
Abstract
Level of Evidence: V, Case Report
Keywords
INTRODUCTION
Surgery has traditionally been the gold standard for managing established symptomatic fracture nonunion. 7 Noninvasive treatments include high-energy extracorporeal shock wave therapy (ESWT), low-intensity pulsed ultrasound, and focused electromagnetic field therapy. Their intended benefit is through the promotion of new bone formation to achieve fracture consolidation without the additional morbidity, cost, and possible complications associated with surgery. 6,8
The relatively immobile “keystone” of the second tarsometatarsal joint provides the foot with the greatest stability in plantarflexion. Therefore, it is important to recognize and manage the pathology in this area in its early stages. The tendency to develop a stress fracture through the base of the second metatarsal is more often seen in professional ballet dancers, because of the repetitive and sustained forces applied through the second tarsometatarsal joint when en pointe. 11 Some may continue to dance through their symptoms for as long as possible before seeking advice, thereby increasing their risk of fracture nonunion, which is a rare and difficult condition to manage. 11,13
This report describes the successful treatment of established fracture nonunion involving the base of the second metatarsal in two professional dancers using pneumatic low-energy ESWT. Fracture consolidation was achieved in both cases with no complications and an early return to activity.
CASE REPORT
Patient 1
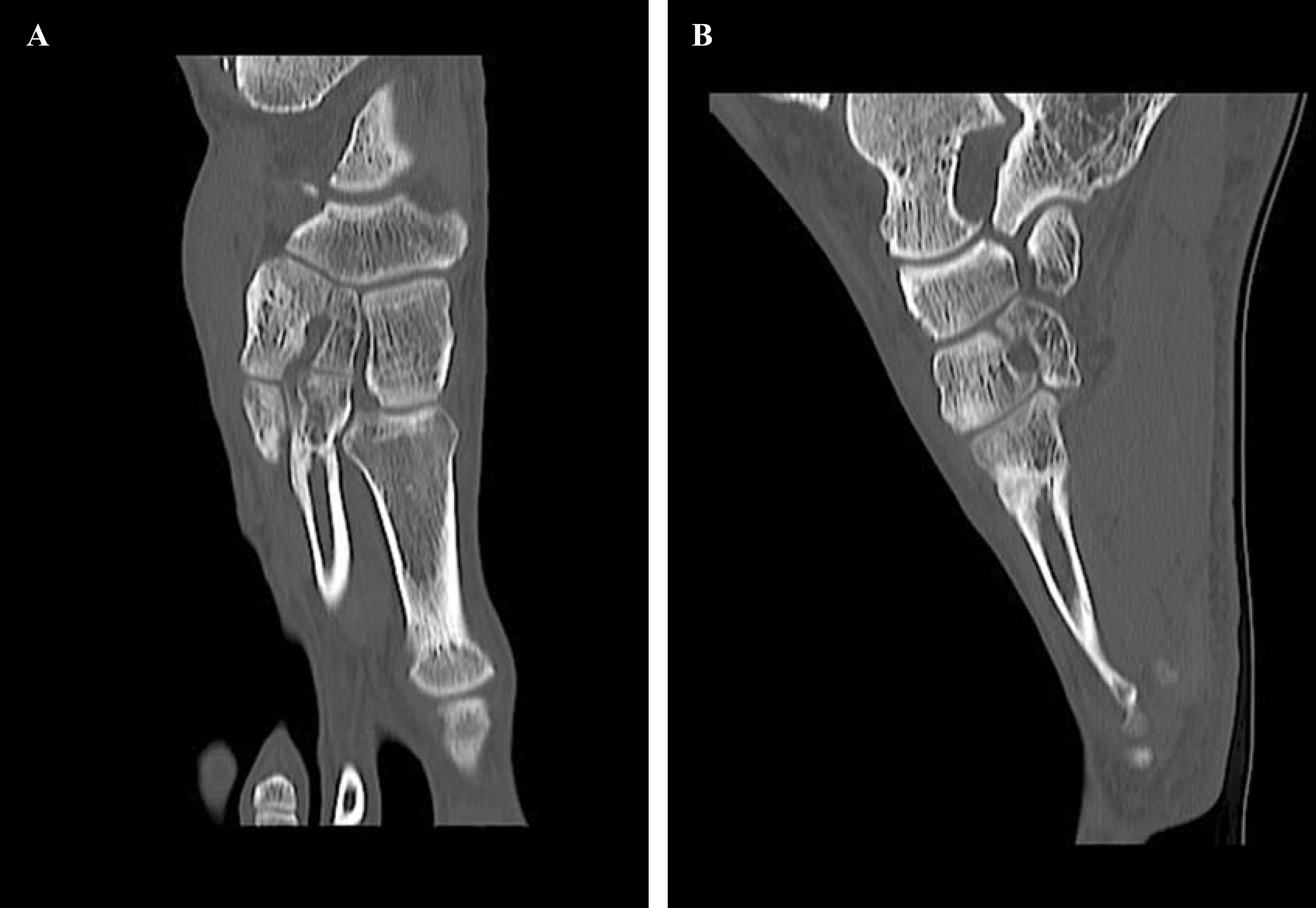
A 22-year-old female contemporary dancer fractured her second metatarsal base after a fall, following which she was managed nonoperatively with 6 weeks of non–weight bearing and a further 4 weeks of protected weight bearing in a boot. The patient returned to dance at 4 months despite ongoing pain. Repeat radiographs demonstrated a delayed union and a further period of protected weight bearing was instructed. At 2 years, pain was still present and a second opinion was sought from the senior author (JDC). At this time, the patient demonstrated residual tenderness at the base of the second metatarsal, which was shown on radiographs to be an established fracture nonunion (Figure 1).

