
Abstract
Level of Evidence: V, Expert Opinion
INTRODUCTION
Arthroscopic subtalar arthrodesis has been reported as an alternative to traditional open methods for intractable hindfoot disorders, such as subtalar arthritis after fracture of the calcaneus or talus, primary arthritis, talocalcaneal coalition, or inflammatory arthritis, 1,2,5,6,9 because of its advantages, including minimal invasion to the soft tissue around the hindfoot and preserving the blood supply to the talus. Although the lateral approach using anterolateral and posterolateral portals in the supine or lateral decubitus position was initially introduced for arthroscopic subtalar arthrodesis, 4,8 recent reports have described the use of posteromedial and posterolateral portals with patients in the prone position, permitting surgeons to access the posterior subtalar joint easily, as compared with the lateral approach. 1,9 Additional techniques, such as the use of a third, accessory portal 2,5,9 or bone substitute for grafting, 1,5 have been reported to result in successful fusion without nonunion. To minimize the risk of nonunion, bone grafting into the void is recommended after sufficient debridement. 1,5 Subtalar arthrodesis with large amounts of cancellous bone graft without internal fixation has also been reported. 7 Although it is easy to perform bone grafting with an open method, grafting through small portals is troublesome because of the size of pieces of cancellous bone may make another incision for grafting, in addition to the arthroscopic portal, necessary. To achieve the implantation of autologous bone via arthroscopic portals, we use a tube harvester, which is a tool commonly used in mosaicplasty for harvesting osteochondral plugs, for harvesting rigid cancellousautograft. In this report, we describe a minimally invasive surgical technique for arthroscopic subtalar arthrodesis via a posterior approach using two portals accompanied by grafting of autologous cancellous bone from the iliac crest.
TECHNIQUE
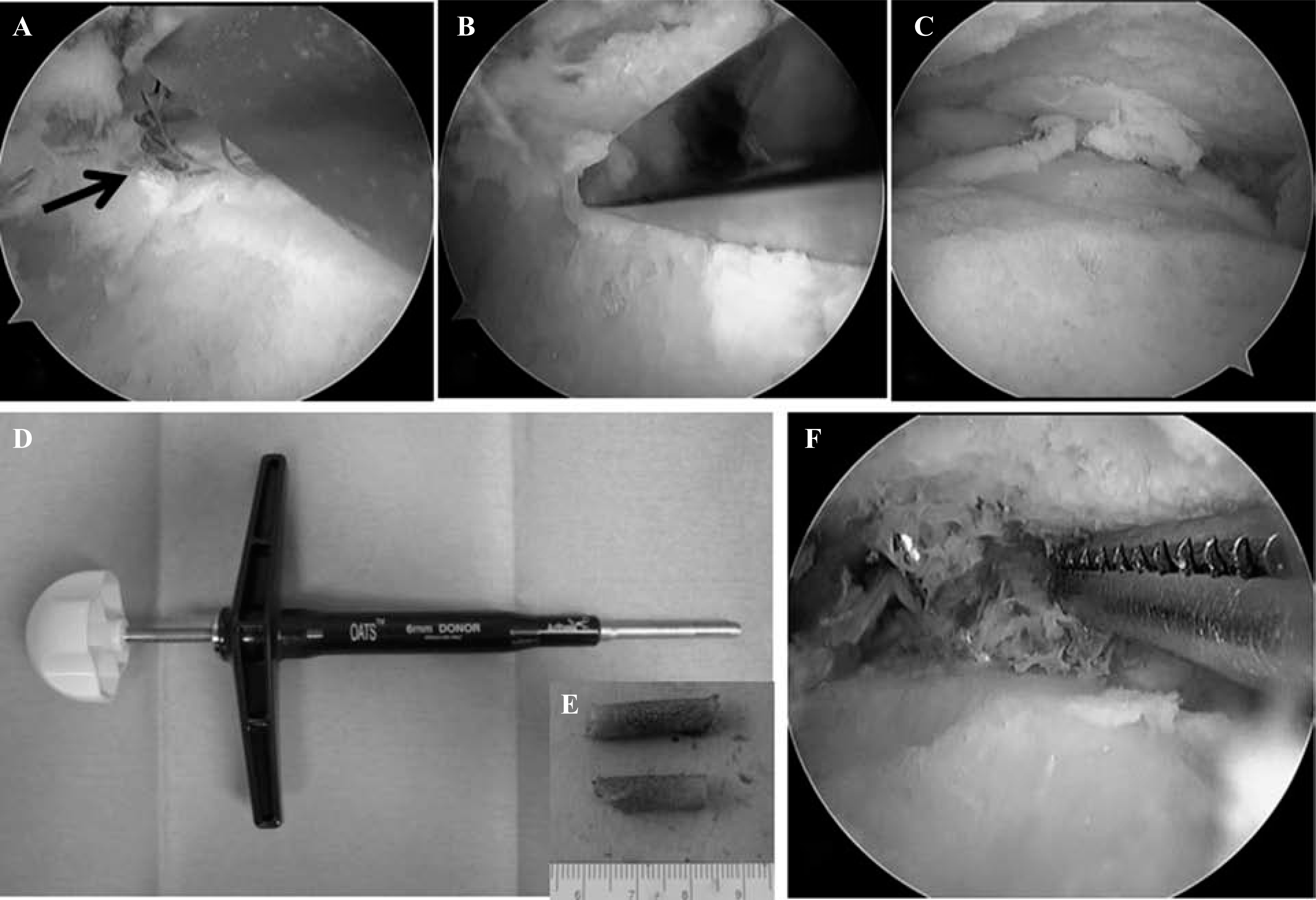
Patients with severe arthritis with malalignment are excluded. The operation is performed with the patient under general anesthesia and in a prone position with a thigh tourniquet. The arthroscopic procedure is started via posterolateral and posteromedial portals adjacent to the Achilles tendon at the level of the lateral malleolus. First, the shaver is inserted through the posteromedial portal, and the soft tissue is removed until the flexor hallucislongus (FHL) tendon is identified by arthroscopic visualization. If tenosynovitis is present around the FHL tendon, release of the flexor retinaculum and synovectomyis performed. After identification of the FHL tendon, the