
Abstract
Background: Failed total ankle arthroplasty (TAA) often results in significant bone loss and requires salvage arthrodesis. This study quantified the bone loss following failed TAA and reports the outcome of seven arthrodesis reconstructions using the Ilizarov method. Methods: A retrospective review of ankle fusions was performed for failed TAA to collect the mode of implant failure, presenting limb length discrepancy (LLD), total bone defect, postarthrodesis LLD, and treatment type (shoe lift versus distraction osteogenesis) and amount (shoe lift or lengthening). Results: Four mechanical failures and three infections were found. Four of seven cases had prior revision TAAs. Four of seven patients were treated with tibiotalar arthrodesis; three of the seven patients required talar resection and tibiocalcaneal arthrodesis. The mean presenting LLD was 2.2 (range, 1.2 to 3.5) cm. The mean time in frame was 197 (range, 146 to 229) days. With a mean postexplantation total bone defect of 5.1 (range, 3.7 to 8.5) cm, four of seven patients elected tibial lengthening following fusion [mean lengthening 4.6 (range, 2.5 to 8.0) cm; external fixation index (EFI) 42.6 (range, 16.5 to 55.6) days/cm)]. Three of seven patients were treated with a shoe lift [mean lift height 2.9 (range 2.5 to 3.2) cm]. There was no failure of fixation, refracture, or infection. All patients had a stable plantigrade foot and walked with minimal limp. Association for the Study and Application of the Method of Ilizarov (ASAMI) functional scores were six good and one fair. ASAMI bone scores were four excellent and three good. Conclusions: Ankle arthrodesis following failed TAA results in large LLDs secondary to bone loss during implant failure and subsequent explantation. External fixation can produce an excellent fusion rate in complex, possibly infected, failed TAAs. Limb length equalization (by either distraction osteogenesis or shoe lift) provides a means of obtaining good functional outcomes following failed TAA.
Level of Evidence: IV, Retrospective Case Series
Keywords
INTRODUCTION
There has been a resurgence of interest in total ankle arthroplasty (TAA) for the management of end-stage tibiotalar degenerative joint disease.12,41 Although survivorship of total ankle replacements has improved, recent analysis of registry data suggests the TAA failure rate is markedly higher than that of total hip or knee replacements, such that by 10 years a third of TAA patients should expect to require revision. 30 There are many contributions to these frequent failures, including mechanical implant loosening and subsidence, malalignment, dislocation, malleolar impingement, cement extrusion, syndesmotic nonunion, soft tissue imbalance, deep infection, persistent pain, and soft tissue envelope failure.4,52
When TAA does fail, a combination of bone loss and poor soft tissue envelope quality typically limits surgical options. Arthrodesis is frequently the preferred salvage procedure 15,19,26,56 ; however, revision arthroplasty has been reported with success. 23,36,56 The scarcity of talar bone stock and availability of appropriate revision implants and instruments contribute to the limited success of revision TAA. 28 In particularly difficult cases, transtibial amputation has been advocated. 4,18,28,48
A wide range of approaches to achieve stable arthrodesis following TAA failure have been reported. Published approaches include the use of external fixation with or without structural bone graft (most frequently iliac crest) 7,10,24,25,49 ; the use of plates, screws, and retrograde nails with or without structural bone graft 4%,8,12,15,20,33,52 ; and the use of trabecular metal graft in conjunction with a retrograde nail. 19 The frequent use of structural grafting material reflects both the loss of bone stock following explanation and concern for resultant limb length discrepancy (LLD). The concern for postarthrodesis LLD is appropriate because LLDs of greater than 10 mm can contribute to functional deficits 14,17,29 ; however, the exact pre- and postoperative LLDs expected with the various treatment options have not been well described.
