
Abstract

Keywords
INTRODUCTION
An isolated gastrocnemius contracture (IGC) is often encountered in patients with foot and ankle pathology. DiGiovanni and colleagues reported the presence of an IGC in 65% to 88% of nonneuropathic patients with midfoot or forefoot symptoms, compared with 25% of asymptomatic controls. 10 More recently, Patel and DiGiovanni found that 57% of patients who presented to an outpatient orthopaedic clinic with plantar fasciitis had an IGC. 27 Before these studies, there were limited reports on the association between IGC and foot pathology in the adult population. 11,13,25 Furthermore, no distinction was made between contractures of the gastrocnemius or the entire gastrocsoleus complex. Thus, if operative intervention was indicated, the contracture was treated with an open or percutaneous Achilles lengthening.
In contrast, a gastrocnemius recession has been performed for many years for contractures associated with pediatric neuromuscular disorders. 32,37,38 Over the past decade, as the link between decreased ankle dorsiflexion and clinical pathologies continues to emerge, there has been an increase in use of this procedure in the adult population. This increase has included both its use as an isolated procedure 4,12,14,19,20,24,28 or as an adjunct to other adult foot and ankle procedures. 7,32,33,39 This topical review defines a gastrocnemius contracture, outlines its impact on foot and ankle pathology, and reviews the potential role of an isolated gastrocnemius recession as treatment for select disorders.
BACKGROUND
The triceps surae is a combination of the two strong plantarflexors of the ankle: the gastrocnemius and the soleus muscles. The gastrocnemius originates on the posterior femoral condyles, while the soleus originates on the posterior aspect of the tibia, fibula, and interosseous membrane. Both muscles insert into the calcaneal tuberosity via the Achilles tendon and can contribute to an equinus contracture. An equinus contracture is a limitation in ankle dorsiflexion not caused by intrinsic bony ankle pathology. It may be secondary to a global contracture of the gastrocnemius–soleus complex or isolated to the gastrocnemius muscle alone. 3 When the equinus contracture involves the entire gastrocnemius–soleus complex, it can be termed an Achilles contracture. This term is not entirely appropriate because the Achilles tendon accounts for only 3% to 5% of the elastic stretch of the triceps surae. 10 When the contracture involves only the gastrocnemius, it should be termed an isolated gastrocnemius contracture.
Whereas the soleus only crosses the ankle and subtalar joints, the gastrocnemius also crosses the knee joint. As such, the excursion of the gastrocnemius and soleus muscles can be differentiated on physical exam with the Silfverskiold test. When performing this test, the examiner passively dorsiflexes the ankle with the patient's knee extended and the subtalar joint held in a neutral postion. 35 The patient's knee is then flexed while the examiner continues to dorsiflex the ankle. An improvement in dorsiflexion with the knee flexed is considered a positive test and indicative of an IGC. 27 The most commonly used criterion to indicate an isolated gastrocnemius contracture is less than 10° of dorsiflexion with the knee extended, which improves past neutral with knee flexion. 9,10,27 The Silfverskiold test has been shown to have a sensitivity of 89% and a specificity of 90% when compared with goniometric evaluation. 27
It is imperative that the hindfoot remain neutralized during the Silfverskiold test. If the hindfoot is in valgus, the transverse tarsal joints unlock and dorsiflexion occurs through the hindfoot and midfoot, rather than the ankle joint. It is also emphasized that this is a passive test designed to test the resting tone of the gastrocnemius as occurs during the stance phase of gait. If active dorsiflexion occurs during the test, the resting tone of the gastrocnemius is relaxed and further dorsiflexion can be obtained.
