
Abstract
Background: Type II accessory naviculars are frequently associated with planovalgus deformity. Operative treatment for patients recalcitrant to nonoperative treatment involves resection, with or without takedown, and reattachment of the tibialis posterior tendon as described by Kidner. This does not address the planovalgus deformity. The authors hypothesized that adding a subtalar arthroereisis to the Kidner procedure would lead to improvement of pain and function and correction of the deformity. Methods: Institutional Review Board-approved, prospectively collected data were reviewed for 20 patients (23 feet), who underwent a combined modified Kidner and subtalar arthroereisis for painful type II accessory navicular with planovalgus deformity recalcitrant to nonoperative treatment. The average age at the time of surgery was 18 years. Patients were evaluated preoperatively and at final follow-up clinically, radiographically, and via the visual analog pain scale (VAPS), the American Orthopaedic Foot and Ankle Society (AOFAS) ankle hindfoot score, and a satisfaction rating. Mean follow-up was 53.9 months. Results: The mean AOFAS scores improved from 53 preoperatively to 95 at final follow-up and the mean VAPS score decreased from 7.4 preoperatively to 1.7 at final follow-up. Radiographically, the average Meary's angle improved from 18.5° apex plantar preoperatively to 3° apex plantar on weight-bearing lateral radiographs, and the average talar head uncoverage percentage on weight-bearing anteroposterior radiographs improved from 24% preoperatively to 3%. Nineteen of 20 patients reported good or excellent results. Three patients required implant removal because of pain; no recurrence of planovalgus deformity occurred after implant removal. No patients developed subtalar arthritis. Conclusion: The modified Kidner procedure combined with a subtalar arthroereisis resulted in significant pain and functional improvement. The deformity correction obtained at surgery was maintained even if the arthroereisis plug was removed. The extra-articular plug did not lead to subtalar arthritis.
Level of Evidence: IV, Case Series
INTRODUCTION
The accessory navicular is a supernumerary ossicle that occurs within the substance of the tibialis posterior tendon (PTT) at its navicular insertion. The incidence has been described as occurring in 10% to 14% of feet, and it is usually asymptomatic. 22 Symptoms develop when recurrent stress occurs at the synchondrosis between the accessory bone and the medial navicular tuberosity secondary to the pull of the tibialis posterior tendon or trauma. Geist described a chronic inflammatory state developing at this articulation creating a stress fracture-type pattern. 5
As with most orthopaedic conditions, the first line of treatment is nonoperative and includes temporary immobilization (cast or CAM boot), bracing, orthotic inserts and shoe modification, and nonsteroidal anti-inflammatory medication. Operative intervention is indicated for patients recalcitrant to nonoperative treatment with persistent pain and dysfunction. Current operative treatments include simple excision of the accessory bone from within the PTT, or excision with takedown and reattachment of the PTT (with or without advancement), the modified Kidner procedure.
In type II accessory navicular, the accessory bone is separated from the actual navicular by a synchondrosis, which is frequently associated with a flexible planovalgus deformity and loss of the medial arch. 5 Patients presenting with medial foot pain and prominence should be evaluated for an accessory navicular as the cause of their pain. Although there is debate of the relevance of a symptomatic accessory navicular in the development of the planovalgus deformity, it has been shown that treatment of the accessory navicular alone may not correct the flatfoot deformity. 11,13,17
Flexible planovalgus deformity has been successfully managed with various soft tissue and bony procedures. Subtalar arthroereisis is a simple procedure in which an implant is placed extra-articularly into the sinus tarsi to “jack up” and correct the flatfoot deformity, restoring the medial longitudinal arch. It has been used extensively in the pediatric population with favorable outcomes and has recently gained some support for its use in the adult-acquired flatfoot. 1%,2,15,16,21,24,26 The authors hypothesized that, in patients with a symptomatic type II accessory navicular and a flexible flatfoot deformity, a combination of a modified Kidner procedure with a subtalar arthroereisis would lead to improvement of pain, function, and correction of the planovalgus deformity.
MATERIALS AND METHODS
This study was approved by our Institutional Review Board. A retrospective review was undertaken of all patients who underwent a modified Kidner procedure between April 2003 and April 2010. Inclusion criteria required the presence of a type II accessory navicular 7 as confirmed on plain radiography, a positive magnetic resonance imaging (MRI) for a stress reaction at the synchondrosis indicating its involvement in the pathologic process, clinical and radiographic planovalgus deformity, and failure of appropriate nonoperative management for a minimum of 6 months. All patients underwent a combined subtalar arthroereisis and a modified Kidner procedure as described as follows.