Patient Demographics and Relevant Surgical History
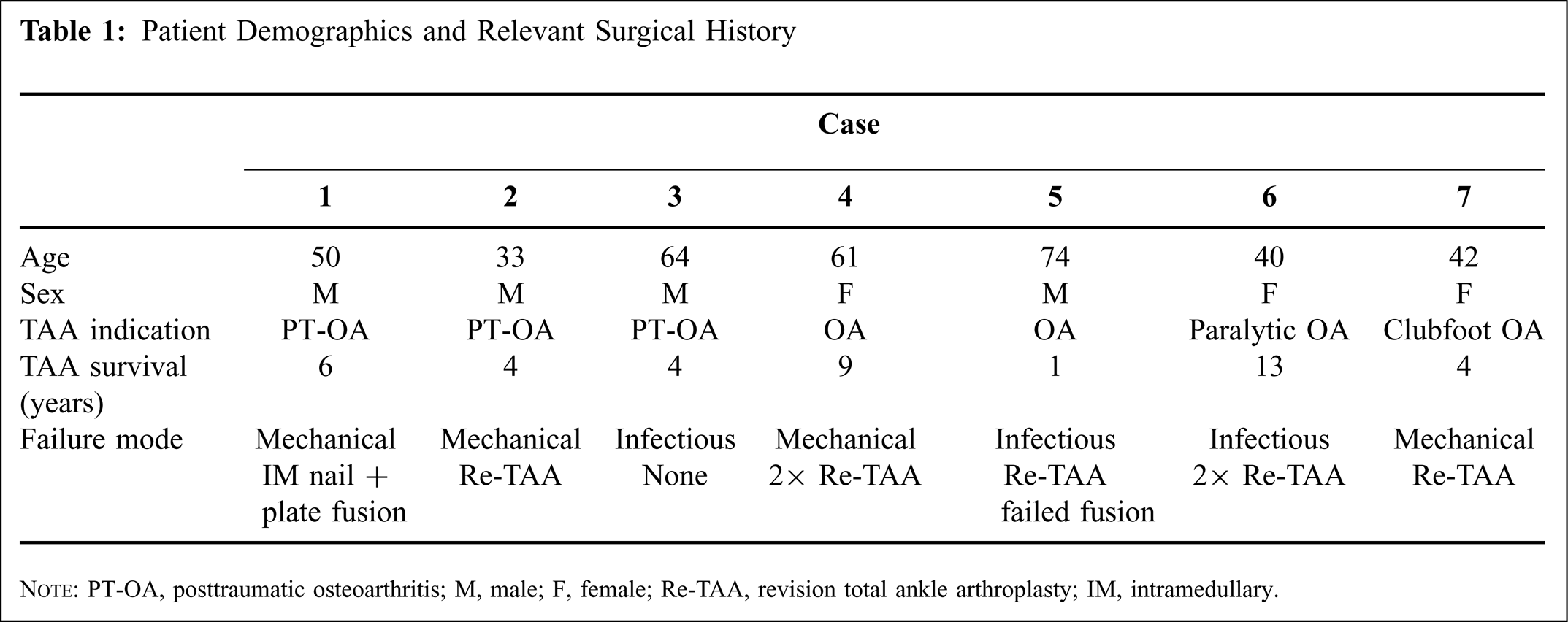
NOTE: PT-OA, posttraumatic osteoarthritis; M, male; F, female; Re-TAA, revision total ankle arthroplasty; IM, intramedullary.
The current study presents the results, with particular attention to the resultant bone loss and final LLD, of treating failed modern TAAs with circular external fixator–assisted arthrodesis and distraction osteogenesis for limb length equalization in lieu of structural graft materials. The purpose of this report was to describe the authors' experiences, complications, and results using modern external fixation as a means of addressing this complex problem, as well as to characterize and highlight the sources and amount of bone loss present in these cases.
METHODS
Patients were selected from the Institutional Review Board-approved limb-lengthening service database. All patients presenting to the senior authors (S.R.R. and A.T.F.) for arthrodesis following failed TAA were included. The mean follow-up available was 58 (range, 15 to 89) months. Patients presented an average of 5.9 (range, 1 to 13) years following primary TAA implantation. The observed modes of TAA failure were mechanical loosening (4/7) and implant infection (3/7). Five patients had undergone prior revision, two of whom had been revised twice for a total of seven prior revisions, and two presented with prior explantation and failed fusion elsewhere.
All data were collected by retrospective review of patient charts, operative reports, and x-rays. Standard demographic data as well as relevant surgical history (as reported in Table 1) were collected from office charts. Bone defects were collected from operative reports and patient charts and reconfirmed on calibrated radiographs when available. Special attention was paid to adverse events encountered during the course of treatment. The amount of time spent in external fixation for arthrodesis and lengthening (in those electing lengthening) was recorded from office charts. All limb length discrepancies were measured on 51-inch standing radiographs (Figure 1). The time spent in fixation was used in conjunction with the amount of lengthening to calculate the external fixation index (EFI) for each patient. (The EFI is defined as days in fixation per centimeter lengthened.) Postoperative Association for the Study and Application of the Method of Ilizarov (ASAMI) scores were calculated for all patients. 47 Adverse events were categorized as problems (resolved fully with nonoperative care), obstacles (resolved fully with operative care), and true complications (could not be fully resolved). 40