Ankle equinus contractures have been shown to contribute to foot and ankle pathology. Gait analysis data suggest that 10° to 18° of ankle dorsiflexion is necessary for normal gait. 40 If a patient cannot obtain this degree of dorsiflexion, increased strain may be placed on adjacent joints and soft tissues. 2 This may explain the increased rate of IGC that has been reported in patients presenting with foot and ankle pathology. 10,27
NONOPERATIVE TREATMENT
Calf muscle stretching is frequently recommended for patients with ankle equinus contractures. It is unclear, however, if such stretching is actually effective in increasing ankle dorsiflexion. In their systematic review of five trials assessing static calf muscle stretches, Radford et al. found that ankle dorsiflexion increased by 2° if stretched less than 15 minutes and 3° if stretched for 15 to 30 minutes three to seven times per week for 3 to 6 weeks. 30 Grady and Saxena also reported limited change in muscle flexibility after a 26-week home stretching protocol. 15 In contrast, Johnson et al. reported a 12° increase in passive ankle dorsiflexion following a 6-week stretching program in older women. 18 Using a technique called proprioceptive neuromuscular facilitation stretching, Mahieu et al. were able to demonstrate a mean increase in ankle dorsiflexion of 6° after 6 weeks of stretching. 23
Despite the controversy regarding the degree to which stretching increases range of motion, calf muscle stretching exercises have been used to successfully improve symptoms in patients with plantar fasciitis (especially when combined with plantar fascia specific stretching exercises) and Achilles tendinosis (when combined with eccentric muscle contraction). 5,8
OPERATIVE TREATMENT
The gastrocnemius recession was originally developed to address calf spasticity while maintaining the strength of the ankle plantarflexors. 37 It was also developed to avoid the potential complications associated with Achilles lengthening, namely wound healing problems, overlengthening, Achilles tendinosis, rupture, weakness, and prolonged recovery. 1,6
The first gastrocnemius recession procedure was reported by Vulpius and Stoffel in 1924. 3 Since then, a variety of gastrocnemius recession procedures have been described. The indication for a gastrocnemius recession in the early literature was an equinus contracture in the neurologically impaired child. 37 Over the past decade, gastrocnemius recessions have been used more frequently in the adult population, both as an adjuvant and an isolated procedure for the treatment of pain associated with foot and ankle pathology in the setting of an isolated gastrocnemius contracture. In the majority of cases, patients were previously unresponsive to traditional nonoperative therapies attempting to stretch or lengthen the gastrocnemius–soleus complex.