During the study period, 66 patients (70 feet) were diagnosed with a symptomatic accessory navicular that was recalcitrant to nonoperative management and underwent operative correction. Of those, only 23 patients (27 feet) had concomitant planovalgus deformity of their hindfoot (34.8% of patients; 38.6% of feet). These 27 feet underwent a combined arthroereisis and modified Kidner procedure. Four patients had bilateral procedures, which were staged at different times and evaluated as separate procedures. Three patients were lost to follow-up, one of whom had undergone bilateral procedures. All three patients' families had left the state and could not be located. Twenty patients (23 feet) were available for follow-up and included in this study. There were 14 females (17 feet) and six males, with a mean age of 18 (range, 10 to 27) years, which is consistent with the reported female predominance of this condition. There were 12 left and 11 right feet. The mean follow-up was 53.9 (range, 24 to 92) months (Table 1). The three patients who were lost to follow-up were all more than 4 years out from their surgery and had never returned with any problems or complaints and, to our knowledge, had not undergone implant removal. These patients were not included in any of the statistical analyses.
All patients were assessed prospectively preoperatively and at final follow-up clinically, radiographically, and via a questionnaire containing a visual analog pain scale (VAPS), the American Orthopaedic Foot and Ankle Society (AOFAS) ankle hindfoot score, 10 and a satisfaction rating. Clinical weight-bearing evaluation was performed from behind to assess for hindfoot valgus, “too many toes” sign, and arch height. Single- and double-leg heel rise maneuvers were undertaken by the patient to assess correctability of the deformity and strength of the PTT. All patients fit within the clinical and radiographic criteria of stage IIA flatfoot. No attempt was made to differentiate between abduction versus flattening, because a combination was usually present.
Preoperative and final postoperative follow-up weight-bearing anteroposterior (AP) and lateral radiographs of the foot were available for all cases. These were evaluated by an independent observer not involved with the operative treatment and blinded to the clinical results. Lateral talar first metatarsal angle (Meary's angle), talus-first metatarsal angle on AP radiographs, and the degree of talar head uncoverage as a percentage of the entire talar head on the AP radiograph were measured as previously described. 25 Subtalar arthrosis was excluded by clinical assessment with painless and uninhibited subtalar range of motion comparable with the contralateral side and the absence of radiographic changes of arthritis on subsequent studies.
Statistical analysis consisted of analysis of variance (ANOVA) using a commercially available computer software, StatView (SAS Inc., Cary, NC). A p value less than .05 was considered significant.
Demographic Data
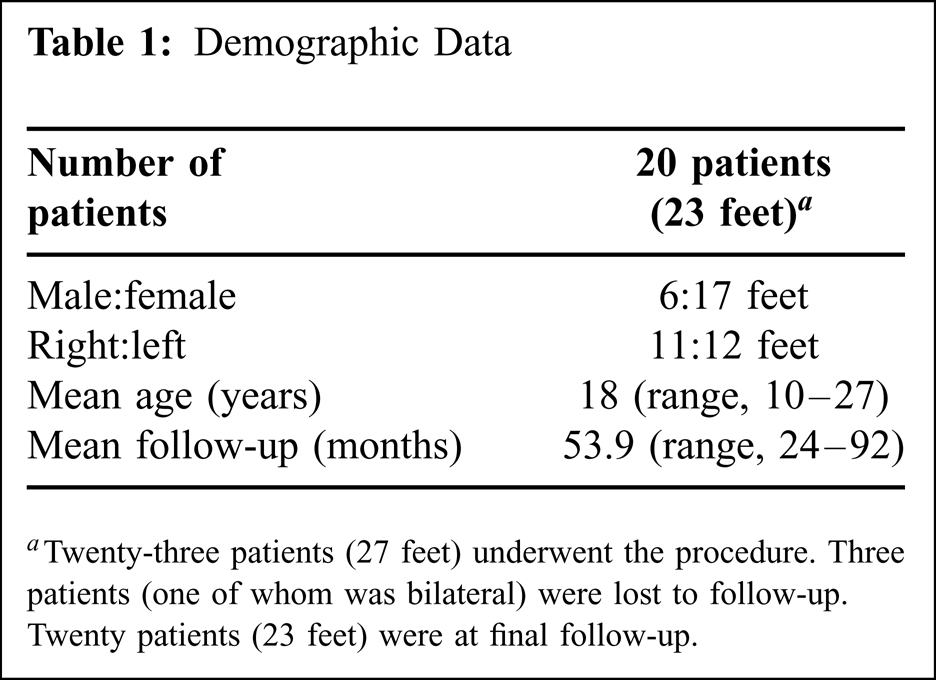
Twenty-three patients (27 feet) underwent the procedure. Three patients (one of whom was bilateral) were lost to follow-up. Twenty patients (23 feet) were at final follow-up.