Sagittal CT section of patient 1 showing a fracture nonunion of the second metatarsal base before treatment with low-energy ESWT.
Low-energy ESWT was administered directly over the fracture site during three consecutive outpatient clinic visits at weekly intervals. A treatment plan of 3,000 impulses at 0.2 mJ/mm2 was provided at each visit. Local anesthetic was not required. Nonsteroidal anti-inflammatory drugs were avoided until fracture union was confirmed. The patient was advised to abstain from dancing for 6 weeks and to mobilize with a flat postoperative shoe until recovery.
At follow-up, the pain had greatly improved and, by 3 months, she was pain free. At this time, repeat radiographs demonstrated radiological union, which was also confirmed by computed tomography (CT) (Figure 2). Dance was slowly reintroduced at 14 weeks and she was back to full training by 19 weeks. The patient remained pain free at her 6-month follow-up.
Axial (
Patient 2
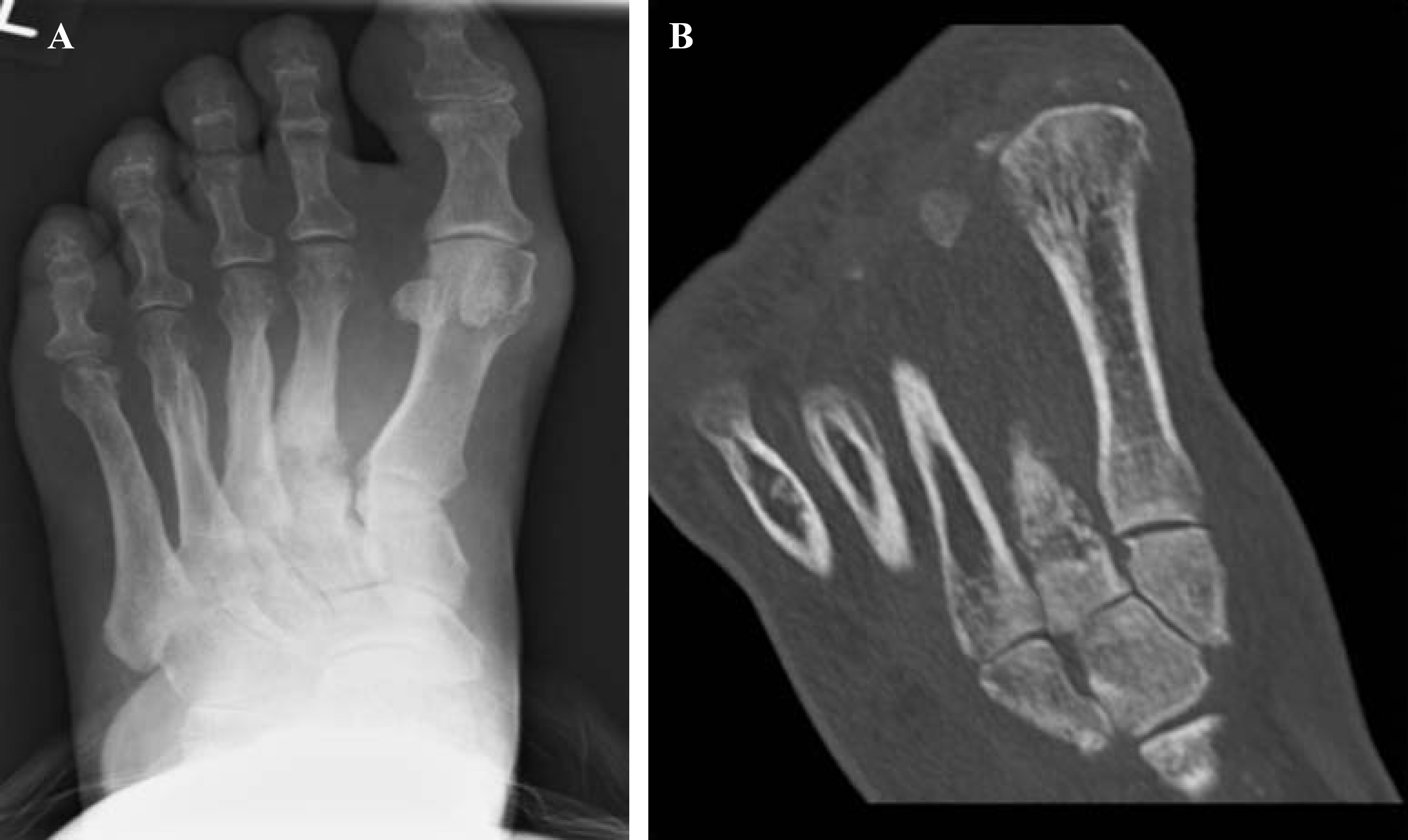
A 29-year-old female ballet dancer presented with a 6-month history of continuing pain at the base of the second metatarsal. The patient's symptoms first began with an insidious onset of midfoot pain exacerbated by training and progressively got worse over a period of 6 weeks. She was diagnosed with a stress fracture and was advised to avoid dance and follow a period of protected weight bearing in a boot for 3 months. Despite this, there was no improvement in the patient's symptoms and at 6-month follow-up, the patient remained tender over the fracture site. A repeat radiograph identified a widened fracture site with sclerotic edges and a diagnosis of fracture nonunion was made (Figure 3).