soft tissue overlying the posterior facet of the subtalarjoint is removed from the lateral field of the FHL tendon. Next, the articular cartilage of the posterior facet of the subtalarjoint is removed using a small chisel and a shaver until subchondral bone is exposed (Figure 1, A–C). After curettage of the anterior region of the posterior facet is confirmed arthroscopically, temporary fixation is performed using guide wires with the hindfoot in neutral position.
(
Cancellous autograft bone is harvested from the ipsilateral posterior iliac crest by inserting a single-use tube harvester [6-mm diameter; osteoarticular transfer system (OATS), (Arthrex, Naples, FL; Figure 1D] between the bilateral cortical bones. Two or three rigid cancellous bone plugs can be harvested through an approximately 1.5-cm skin incision by changing the insertional direction of the harvester; harvested cancellous bone plugs are cut by a blade into small bone columns so that autologous bone grafting is more easily performed via the arthroscopic portals (Figure 1, E and F). Under arthroscopic visualization, autologous bone is grafted into the void after curettage of the posterior facet of the subtalar joint, and two or three headless cannulated screws (Acutrak Plus, Acumed, Hillsboro, OR) are inserted from the plantar aspect of the heel into the talus through the posterior facet of the subtalar joint. Using fluoroscopy, we verify that the hindfoot position is adequate. After surgery, active range-of-motion exercise of the ankle joint is allowed the next day. Partial weightbearing is allowed 6 weeks after surgery, and full weightbearing is permitted after a bridging callus is confirmed between the posterior facets.
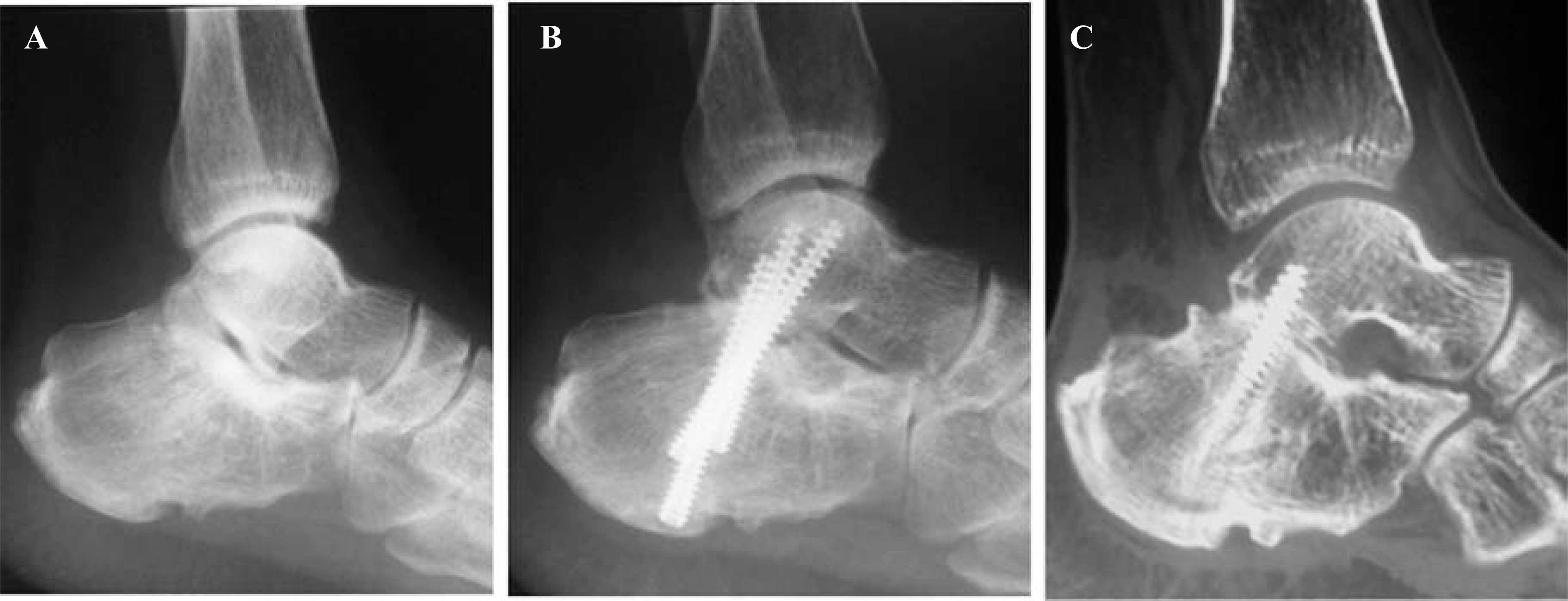
Eight patients with an average age of 51.5 (range, 40 to 59) years underwent our procedure for posttraumatic subtalar arthritis with followup exceeding 24 months (average, 26.6 months; range, 20 to 36 months). The average preoperative American Orthopaedic Foot and Ankle Society (AOFAS) scale score improved by 32 to 75 points at the final follow-up. In all of the patients, complete fusion was achieved by 8 weeks after the surgery (Figure 2). No complications such as infection, wound breakdown, or nerve injury were observed.
(
DISCUSSION
To the best of our knowledge, this is the first article reporting the implantation of autologous bone for subtalar fusion via arthroscopic portals. In 2000, van Dijk introduced an endoscopic posterior approach with the patient in the prone position to allow access to the posterior ankle compartment, subtalar joint, and extra-articular structures, 10 and, recently, this approach has been applied to arthroscopic subtalar arthrodesis. 