OPERATIVE TECHNIQUE AND POSTOPERATIVE COURSE
All procedures were performed on an outpatient basis under general anesthesia, utilizing a calf tourniquet. The subtalar arthroereisis procedure was performed first to correct the planovalgus deformity before reattaching the PTT. A longitudinal 1-cm incision was made just dorsal to the peroneal tendons over the sinus tarsi. A blunt guide wire was inserted from anterolateral to posteromedial following the orientation of the sinus tarsi. Appropriate positioning was confirmed fluoroscopically.
Sequential smooth dilators were used to distract the sinus tarsi starting at a 6 mm and increasing by 2-mm increments. Simulated weight-bearing fluoroscopic evaluation was undertaken in both lateral and AP planes after inserting each dilator until the appropriate correction was obtained of the talus–first metatarsal axis and coverage of the talonavicular joint. The selected trial implant was then inserted over the wire and the foot position was again checked clinically and radiographically. The appropriate size implant limited subtalar eversion to 5° of valgus, without creating hindfoot varus. Radiographically the implant was positioned so that the lateral edge of the trial was flush with the lateral border of the talar neck, but the medial edge of the implant did not cross the midline of the talar neck. The final implant was then inserted over the wire to the appropriate position and correction was again radiographically and clinically verified. The guide wire was then removed medially to prevent potentially backing out of the implant. A titanium Maxwell-Brancheau arthroereisis (MBA) plug was used for all cases (Tornier, Warsaw, IN).
The modified Kidner procedure was next performed through a 5-cm medial incision made from 1 cm anterior to the tip of the medial malleolus to the medial cuneiform along the path of the PTT. The ossicle was identified and excised together with the entire synchondrosis and any residual navicular prominence until it was flush with the medial border of the talus. The tendon was completely detached from the PTT insertion site. The plantar medial tuberosity of the navicular (normal anatomic insertion point of the PTT) was decorticated. The modification of the Kidner procedure was performed utilizing a 5-mm suture anchor (Twinfix Ti, Smith & Nephew, Memphis, TN) inserted into the insertion point in the navicular. 4 Positioning of the anchor should be confirmed under fluoroscopy to ensure that the optimal reattachment point has been utilized and that the navicular–cuneiform joint has not been violated. With the hindfoot in a corrected anatomic position, the PTT was advanced and attached to the navicular at neutral resting tension, utilizing the two No. 2 braided nonabsorbable sutures attached to the anchor. With the deformity corrected, contracture of the gastrocsoleus Achilles mechanism was assessed using the Silfverskiold test, and a lengthening was performed if indicated (4 of 23 feet). The ankle was immobilized in a well-padded splint in slight inversion.
Sutures were removed after 10 to 14 days, and patients were placed in a neutral non-weight-bearing boot or cast for 4 additional weeks. At 6 weeks, patients were allowed to progress to protected weight bearing as tolerated, and physical therapy was initiated for PTT strengthening and gait training in a sneaker. At 12 weeks, patients were transitioned to a normal shoe and no further bracing or orthotic inserts were usually needed.