A number of procedures exist for lengthening the gastrocnemius–soleus complex and gastrocnemius muscle in isolation. All procedures fundamentally attempt to increase ankle dorsiflexion. Only a few of these procedures are commonly performed. They are primarily defined by their anatomic location (Figure 1).
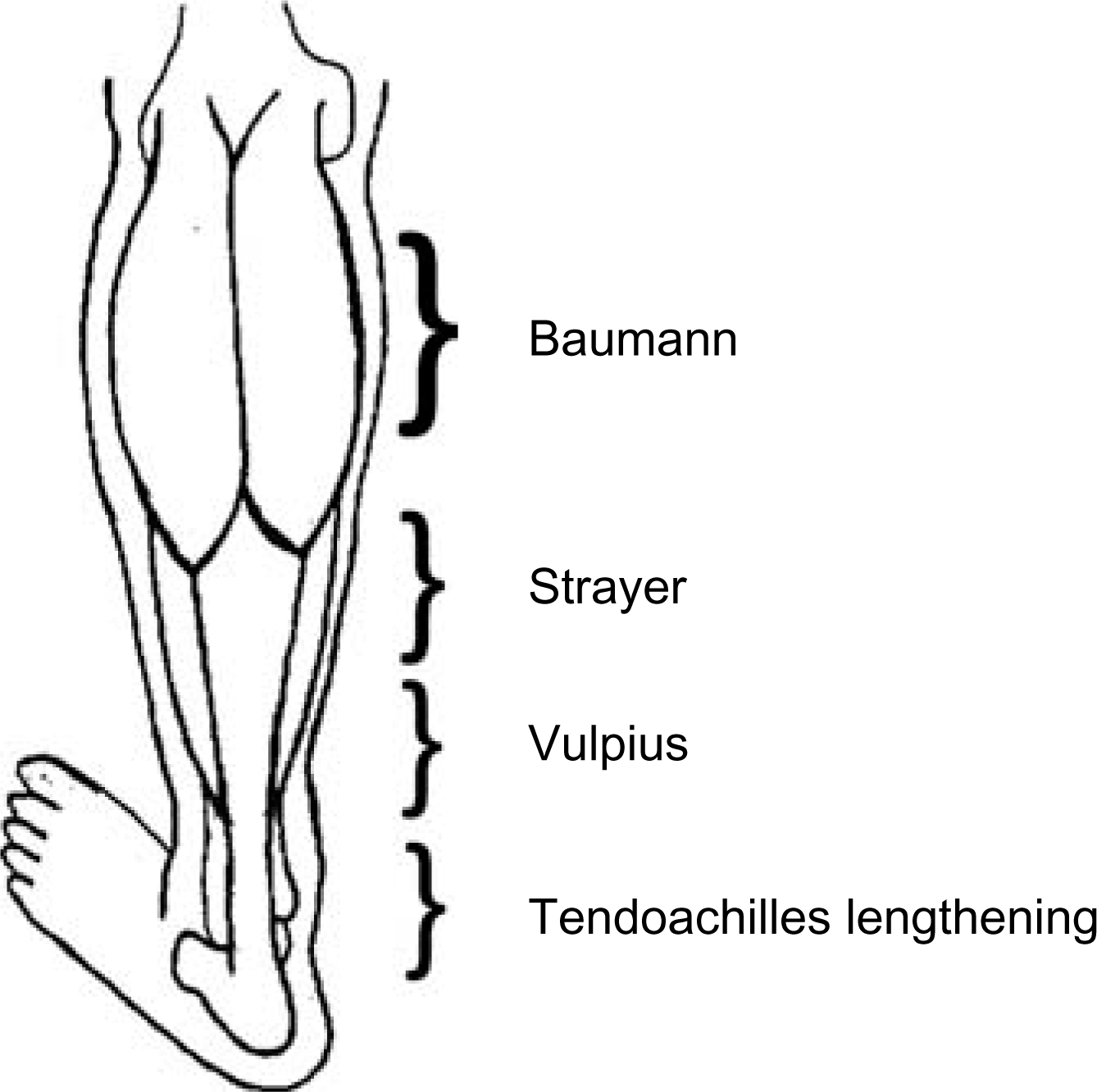
Anatomic location of gastrocnemius recession procedures.
Vulpius procedure
Vulpius and Stoffel described the original gastrocnemius–soleus recession in 1924. 3 The incision is made at the level of the distal one-third of the soleus muscle belly. At this level the gastrocnemius is a tendinous structure. With the Vulpius technique, a transverse cut is made through the superficial side of the gastrocnemius tendon as well as an incision through the deep fascia and median raphe of the soleus muscle. 17 The Vulpius procedure incises both the gastrocnemius fascia and the soleus fascia. It is therefore useful in patients with plantarflexion contractures in which both the gastrocnemius and soleus muscles are restricted and who have a negative Silfverskiold test on physical examination.
Strayer procedure
In 1950, Strayer reported a variation of the Vulpius technique that reduced the amount of disruption to the soleus muscle. 37 The skin incision for the Strayer procedure is made on the posterior calf just proximal to the gastrocnemius–soleus aponeurosis. The level of the incision has been described as 2 cm distal to the gastrocnemius indentation. 29 The gastrocnemius and soleus fascial layers are bluntly separated and, once isolated, the gastrocnemius fascia is sectioned one to two fingerbreadths distal to the musculotendinous junction, without disruption of the soleus. This allows the gastrocnemius tendon and muscle to retract proximally. In the original description, the gastrocnemius fascia was then sutured to the soleus fascia in a more proximal location. 37 Recent modifications do not include suturing of the fascia. Using this technique, the IGC is corrected and the pull of the gastrocnemius is diminished without interfering with the soleus muscle or distal Achilles tendon. 29
Baumann procedure