Anteroposterior (AP) radiograph (
The patent received a course of low-energy ESWT as outlined above and did not require local anesthetic. At 3 months, the patient reported no pain (Figure 4) and was able to return to training 14 weeks after the start of therapy and, over the following 7 weeks, was able to get back to full training and perform en pointe. The patient remained pain free at 1 year (Figure 5).

AP radiograph (
AP radiograph (
DISCUSSION
In addition to the tibia and fifth metatarsal, stress fracture of the second metatarsal is one of the most common sites of injury seen among elite athletes and, in particular, ballerinas. 1,3 These can often present late with an insidious onset of pain, swelling, and an inability to fully weight bear. The pressure to compete may also influence a premature return to sport without allowing for adequate healing to occur. Ballet dancers are particularly at risk for lesser metatarsal fractures because of the forces exerted while en pointe. Because of its locking keystone configuration with the surrounding tarsal bones, the second ray provides the forefoot with the greatest stability, which explains why it is particularly prone to stress fractures. 11 Nonunion of second metatarsal stress fractures is, however, extremely rare. 13 Also, in females, nonunion and delayed union may result from the triad of malnutrition, amenorrhea, and osteoporosis, which not only predisposes these patients to fracture but also results in poor healing potential. 13,18
Currently, the main use of low-energy ESWT is in the treatment of chronic enthesopathies refractory to conservative management, such as Achilles tendinopathy and plantar fasciitis. 14,15 The core benefits of low-energy ESWT are related to its safety, ease of use, and ability to provide therapy in an outpatient clinic setting without the associated complications of surgery or an anesthetic. 5,7 It differs from high-energy ESWT in terms of the energy flux density generated, with low-energy defined as less than 0.2 mJ/mm2 and high-energy greater than this. 8 Low-energy ESWT can be uncomfortable and occasionally painful, although a short burst of therapy is usually well tolerated. Rarely, it may be necessary to administer a local anesthetic or sedation, which is the usual requirement for the high-energy form of ESWT. 14 –16
Therapeutic shock waves are more traditionally used for the noninvasive treatment of urolithiasis. One of the side effects was an observed increase in pelvic bone formation, 9 later prompting work to establish its effectiveness in the management of fracture nonunion or delayed union. 5,16,17,19,20 The underlying mechanism is yet to be fully explained, but from a variety of animal models and biochemical studies, we know that high-energy ESWT can promote neovascularization and lead to the release of osteogenic growth factors. 8,10,20
Since its first clinical application in 1991 as a means of enhancing fracture healing, 19 the high-energy form of ESWT has been increasingly employed in the management of fracture nonunion, avascular necrosis, and delayed union of stress fractures involving both long and small bones. 2,5,8 In their systematic review, Birnbaum et al. found the success rate of high-energy ESWT to be anywhere between 75% and 91%. 4 Later studies have shown similar results and have gone on to highlight the minimal complications associated with ESWT when compared with surgery. 6,7,21 However, unlike the low-energy form of ESWT, high-energy ESWT requires a hospital admission for a regional or general anesthetic.
To the best of our knowledge, this report demonstrates the first clinical application of low-energy ESWT to successfully treat fracture nonunion of the lesser metatarsals. There is only one description of second and third metatarsal stress fractures among ballet dancers that were treated with low- to medium-energy ESWT. 1 However, this report focused on the acute management of these fractures and did not show its application in managing nonunion or delayed union.
In a separate series of six soccer players with fractures of their fifth metatarsal, five presented with delayed union and one with established nonunion despite operative fixation. 12 All underwent low-energy ESWT. Radiographic consolidation occurred between 6 and 12 weeks later, with full return to activity approximately 4 months after start of treatment. As a result, we believe low-energy ESWT should be considered as a first-line treatment option for any patient presenting with a painful delayed union at 3 months where there is no indication of callus or healing on a CT scan. This can be safely administered before consideration for surgical fixation with or without bone graft, if required.
SUMMARY
In summary, this report describes a novel approach to the treatment of nonunion or delayed union of lesser metatarsal fractures. Low-energy ESWT is noninvasive and can be safely applied in an outpatient clinic with no need for an anesthetic. The overall evidence base for using low-energy ESWT to treat fractures remains weak and a randomized controlled trial comparing it to high-energy ESWT is warranted.