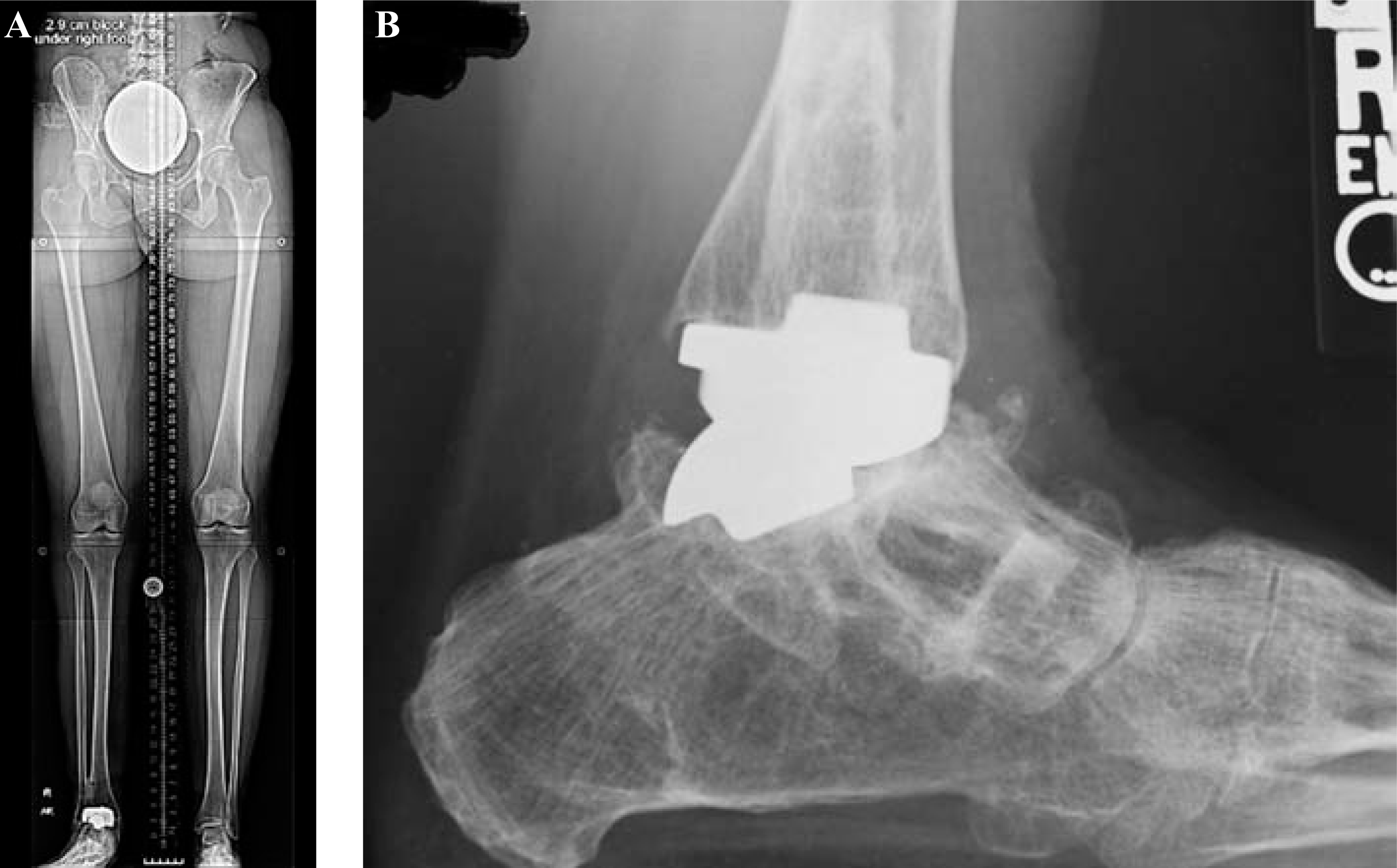
Example of failed ankle replacement and preexisting LLD.
A total of seven patients were identified and included: three women and four men at an average age of 52 (range, 33 to 74) years. Four underwent tibiotalar arthrodesis, whereas three required direct tibiocalcaneal fusion following complete talar resection. The indications for primary TAA included three cases of posttraumatic osteoarthritis (OA), two cases of primary OA, one case of postparalytic OA, and one case of OA attributed to clubfoot. One patient received autologous local bone graft, one patient received autologous local bone graft with bone morphogenic protein (BMP) putty (OP1, Stryker, Mahwah, NJ), and one patient received BMP putty alone. The remaining patients received no augmentation.
Descriptive statistics were calculated using Microsoft Excel (v2007, Microsoft, Redmond, WA). Given the sample size, cross-group comparative analysis was deemed inappropriate and no pvalues were calculated.
OPERATIVE TECHNIQUE
The ankle was approached from both the lateral and medial sides. The fibula was excised just above the level of the planned tibial cut to allow for the shortening needed to close the postexplantation bone defect. The failed implant excision was done en bloc and bone quality and residual bone stock were assessed. The tibial cut was performed perpendicular to the tibia, whereas the talus was cut parallel to the plantar plane of the foot. If, following talar implant excision, the residual bone quality and quantity were suboptimal, the talus was excised completely and os calcis surface was used to achieve fusion (Figure 2). Soft tissue and bone cultures were sent to rule out residual infection. Preoperative antibiotics were held until after the cultures were retrieved during surgery. The bone surfaces were prepared and opposed verifying final foot alignment. A two-ring Ilizarov apparatus was mounted around the ankle in compression using either rods or Taylor Spatial Frame (TSF) struts. In those cases with prohibitively large bone defects or soft tissue gapping following acute shortening, gradual shortening was used. The use of gradual shortening was dictated by the soft tissue envelope and ability to close the operative wounds while maintaining tibialis posterior and dorsalis pedis pulses. The Ilizarov apparatus was kept on the leg for 4 to 6 months to achieve solid fusion.