Another procedure used to lengthen the gastrocnemius muscle is the Baumann procedure. Baumann and Koch described this technique in 1989 for the treatment of patients with cerebral palsy. 17 In this technique, an incision is made along the proximal medial calf, and the plane between the gastrocnemius and soleus is developed. The recession is then performed on the deep undersurface of the gastrocnemius muscle. The tendon of the plantaris muscle is cut and a transverse incision is made across the gastrocnemius muscle fascia and the intramuscular septum between the medial and lateral gastrocnemius heads. Dorsiflexion is then tested and, if lacking, another recession of the gastrocnemius fascia is made 1 to 2 cm away from and parallel to the original. The advantages of both this procedure and the Strayer, as compared with the Vulpius, are that they isolate the gastrocnemius muscle, leave the soleus intact, and potentially preserve the muscle strength of the plantarflexors. 17
Endoscopic gastrocnemius recession procedure
An endoscopic modification has been described for the gastrocnemius recession. The endoscopic technique is reported to improve isolation of the gastrocnemius fascia and thereby reduce injury to the soleus muscle fibers. 34,38 Tashjian et al. first described the technique in cadaveric limbs. 38 In 2004, Saxena and Widtfeldt reported a series of 18 patients 34 and, in 2005, Trevino et al. reported a series of 28 patients 39 treated with the endoscopic technique. Two 1- to 2-cm incisions are made on the medial and lateral aspects of the gastrocnemius aponeurosis, at the same level described by Strayer. After blunt dissection to the fascia, the fascia is elevated and a cannula is introduced through the medial incision. A 4-mm endoscope is then inserted to visualize the gastrocnemius aponeurosis and sural nerve. The endoscope is removed and a cannulated camera-mounted knife is then used to incise the gastrocnemius fascia.48 Although this technique is reported to limit operative time and improve cosmesis by using smaller skin incisions, increased rates of sural nerve complications have been reported. 34,39
OUTCOMES OF GASTROCNEMIUS RECESSION