RESULTS
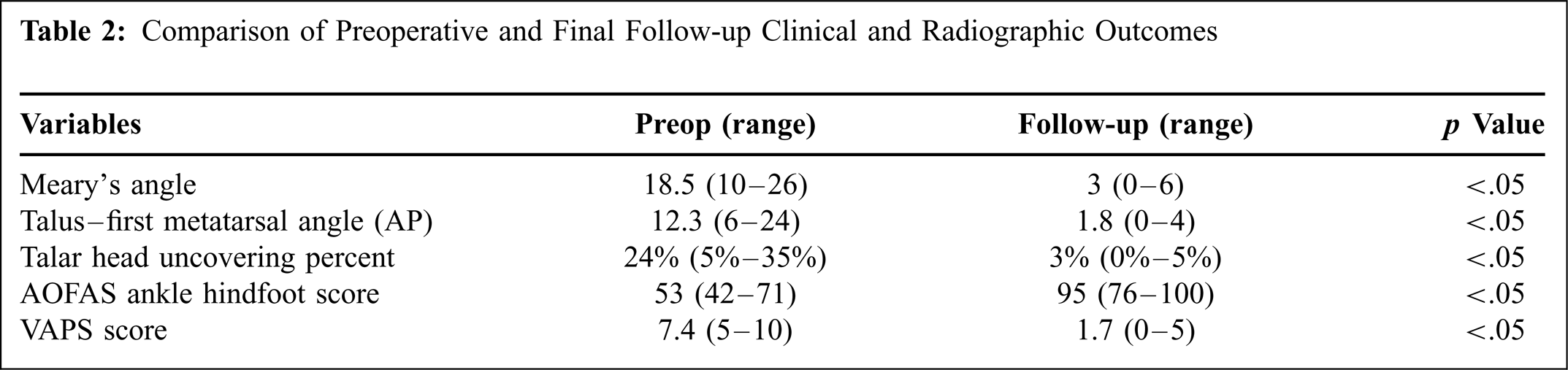
The mean AOFAS ankle hindfoot scores demonstrated significant improvement from a mean of 53 (range, 42 to 71) preoperatively to a mean of 95 (range, 76 to 100) at final follow-up (p < .05). The mean VAPS also improved significantly decreasing from 7.4 (range, 5 to 10) out of 10 preoperatively to 1.7 (range, 0 to 5) at final follow-up (p < .05) (Table 2).
Comparison of preoperative and final follow-up weight-bearing radiographs showed significant improvement in both Meary's angle and talar head coverage. 25 The average Meary's angle improved from 18.5° (range, 10° to 26°) apex plantar preoperatively to 3° (range, 0° to 6°) apex plantar at final follow-up (p < .05) (Figure 1). Talar-first metatarsal angle as measured on AP radiographs also significantly improved from an average of 12.3° (range, 6° to 24°) preoperatively to an average of 1.8° (range, 0° to 4°) at final follow-up (p < .05) (Figure 2). The average talar head uncoverage on AP radiographs improved from 24% (range, 5% to 35%) preoperatively to 3% (range, 0% to 5%) at final follow-up (p < .05) (Table 2).

Pre- and postoperative lateral radiographs demonstrating improvement in Meary's angle.

Pre- and postoperative AP radiographs demonstrating improvement in both the talar-first metatarsal angle and talar head coverage.
Nineteen of 20 patients (22 of 23 feet) rated their results as good or excellent and would undergo the procedure again. There were no wound complications or infections. Three patients required removal of the arthroereisis plug because of impingement pain laterally. These were performed 9, 17, and 23 months after implantation. All of these were larger implants (two size 10 mm and one size 12 mm). None of these patients developed any recurrence of their planovalgus deformity either clinically or radiographically at final follow-up (Figure 3). The patient undergoing implant removal at 9 months had continued lateral and medial pain despite maintenance of foot alignment radiographically with absence of subtalar arthrosis and a normal MRI study and was the only poor result in the study. The other two patients had complete resolution of their symptoms and rated their outcome as excellent on final evaluation. No patients developed talar cysts, synovitis, or subtalar arthrosis, and none of the implants were noted to have displaced on final radiographs.

Postimplantation and postremoval radiographs demonstrating maintenance of alignment at 6 months after removal.
The average implant size was 9 (range, 6 to 12) mm. There was a trend noted within this case series for using smaller implants with increased experience. These were felt to reduce implant-induced irritation. The last implant that was size 10 or higher was used in April 2008.