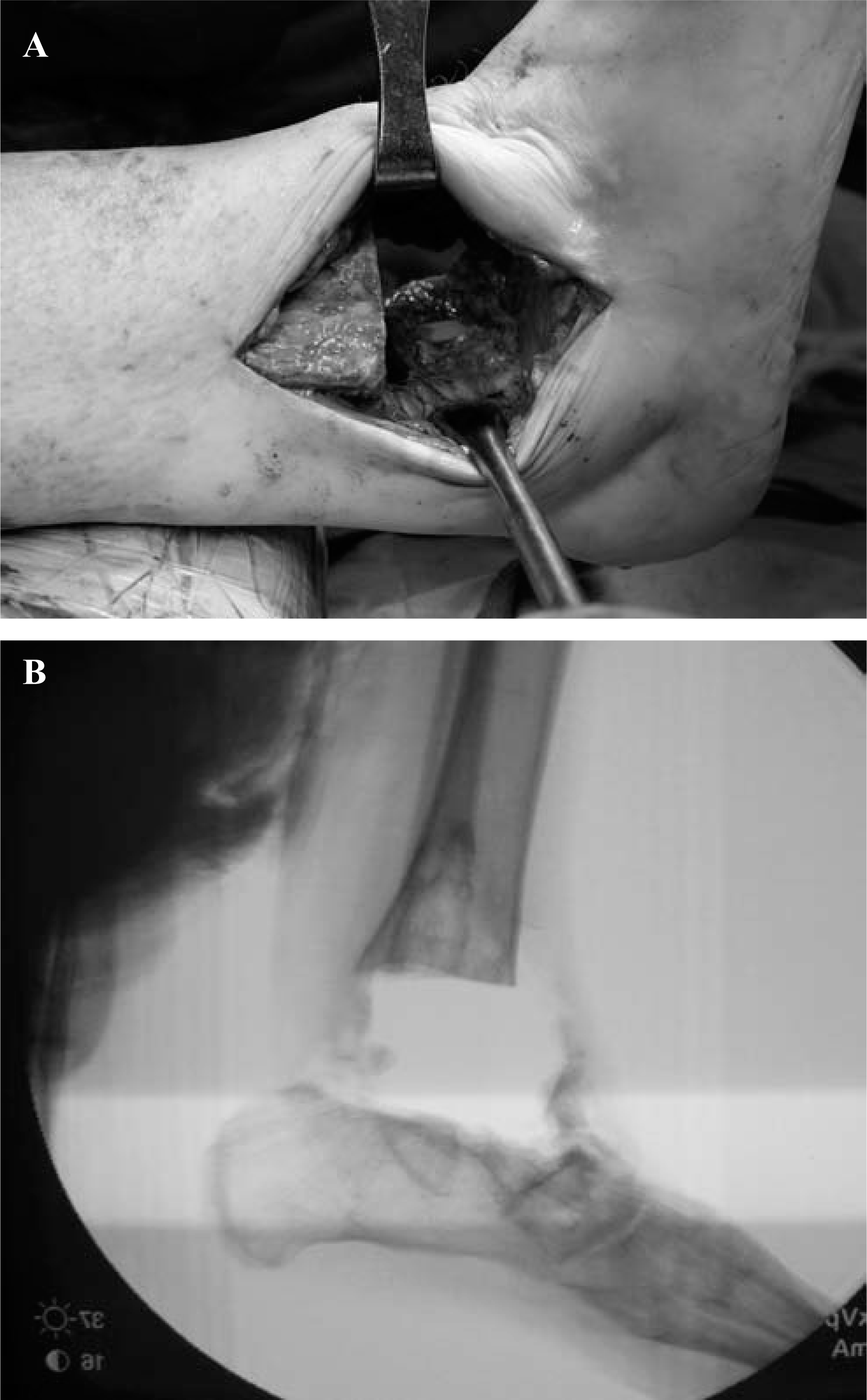
Same patient as in Figure 1.
The risks, course of treatment, and expected results of gradual lengthening and lifetime shoe modification were discussed with all patients and a shared decision was reached regarding optimal management for each patient. For those patients who elected lengthening for LLD equalization, a proximal tibia and fibula osteoplasty was performed 4 to 8 weeks following the ankle arthrodesis surgery. This procedure staging was designed to minimize the total time a patient spent in external fixation by overlapping the time spent in the fusion frame and time spent in the distraction frame. In most cases, bony union, not regenerate consolidation, dictated frame removal. If infection was present, the lengthening operation was delayed until the patient completed a standard course of intravenous antibiotics. During the lengthening operation, an additional TSF block was mounted on top of the existing fixator (Figure 3). The lengthening was done using either the classic or hybrid method (Figure 4). Either lengthening and then nailing (LATN) (Figure 5) or lengthening and then plating (LAP) were chosen as hybrid techniques to shorten the time in frame, allowing both fusion and lengthening fixators to be removed simultaneously.45,51 After frame removal, a short leg cast was applied for the transition.