The gastrocnemius recession may be used in isolation or as an adjunct to other foot and ankle procedures. The associated pathologies for which the gastrocnemius recession procedure has been used include plantar fasciitis, 4,24 metatarsalgia, 24,28 Achilles tendinopathy, 12,14,19 posterior tibialis tendon dysfunction, 7,28,32–34,39 arthritis, 32–24,39 neuromuscular conditions, 16,34,36,37,39 forefoot ulcers, 16,21,39 and hallux valgus. 28,39 Despite the wide array of indications and reports, there are limited outcome studies of gastrocnemius recession procedures (Table 1). This review focuses on those disorders for which a gastrocnemius recession is used in isolation, namely plantar fasciitis, Achilles tendinopathy, metatarsalgia, and forefoot ulceration.
Summary of Studies Using Gastrocnemius/Gastrocsoleus Recession Procedures in Isolation to Treat Various Foot Pathologies
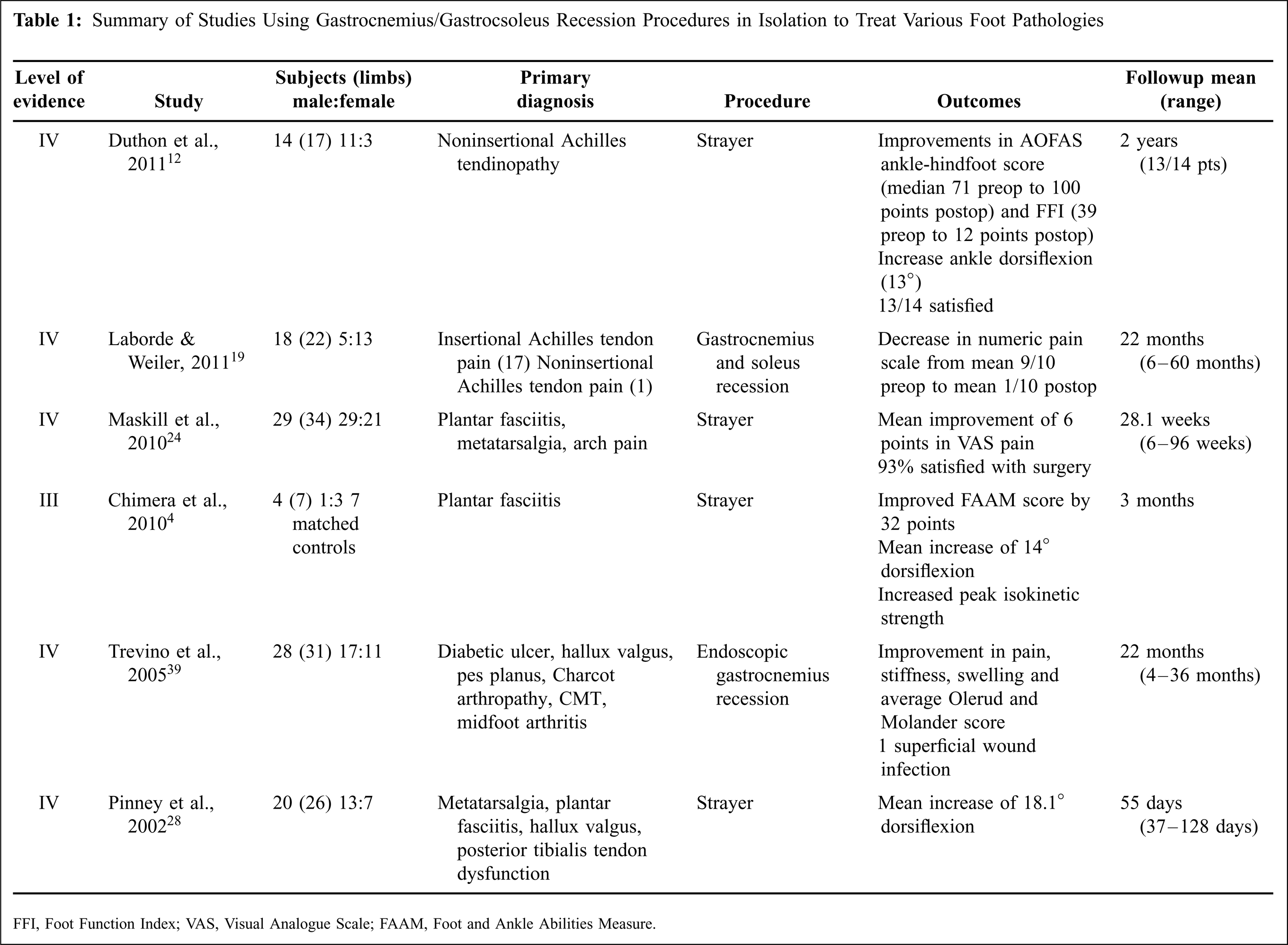
FFI, Foot Function Index; VAS, Visual Analogue Scale; FAAM, Foot and Ankle Abilities Measure.
Effect on ankle motion
Following a gastrocnemius recession, studies consistently demonstrate resolution of the gastrocnemius equinus contracture, with reported increases in ankle dorsiflexion ranging from 12° to 18°. 17,24,28,32 Pinney et al. reported on the gastrocnemius recession's ability to improve ankle dorsiflexion. 28 In 20 patients with an IGC, these authors demonstrated that an isolated Strayer procedure improved ankle dorsiflexion by 18°. They also found that patients' postoperative ankle dorsiflexion with the knee extended was equal to preoperative motion with the knee flexed. This correction was maintained at short-term follow-up (37 to 128 days). Herzenberg et al. confirmed the improvement in ankle dorsiflexion associated with a gastrocnemius recession in a cadaveric study using the Baumann procedure. 17 In addition, Maskill et al. have reported increases in ankle dorsiflexion after gastrocnemius recession in patients with plantar fasciitis. 24
Plantar fasciitis
The traditional surgical treatment for recalcitrant plantar fasciitis is a partial plantar fascia release. Plantar fascia release combined with nerve decompression has also been recommended. 22 Patients who undergo this type of surgery occasionally have persistent pain, functional limitations, and prolonged recovery times. 22 This has led surgeons to explore other methods of operative intervention. Biomechanically, contracture of the Achilles tendon or the superficial posterior musculature has been linked to increased tensile loading of the plantar aponeurosis. 3,8 An equinus contracture has been reported in 83% of patients presenting with plantar fasciitis. 27 Fifty-seven percent of these patients had an equinus contracture that was isolated to the gastrocnemius muscle. It has therefore been theorized that treating the equinus contracture may reduce plantar fascia pain.
