence of infection many months after insertion, 4,13 and that osteolysis with unexplained widening of the tibial drill tunnels can occur. 4
When assessing any new surgical technique, any potential issues of safety or complications need to be clearly documented to permit surgeons to modify the technique to improve results. The aim of this paper is to review patients with unstable ankle fractures treated with the Tightrope, specifically highlighting the complications of the procedure and how the authors suggest modifying the surgical technique to avoid them.
METHODS
Syndesmosis stabilization with the TightRope device was performed in 106 patients with 107 ankle fractures at our unit between January 2007 and December 2010. Cases were identified from surgical log books and hospital notes were reviewed. There was no record of followup for five patients who were therefore excluded, leaving 102 cases as the study group for this retrospective case review. Fifteen of the consultant trauma and orthopaedic surgeons from our department used the device during the study period, performing a median of five (range, 1 to 28) cases each.
The majority of injuries were sustained following a nonspecific twisting injury or during sporting activity. Fractures were classified using the Weber and Lauge Hansen systems: Weber C/pronation external rotation (60 cases), Weber B/supination external rotation (31 cases), and Weber B/pronation abduction (one case). Ten of the injuries were unclassifiable by this system; there were eight Maisonneuve-type syndesmotic injuries (none of which were bony), one minimally displaced pilon fracture associated with a pronation external rotation injury, and one open talus dislocation. Patients were followed up a median of 85 days after surgery, with a range of 17 to 1292 days (n = 102). The median number of days between surgery and the final radiographic followup was 71 days, with a range of 7 to 1265 days (n = 80).
The mean patient age at the time of surgery was 31 years (SD = 14), and 64 were male. Three of the injuries were open fractures (two Gustillo A and one C1), five required external fixation before definitive management by open reduction and internal fixation, and five were sustained in association with other significant injuries (polytrauma).
The median wait from initial radiographs to definitive surgery was 2 days (n = 100) with a range of 0 to 411 days. Fibula plates were used in 73 cases and lag screw fixation of the fibula fracture was used in 38 cases. Tibial screws were used in 27 cases and posterior malleolar fractures were stabilized in seven cases.
The study was approved by the Northern General Hospital Research Committee. Medians and ranges were used to describe the data when it was not distributed normally. An independent observer (senior registrar, first author) performed the classification and data collection.
RESULTS
Sixty-one patients had syndesmotic stabilization using one TightRope device, and in 41 patients, two devices were used. Sixty-one patients had the TightRope inserted through a fibular plate; eight of these were three-hole plates inserted solely to act as a washer for the fibula button. Twelve patients had a plate used to stabilize a fibula fracture but the TightRope was not inserted through the plate.
There were three cases (3%) of superficial wound infection, three cases (3%) of osteomyelitis, two cases (2%) of aseptic osteolysis surrounding the TightRope device, three cases (3%) of intraosseous migration of the lateral endobutton, and three cases (3%) with malpositioning of the medial endobutton. Ten of these 14 complications occurred in patients with Weber C/pronation external rotation injuries. At final followup, 44 patients (44%) had ankle pain, swelling, or stiffness, or combinations of the three symptoms. Two patients (2%) had nonfatal pulmonary emboli and two (2%) had symptomatic deep vein thromboses.
Three cases (3%) required further surgery for a reason unrelated to the TightRope: a delayed wound closure of an open fracture with split skin grafting, an ankle arthroscopy to assess the articular cartilage because of ongoing ankle pain, and fibular plate removal for hardware prominence.
Eight patients (8%) had the TightRope removed. Removal was performed for one of four reasons: osteomyelitis surrounding the TightRope, radiological track widening from aseptic osteolysis and pain, failed stabilization of the syndesmosis, and unexplained pain (Table 1).