Same patient as in Figure 1. End of distraction standing picture.
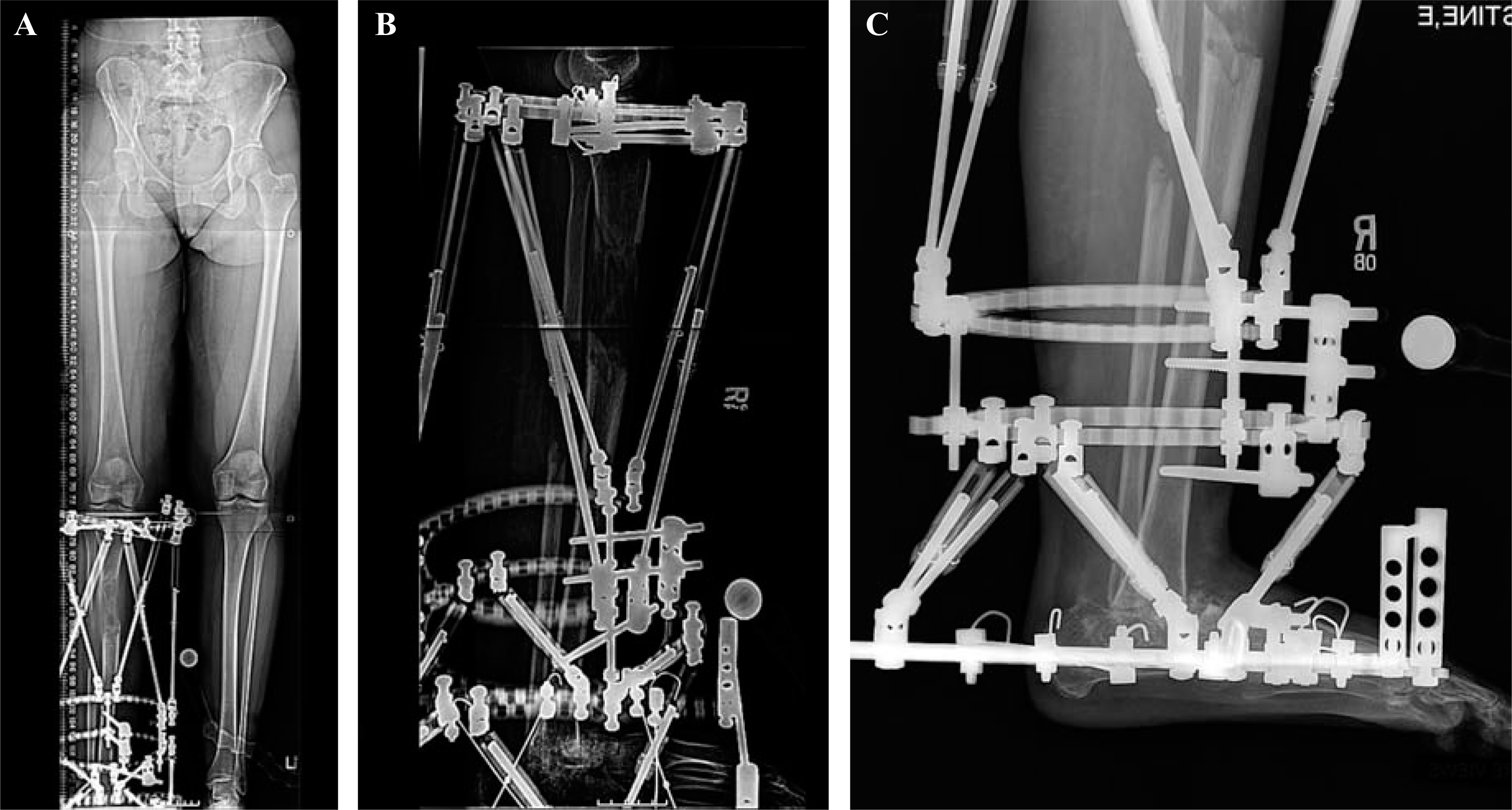
Same patient as in Figure 1.

Same patient as in Figure 1.
RESULTS
All patients presented with a LLD. The average LLD on presentation was 2.2 (range, 1.2 to 3.5) cm. Operative resection increased the total bone deficit by 2.9 (range, 1.0 to 5.0) cm. In three of seven cases, this resection included talar sacrifice and was associated with an average resection of 3.7 (range, 3.0 to 5.0) cm. In four of seven cases, the talus was spared, resulting in an average resection of 2.3 (range, 1.0 to 3.8) cm. The combination of presentation LLD and resection resulted in an overall mean postexplantation bone deficit of 5.1 (range, 3.7 to 8.5) cm. Patients spent an average of 197 (range, 149 to 229) days in the fusion frame. The four patients undergoing tibiotalar fusion spent an average of 186 (range, 149 to 229) days in fusion fixation, whereas those undergoing tibiocalcaneal fusion spent an average of 212 (range, 190 to 229) days in fusion fixation (Table 2).