The largest series of patients with plantar fasciitis treated with gastrocnemius recession was reported by Maskill et al. 24 They assessed pain relief in 29 patients who underwent a Strayer procedure for an isolated gastrocnemius contracture associated with recalcitrant plantar fasciitis, metatarsalgia, or arch pain. Twenty-five of the 29 patients had a primary diagnosis of plantar fasciitis. The average 10-point visual analog scores improved from 8 to 2. The greatest improvements in pain scores were found in patients with plantar fasciitis. These patients also reported a high (93%) satisfaction rate with the surgery. In addition to pain relief, the authors confirmed increases in ankle dorsiflexion on physical examination.
Studies examining functional outcome scores following gastrocnemius recession for plantar fasciitis are limited. Using the validated Foot and Ankle Ability Measure outcome instrument, Chimera et al. 4 reported on four patients with plantar fasciitis who underwent an isolated Strayer procedure. Three months postoperatively, the patients reported 35% to 45% improvement in function and global rating scales, as well as improved strength. However, these scores remained lower than healthy control subjects.
Achilles tendinopathy
Tightness of the gastrocnemius–soleus complex will increase tension in the Achilles and may manifest as pathologic degeneration at the insertion or above. 3 This may account for the beneficial effect of stretching protocols in symptomatic treatment of Achilles tendon disorders. 5 The traditional operative treatment of refractory Achilles tendinopathy has in some series been associated with high complication rates, inadequate relief of symptoms, and long recovery periods. 5 Recently, the gastrocnemius recession has been reported as an isolated procedure for treatment of Achilles tendinopathy, both insertional and noninsertional. Gentchos et al. published a case report on a gastrocnemius recession used to treat a patient with refractory Achilles tendinopathy in 2008. 14 After 6 months of failed nonoperative treatment for insertional Achilles tendinopathy, the patient underwent an isolated gastrocnemius recession (modified Vulpius). At 6 weeks postoperatively, the patient had complete resolution of pain (0/10 on the visual analog scale, VAS) and at 24 months remained asymptomatic. Follow-up magnetic resonance imaging at 2 years showed normalization of signal and thickness of her distal Achilles tendon.
In 2011, Duthon et al. reported a prospective case series of 14 patients (17 tendons) with noninsertional Achilles tendinopathy who had failed 1 year of nonoperative management. 12 These patients underwent an isolated Strayer gastrocnemius recession. They were evaluated preoperatively and at 1 and 2 years postoperatively using the Foot Function Index (FFI), the American Orthopaedic Foot and Ankle Society score (AOFAS), and VAS. At both 1- and 2-year follow-up, patients showed significant improvement in their FFI (from 39 points preoperatively to 12 points postoperatively) and AOFAS scores (71 preoperatively to 100 points postoperatively). The SF-12 scores also showed significant improvement from an average of 36 points before surgery to 51 points at 1 and 2 years after surgery. The authors did not report any postoperative complications and all patients returned to their regular occupations.
Recently, Laborde and Weiler reported improved pain scores in 24 patients treated with gastrocnemius–soleus recession for insertional and noninsertional Achilles tendon pain. 19 Seventy-five percent of patients (18/24) had greater than 6 months follow-up. Average reported pain at follow-up was 1/10 compared with 9/10 preoperatively. No patient required further surgery or treatment. Eleven of the patients had diabetes and no wound complications occurred.
Metarsalgia and plantar ulceration
Limited dorsiflexion of the ankle has been shown to increase forefoot loading during gait, creating higher-pressure areas. 1 These high-pressure areas may result in pain, deformity, and ulceration in some patient populations. 1,10 The literature for the use of a gastrocnemius recession for metatarsalgia, hallux valgus, and forefoot ulceration is limited. Included in the previously mentioned studies by Maskill et al. and Pinney et al. were a small number of patients with metatarsalgia. 24,28 Pinney et al. reported improved dorsiflexion after gastrocnemius recession in patients with metatarsalgia, plantar fasciitis, hallux valgus, and flatfoot but did not stratify results by diagnosis. 28 No functional or satisfaction outcomes were reported. Maskill's series of 29 patients included six with metatarsalgia. However, results were not stratified by diagnosis either. 24 This study did report good pain relief and satisfaction from a gastrocnemius recession.