1,2,5,6,9 This approach appears suitable for arthroscopic arthrodesis because only the posterior facet, which is the main articular surface of the subtalar joint, is the target for fusion in arthroscopic arthrodesis. Furthermore, the use of a third portal as an accessory portal that allows joint distraction by insertion of a large, blunt trocar and the placement of bone graft or a synthetic substitute has been reported. 2,5,9
For both open and arthroscopic procedures, a major complication of subtalar arthrodesis is nonunion. In 184 feet that underwent open subtalar arthrodesis, Easley et al. 3 reported a nonunion rate of 16%, which was higher than that previously reported, and 42% of their patients had avascular subchondral bone measuring more than 2 mm at the subtalar joint. Furthermore, because all patients with nonunions in their study had this condition, avascular bone was considered a risk factor for nonunion. Therefore, the importance of aggressive debridement of subchondral bone when performing subtalar arthrodesis is essential. However, such debridement produces a void between the joint surfaces after debridement that should be filled by bone graft. Although autografting, which is inexpensive and for which tissues can be harvested quickly and easily, remains the standard treatment, grafting through a small arthroscopic portal may be troublesome compared with grafting in traditional open procedures, because harvested autologous cancellous bone has to be prepared such that it can pass thorough small arthroscopic portals.
The tube harvester is a tool for harvesting plugs in osteochondral plug transplantation. For this surgical procedure, the use of this tool facilitated obtaining an implant the appropriate size and shape of autologous cancellous iliac crest bone that could be passed through small arthroscopic portals into the subtalar joint. Cancellous bone plugs harvested from the iliac crest by means of a tube harvester were converted into several small bone columns by cutting the harvested plugs with a blade at even, regular intervals, which could then be easily inserted into the void through an arthroscopic portal. In our experience, two cancellous bone plugs with a diameter of 6 mm and a height of 15 mm are sufficient for bone grafting in subtalar arthrodesis, and consolidation was achieved within 8 weeks after surgery with this procedure in all patients in our series.
Arthroscopic procedures have been shown to have lower nonunion rates than open procedures for subtalar arthrodesis. 1–3,5,6,9 To minimize the surgical invasion and reduce the risk of complications for subtalar arthrodesis, we propose an arthroscopic posterior approach to implant osseous autografts into the joint space.