Four of seven patients elected lengthening as primary management of their postarthrodesis bone deficit and LLD, whereas three of seven chose a shoe lift as primary management of their post-LLD. Those who elected lengthening had an average age of 44 (range, 33 to 61) years and had a mean bone deficit of 5.7 (range, 3.7 to 8.5) cm, whereas those electing to wear a lift were on average 62.6 (range, 50 to 74) years old and had a mean bone deficit of 4.4 (range, 3.7 to 5.2) cm. The four patients who elected lengthening were lengthened by an average of 4.6 (range, 2.5 to 8.0) cm. These patients spent 162 (range, 132 to 189) days in the frame, resulting in an average EFI of 42.6 (range, 16.5 to 55.6) days/cm. One of four lengthenings was done using LATN and another patient was lengthened using LAP. The three patients who elected to use a shoe lift were fitted with an average lift of 2.8 (range, 2.5 to 3.0) cm (Table 3).
All patients obtained solid pain-free fusion as planned. Despite fibular excision, all patients have maintained appropriate subtalar joint alignment. Six patients showed an ASAMI function score of good, and one showed a score of fair. Because the ASAMI function score includes ankle range of motion, the fusion group's highest possible function score was “good.” Four patients had an ASAMI bone score of excellent and three had a score of good. The group undergoing lengthening was uniformly excellent, whereas those electing a shoe lift were uniformly good with respect to bony outcome as a result of their persistent LLD.
A low rate of significant adverse events was observed. In total there were six problems, zero obstacles, and zero true complications. The problems encountered were four pin-tract infections that resolved with oral antibiotics, one wound breakdown treated with dressing changes, and one painful wire removed in the office.
DISCUSSION
Failed TAA is not uncommon and its management is challenging. Although the survival rate of modern ankle prostheses is much improved, it has not reached that of total hip or total knee arthroplasties. 30 The 5-year reoperation-free survival for total hip and knee arthroplasties may be in excess of 95%, whereas the 5-year reoperation-free survival rate of modern TAA has been reported at 54%, with an implant survival rate of 80%. 2,5,44,48,55 Although some authors have reported successful revision in two-thirds of cases, revision arthroplasty has been less successful in other series, and literature on multiple revisions is scarce. 16,27,28,48,49 When revision arthroplasty is either undesired or impractical, salvage options include transtibial amputation and arthrodesis.
None of our patients were considered candidates for (re)revision TAA at the time of referral to our service; however, five of seven patients had undergone a total of seven prior TAA revisions. In keeping with past reports, it was found the most common causes of unsalvageable implant failure were mechanical loosening and infection. In our patients, TAA failure came at the expense of significant bone stock. Unsurprisingly, all patients had a preoperative limb length discrepancy that was on average 2.2 cm. Operative resection for explantation or nonunion repair increased the total bone deficit an average of 2.9 cm. Finally, the process of arthrodesis can contribute as much as 1 cm to total bone deficit regardless of the method used.32,34 Thus salvaging failed TAA with ankle arthrodesis has the potential to create significant bone deficits. In our patients, the mean total deficit was 5.1 (range, 3.7 to 8.5) cm.
Operative Course
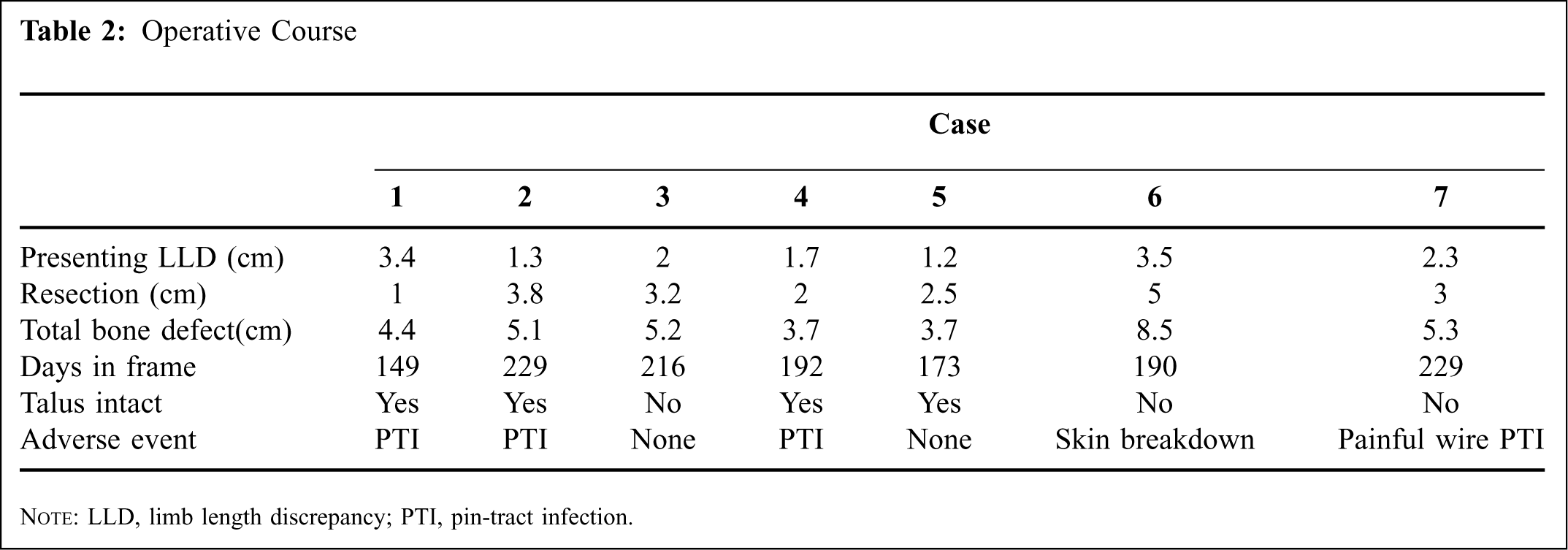
NOTE: LLD, limb length discrepancy; PTI, pin-tract infection.