Reasons for TightRope Removal (n = 102)
ILLUSTRATIVE CASE
A 37-year-old male presented with multiple injuries following a significant crush injury and was initially treated with a bridging external fixator and VAC to an open right pronation external rotation type ankle fracture. Following medical stabilization, definitive fixation of both ankle fractures was achieved with a combination of plates and screws together with four TightRopes, two for each diastasis. After 9 months, a sinus to the lateral wound of the left ankle developed, which was discharging serous fluid. Radiological lucency was observed around the TightRopes (Figure 1). The two devices were removed and their tracks debrided. The curettage showed no growth on culture but histological evidence of a foreign-body osteolysis reaction secondary to polyethylene wear debris. No antibiotics were used, and there remained no clinical evidence of infection at the final followup 3 months later.

Radiological lucency surrounding TightRope implants. Polyethelene debris and osteolysis surrounding the TightRopes identified on histology.
DISCUSSION
As with any new surgical device and procedure, there was a learning curve for TightRope insertion. During 3 years of using this device in our unit, we have observed three notable complications and pitfalls of using the TightRope: osteomyelitis surrounding the TightRope, rediastasis resulting from a failure of the implant insertion technique, and FiberWire polyethylene wear-related painful aseptic osteolysis. On the basis of our experience of these 102 cases, we suggest a modification of the surgical technique for TightRope insertion as outlined below and in Table 2.
Learning Points from TightRope-Related Complications and Proposed Changes to the Manufacturer's Suggested Operative Technique
The sharp, inflexible, FiberWire knot (No.5, three half-hitches) protrudes deep to the lateral wound and can result in a stitch abscess and osteomyelitis (three out of 102 cases) (Table 1 and Figure 2). None of the patients with wound problems or osteomyelitis in this case series had had open fractures or external fixators applied. There have been three other published cases of infection related to TightRopes requiring removal of the device. 1,4,9 As described in the Arthrex TM TightRope® Surgeon's Guide, the FiberWire is best cut 1 cm beyond the knot. We concur with a recent report suggesting the importance of burying the sharp end of the suture adjacent to the fibula to prevent skin irritation. 6
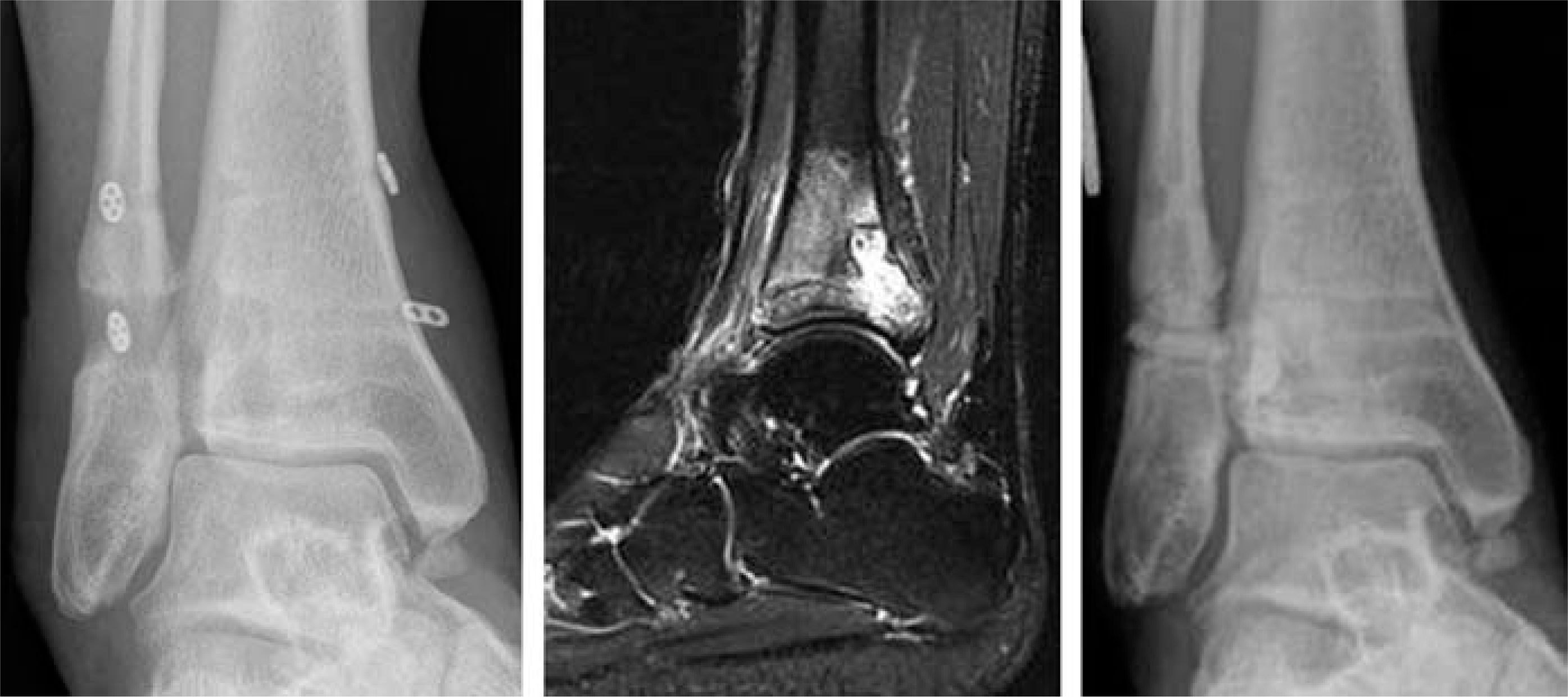
Radiographic and magnetic resonance imaging evidence of osteomyelitis surrounding TightRopes. Managed by track debridement and PALACOS cement insertion.