DISCUSSION
An accessory navicular is one of the most common symptomatic accessory bones in the foot and has been reported to have a prevalence of 10% to 14% in the normal population. It is usually situated posteromedially and proximal to the navicular tuberosity.14,22 There is a significant gender predilection toward females, accounting for more than 80% of cases. 22 Most patients present between the ages of 11 and 15 with pain, tenderness, swelling, and a palpable protuberance along the medial longitudinal arch. 22 Symptoms are exacerbated by weight bearing, walking, sports, and shoe wear. The pain is thought to be caused by pressure on the bony prominence, abnormal biomechanics, and repetitive trauma to the fibrocartilaginous synchondrosis. 22 The synchondrosis experiences tension and shear forces as a result of the PTT and compression from subtalar pronation attributable to pes planus. 22 Diagnosis is usually both clinical and radiographic. Plain radiographs combined with MRI or scintigraphy can be used to localize the pathology to the accessory navicular and synchondrosis. 22 Initial treatment options are nonoperative, such as immobilization or orthotics; however, these frequently fail to relieve symptoms. 7 Most operative treatments have been successful at relieving pain. 22
Comparison of Preoperative and Final Follow-up Clinical and Radiographic Outcomes
Flattening of the arch is often associated with a type II accessory navicular and is thought to occur because of weakness of the PTT that attaches to the accessory navicular rather than the rest of the bone.14,22 Although numerous prior studies have described this association, to our knowledge, this is the first study to quantify the relationship. In our study, 34.8% of patients (38.6% of feet) with an accessory navicular had a concomitant planovalgus deformity. It has been theorized that stretching of the PTT around the accessory navicular causes weakness of the tendon and alteration of its line of pull and biomechanics, leading to flattening of the medial arch. 9,13,14,22 The accessory bone attachment location results in medial and dorsal displacement of the PTT insertion, which may change it from a supinator to an adductor while lengthening its lever arm. 22
The Kidner procedure was first described by Kidner in 1929 and has had great success in alleviating pain in patients with a symptomatic accessory navicular recalcitrant to nonoperative treatments. 8,9,2,18 It was later modified to include advancement of the PTT to the normal plantar and medial aspect of the navicular after excision of the accessory navicular, thereby theoretically recreating its arch-supporting function. 8,9,12,18,22
Several studies have shown that the modified Kidner procedure fails to correct the flattening of the arch, except in very young children, where correction has been attributed to growth rather than to the procedure. 11,13,14,17,22,23 Several procedures have been used to address flexible flattening of the medial arch, including tibialis posterior tendon reconstruction, flexor digitorum longus tendon transfer, spring ligament reconstruction, dorsal opening-wedge first metatarsal or medial cuneiform osteotomy, medializing calcaneal osteotomy, and lateral column lengthening. 22 In the pediatric population, subtalar arthroereisis has been utilized with success in correcting and maintaining the flexible deformity.6,26
Arthroereisis, which literally translates to “propping up,” was first described by Chambers in 1946 with the use of a bone block graft to fill the sinus tarsi. 20 The modern procedures utilize metallic or bioabsorbable conical or cylindrical implants placed into the sinus tarsi to restore the medial arch and correct the flatfoot deformity. 26 The implant works as an internal orthotic support, preventing excessive, nonphysiologic eversion of the hindfoot, without excessively limiting normal motion, while properly orienting the talus over the calcaneus.21,26 It has been utilized with success in the pediatric population and has gained support for its use in adult-acquired flatfoot deformity, showing similar successful results. 6,16,21,24,26 Furthermore, it has also been shown to protect medial soft tissue reconstructions as an adjunct procedure. 15,16,21,26 Various materials have been used for arthroereisis, including bone, silicone, bioabsorbable poly-l-lactic acid, ultra-high-molecular-weight polyethylene, and titanium. 20 There have also been multiple shapes described, including cylindrical, conical, spherical, and wine glass shaped.21,26 Arthroereisis is not without associated complications, such as persistent pain, loss of motion, avascular necrosis of the talus, intraosseous talar cysts, implant migration, reaction to implants, and subtalar arthrosis. 16,19,20,26 None of these were seen in our study. Postoperative sinus tarsi pain is the most common complication, usually requiring removal of the implant in up to a third of patients. 16,21,26 It may be caused by incorrect sizing of the implant and overcorrection,21,26 resulting in painful impingement, supination of the forefoot, and varus of the hindfoot. If too small, continued eversion may also be painful. 21 The risk of foreign-body reaction to the titanium MBA-type implant is minimal. 21 Implant migration and subtalar arthrosis are very rare and have not been reported. 21
In conclusion, this article reports the first use of subtalar arthroereisis to correct the planovalgus deformity associated with an accessory navicular resection. The results indicate that combining the modified Kidner procedure with subtalar arthroereisis can correct both the painful prominence and the hindfoot deformity. Even with implant removal, the deformity correction was maintained. This was attributed to the otherwise healthy PTT establishing an appropriate length after healing with the implant in position. Even when the implant was removed, the PTT was able to support the arch on its own, as it does in a person with normal arch mechanics. This finding is consistent with the experience with bioabsorbable implants where correction is maintained despite resorption of the implant. 22