Surgical Outcomes
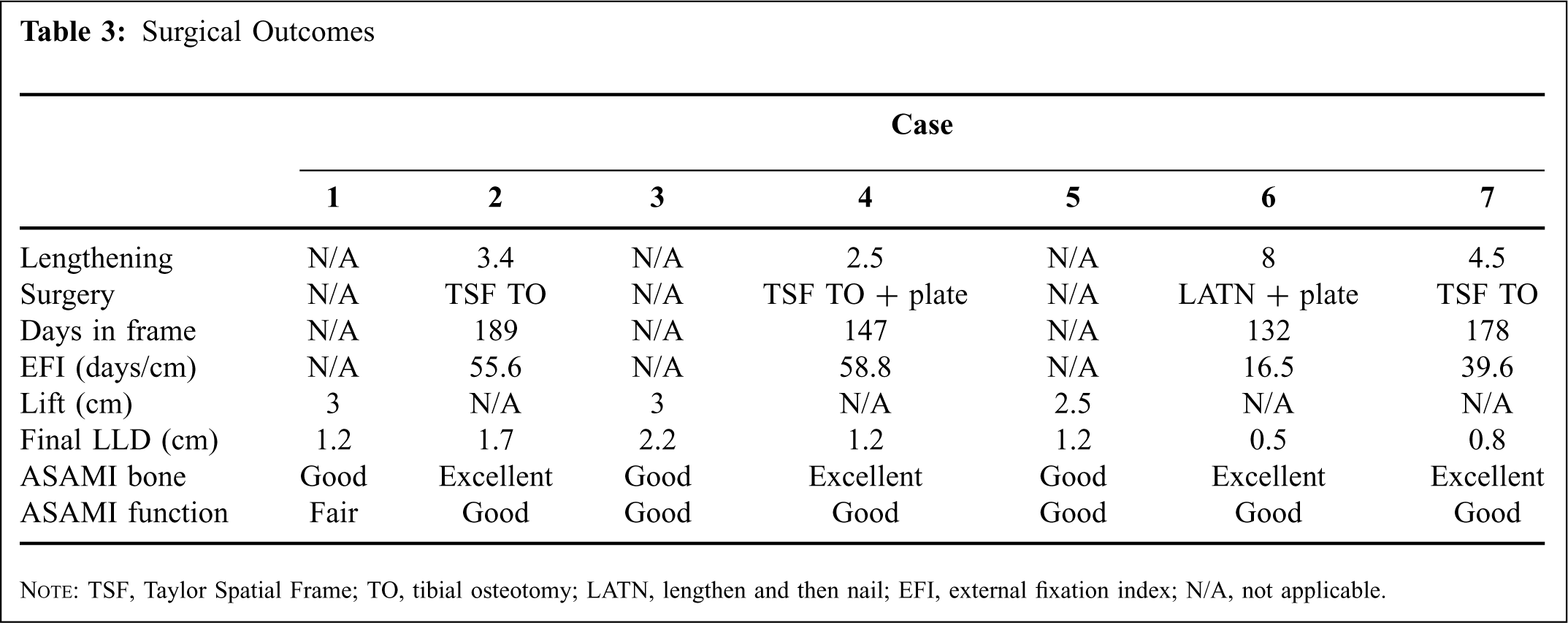
NOTE: TSF, Taylor Spatial Frame; TO, tibial osteotomy; LATN, lengthen and then nail; EFI, external fixation index; N/A, not applicable.