Forefoot ulceration is a difficult problem to treat and can ultimately lead to amputation. Current treatments include total contact casting, exostectomy, and tendo-Achilles lengthening (TAL). TAL has been shown to relieve forefoot pressure and assist in ulcer healing. 1,26 Percutaneous TAL resulted in a 27% decrease in peak plantar pressure measurements in the forefoot in patients with equinus contractures and previous forefoot ulceration. 1 In an randomized control trial, Mueller et al. demonstrated a 75% decrease in recurrence of forefoot ulceration when total contact casting (TTC) was combined with TAL as compared with TTC alone. 26 A potential complication of TAL is overlengthening of the gastrocnemius–soleus complex, causing a calcaneus gait. 3,6 This has not been reported with gastrocnemius recession.
The literature supporting the use of gastrocnemius recession for foot ulceration is not as robust as the literature for use of TAL. A case report describing the gastrocnemius recession to improve healing in a forefoot ulcer reported healing by 6 weeks with no recurrence by 20 months. 16 Laborde reported on 17 patients with 20 forefoot ulcers secondary to neuropathy. 21 He performed an isolated gastrocnemius–soleus recession in 5/20 ulcers and combined a gastrocnemius–soleus recession with peroneus longus or tibialis posterior z-lengthening in 14/20. He reported healing of the ulcer in 95% (18/19) of cases and a low recurrence rate (3/19) in those patients available for follow-up.
COMPLICATIONS OF GASTROCNEMIUS RECESSION
Although a gastrocnemius recession may avoid many of the potential complications associated with tendo-Achilles lengthening, complication rates following gastrocnemius recession range from 0% to 20%. 3,12,19,20,24,31,32,34,39 The complications reported in the literature include poor cosmesis because of the location of the incision, sural nerve injury (open 2%, endoscopic 16%), and decreased circumference of the calf secondary to muscle atrophy. 3,31,32,39 Other reported complications include infection, wound dehiscence, and complex regional pain syndrome. 31 The incision is 3 to 8 cm long and the skin can tether to the underlying fascia, potentially leading to poor cosmesis. Because of its location almost directly posterior to the gastrocnemius insertion point on the Achilles tendon, the sural nerve can be injured by direct trauma or excessive stretch during the procedure. To minimize risk of injury, it is critical that the sural nerve be identified and protected before recession of the gastrocnemius fascia. 17,31
Despite the positive operative results noted above, one of the potential drawbacks of a gastrocnemius recession is that mechanical lengthening of the myotendinous unit may contribute to weakness and disability. 4,32 It is thought that controlled and selective lengthening of the gastrocnemius–soleus complex or gastrocnemius alone minimizes this weakness, but the literature is not conclusive. There has been limited and contradictory information regarding strength changes after isolated gastrocnemius contracture. In a prospective study that assessed seven limbs in four subjects with isolated gastrocnemius contracture, Chimera et al. 4 found significant isometric (p = 0.02) and isokinetic (p = 0.01) strength deficits compared with matched control subjects preoperatively. Three months following the gastrocnemius recession, isometric plantarflexion strength did not change; however, there was a significant increase in isokinetic strength at 60°/s. Although postoperative improvements were noted in the patient group, these values remained below the values of the control subjects, as noted by confidence intervals. Sammarco et al. also found that patients remained weaker than their contralateral limb, but that improvements in strength were seen over time. 32
SUMMARY
Recent literature has demonstrated an increased awareness of the role of an IGC in patients with foot and ankle symptoms and disorders. However, the contribution of an IGC to the pathology and natural history of these foot and ankle disorders is not known.
Initial investigations of gastrocnemius recession procedures for a variety of pathologies suggest improvements in dorsiflexion range of motion, pain, and patient satisfaction. Functional outcomes, however, are less clear. Whether prospective or retrospective in design, comparison of outcomes among current investigations is difficult because of the small subject numbers and limited use of validated functional outcomes. Although further investigations are necessary, early reports note encouraging results for pain relief and increased motion for the gastrocnemius procedure used in isolation for plantar fasciitis, Achilles tendinopathy, metatarsalgia, and forefoot ulcerations.