Device malpositioning and migration can both lead to rediastasis. The Arthrex TM TightRope® Surgeon's Guide suggests that insertion of a TightRope be performed without a medial incision. However, the risk of soft tissue interposition between the medial endobutton and the medial tibial cortex (Figure 3) and subsequent soft tissue necrosis leading to loosening of the TightRope construct leads us to recommend a small medial incision to ensure accurate positioning of the endobutton directly onto the tibial cortex (Figure 4). We also advise to always insert the TightRope through a fibular plate, because the lateral endobutton can pull through the thin lateral fibula cortex during insertion or subsequently (Figure 5). If a fibular plate is not required to stabilize the fracture configuration, it is advisable to use a small plate to act as a washer for the lateral TightRope button (Figure 4).

Potential for rediastasis caused by soft tissue interposition between the medial TightRope endobutton and the tibia or medial TightRope endobutton malposition.

Fibula plate to anchor the lateral button. Medial wound to ensure tibial contact without soft tissue interposition for the medial endobutton.

Potential for rediastasis caused by fibula button pull-through during insertion or fibula button intraosseous migration.
Previous studies have raised concerns regarding endobut-tons pulling through the cortex. 1,5 There have been reports from cadaver studies of significant rediastasis with the use of TightRopes when compared to 4.5-mm screws spanning four cortices. 5 However, there are no reports suggesting that the TightRope device can overtighten the syndesmosis and, therefore in our view, the above techniques should be used to reduce the chances of construct loosening. Recent evidence suggests that for supination–external rotation injuries, there is little difference in functional outcomes between stabilizing or leaving a radiologically detectable diastasis. 10 When used for Weber B/supination–external rotation type injuries, the TightRope may not have the same mechanical demands placed on it compared to when it is used for a Weber C/pronation external rotation type of injury, and it may therefore be less likely to mechanically fail.
To our knowledge, this is the first article to report histological evidence of polyethylene wear debris (polyethylene birefringent inorganic material) in excised connective tissue from around a TightRope device. The principal advantage of using this device is to allow continued movement at the distal tibiofibular joint, both in the anteroposterior and the proximal-distal planes. Widening of the tibial tunnels around the implants occurred in our cases and has been noted previously, 4 and we question if it is evidence of an osteolytic reaction to polyethylene wear debris. This may become painful, necessitating TightRope removal, as described in the report, and perhaps previously in two reports of foreign-body type reactions to the TightRopes requiring implant removal. 4,13 We offer these observations and recommendations in an attempt to improve the clinical effectiveness and safety of a useful new tool in the management of syndesmotic injuries.