In light of this bone deficit, arthrodesis in the setting of failed TAA presents two distinct challenges: achieving adequate fixation for fusion and addressing the potentially sizable bone deficit. Our practice is to address these challenges separately in a staged fashion. In the index operation, we perform the arthrodesis and apply compressive external fixation and treat any infection. Four to eight weeks following the index operation, the patient's total LLD is apparent, and infection, if present, has been adequately addressed. The LLD is then treated using either distraction osteogenesis or a shoe lift according to the patient's wishes. In our series, younger patients (44 versus 62.6 years) with larger LLDs (5.7 versus 4.4 cm) were more likely to elect lengthening. Regardless of the patient's preferred means of limb length equalization, our goal was to leave the fused leg 1 cm shorter than the unaffected leg to allow for toe clearance.
Using modern hybrid circular external fixation as a means of stabilizing the fusion, we achieved a 100% fusion rate with an average of 197 days in the frame. This result is comparable to previous reports using this fusion technique for other indications, which have shown 80% to 100% fusion rates over 96 to 240 days in the frame. 22,46,51,54,57,59 Noncircular external fixation was one of the first techniques described for fusion following failed TAA and has been reported to have an 81% to 89% success rate. 10,25,38,49 More recently, authors have shown success with internal fixation as a means of stabilizing the arthrodesis, reporting fusion rates of 74% to 94%. 4,12,20
A variety of approaches to the sizable bone deficit exist. Autograft, most often iliac crest, was initially described and continues to be used effectively 7,9,12,16,49 ; however, a wide range of donor site morbidities have been described and are a concern when this technique is used. 1,3,39,58 Allograft, particularly femoral head, has also been used successfully in complex ankle reconstructions 11,13,21,37,52 ; however, the use of allograft carries a risk of latent infection, decreased mechanical strength following sterilization, and an increased risk of fracture, collapse, or nonunion. 6%,31,35,42,43,50,53 In addition to structural bone grafts, there are limited reports of novel structural grafts, including trabecular metal and cages filled with bone chips.8,19
This defect was addressed with either a shoe lift or staged tibial lengthening. 22,46,51 Distraction osteogenesis via the Ilizarov method has significant theoretical advantages when compared with the various graft materials. The regenerate bone has the biological merits of autograft but no risk of donor site morbidity. Successful regenerate bone is free of the mechanical and biologic compromise inherent in allograft preparation as well as the possibility of latent infection. Because the resulting regenerate is a biologically active, fully incorporated living structural tissue, this option is particularly appealing in younger patients. In the setting of failed TAA, staged lengthening has particular appeal because it allows for limb length targets to be determined after ankle fusion bony apposition has been set in the frame. With this approach, optimal bone contact is achieved at the ankle fusion site and accurate assessment of the postarthrodesis LLD (bone defect) can be done. The patient and surgeon can then make a more informed decision regarding further treatment with limb lengthening or a shoe lift. Both options allow precise adjustment of limb length to patient comfort. When compared with acute lengthening with bulk allograft and internal fixation, our approach produced equivalent to superior rates of bony union, optimal limb length equalization even in patients with large bone defects, and freedom from allograft collapse or latent disease transmission risk. Additionally, because the reconstruction does not rely on indwelling hardware or dead bone, there is less concern when working in an infected field. Given that the patients in this series had LLDs of 3.7 to 8.5 cm and four of seven ankles failed because of infection, external fixation for fusion and lengthening offers an appealing treatment option for these failed total ankles.
The Ilizarov method has limitations. Many patients are not interested in long-term external fixation, whereas others tolerate the frame poorly. Hybrid techniques such as LATN and LAP can reduce the amount of time spent in external fixation and the risk of early regenerate fracture. The use of BMP at the fusion site may also decrease the external fixation index. Half of the lengthenings in this series used a hybrid technique. Although patients are initially apprehensive about the frame, in our experience, circular external fixation is well tolerated on the distal lower extremity. In this series, there were no complications and no obstacles. The most common problem was pin-tract infection successfully treated with oral antibiotics. The only other problem was a painful foot wire, which was successfully removed in the office. To date there have been no cases of regenerate fracture or reoperation.
This case series is not without limitations. The most obvious limitation is the small sample size. A larger sample would be desirable to enhance generalizability. Given the small sample size and large number of failed prior revisions within this series, it is possible that the large bone deficits observed were unique to failed revisions. Additionally, there may be a significant referral bias inherent in the study by the nature of our practice. Ours is a subspecialty limb-lengthening and complex deformity correction service with significant limb salvage experience at an academic medical center. In spite of these limitations, we feel the design and content of this report are adequate to support its wholly descriptive conclusions.
Compression via hybrid circular external fixation can be a highly successful means of salvaging complex, frequently infected, failed TAA in a reasonable amount of time. These constructs can optionally be extended and used as part of staged lengthening to address total bone deficit following fusion. Patients with failed TAAs present with functionally significant LLDs; as such, they often require lengthening and not simply a preservation of preoperative length. Limb length equalization (by either distraction osteogenesis or shoe lift) provides a means of obtaining good functional outcomes following explantation and fusion. As such, both patients and surgeons should know that the staged gradual lengthening option exists and can produce good to excellent results. Finally, we believe that LLD is important to a patient's final functional status and should be reported with other results of salvage.