
Abstract
BACKGROUND:
Following ankle sprain, residual symptoms are often apparent, and proprioceptive training is a treatment approach. Evidence, however, is limited and the optimal program has to be identified.
OBJECTIVE:
To investigate the effects of two post-acute supervised proprioceptive training programs in individuals with ankle sprain.
METHODS:
Participants were recruited from a physiotherapy center for ankle sprain rehabilitation. In a pre-post treatment, blinded-assessor design, 22 individuals were randomly allocated to a balance or a proprioceptive neuromuscular facilitation (PNF) group. Both groups received 10 rehabilitation sessions, within a six-week period. Dorsiflexion range of motion (ROM), pain, functional and balance performance were assessed at baseline, at the end of training and eight weeks after training.
RESULTS:
Follow-up data were provided for 20 individuals. Eight weeks after training, statistically significant (
CONCLUSIONS:
Balance and PNF programs are recommended in clinical practice for improving ankle ROM and functional performance in individuals with sprain. Balance programs are also recommended for pain relief.
Introduction
Lateral ankle sprains are among the most common musculoskeletal injuries and account for 80% of total ankle injuries [1]. For most individuals, conventional treatment is the initial preferable strategy, comprising early mobilization and weight-bearing of the ankle, unsupervised exercises and sometimes use of external support (bandage, brace or tape). Prognosis is typically a decrease in disablement within two weeks [2]. Nevertheless, a considerable number of these individuals report residual symptoms and experience an insufficient recovery up to three years after the sprain, irrespective of the injury severity [2].
Among residual symptoms, deficits in the functional performance of daily activities are common up to 18 months post-injury in generic clinic populations [3]. For athletic populations, functional deficits have been found up to two years after the sprain [4]. Furthermore, findings from a systematic review in 18 studies show that 5% to 33% of conventionally treated sprains produce pain one to three years post-injury [2]. One reason for the persistence of functional deficits and pain may be limited ankle ROM. Limited dorsiflexion ROM is often apparent to individuals with conventionally treated sprains [5, 6], and without proper rehabilitation this may result in recurrent episodes of giving way and chronic ankle instability [7]. The risk for chronic ankle instability is also increased in individuals who exhibit poor balance performance [8], indicating the importance of proprioceptive training after the sprain.
For individuals with sprain, the high incidence of residual symptoms and the risk for developing chronic ankle instability require identification of the optimal approaches for rehabilitation. Systematic reviews reveal the benefits of supervised training for sprains [9, 10], and until now the effects of various programs have been investigated. Published clinical guidelines for sprains recommend participation in proprioceptive training, which consists of balance activities and exercises promoting functional movements [11]. Proprioceptive training is thought to promote afferent signals and sensory feedback from the ankle proprioceptors to the central nervous system in order to improve sensorimotor function and maintain orientation during activities [12]. Guideline recommendations, however, are based on weak evidence, as relevant studies exhibit methodological limitations, including assessment bias, poor description of sample characteristics and inappropriate handling of missing data [11]. Moreover, the conclusions from a recent systematic review and meta-analysis in individuals with ankle ligament injuries, such as sprain and chronic instability, underline that proprioceptive exercises may improve functional outcomes, but there is no consensus on using proprioceptive exercises to improve balance performance [12]. The reviewers mention that until now there are no studies investigating effectiveness of proprioceptive exercises on ankle ROM, and point out the need for further research into the effects of different proprioceptive training programs in individuals with ankle sprain and chronic instability [12].
For individuals with ankle sprain, there is limited evidence for effectiveness of proprioceptive training programs, and in relevant studies investigators have utilized multi-component rehabilitation protocols, including balance training. In particular, a rehabilitation protocol that consisted of balance and strength training, stretching and running activities was capable of improving functional performance [13]. Balance performance has also been improved following participation in balance and strength training [14], but not following participation in balance training and running activities [15]. In addition, wobble board and strength exercises, mobilization techniques and cryotherapy were able to reduce pain, but similar reduction in pain has been reported following bandage support and immobilization [16, 17]. The effects of proprioceptive training on ankle ROM have not been investigated until now.
Proprioceptive neuromuscular facilitation (PNF) is another proprioceptive training technique, which is designed to stimulate proprioceptors and promote response of neuromuscular mechanisms [18]. The patterns of PNF techniques emphasize multi-planar movement, and they have diagonal direction with goal to stimulate functional movements through strengthening (facilitation) and relaxation (inhibition) of muscle groups [18]. Despite that PNF techniques are commonly used in clinical practice, there is still limited research evidence investigating effectiveness in ligament injuries [19], whereas there is lack of studies concerning the rehabilitation of ankle sprains. Taking into consideration that the application of PNF patterns is comparable to the performance of functional movement patterns [18], it is suggested that PNF training may improve functional and balance performance in individuals with sprain. Moreover, as PNF techniques have already been used in musculoskeletal rehabilitation in order to improve articular ROM and pain [20, 21], they may also be capable of improving dorsiflexion ROM and pain after the ankle sprain.
Although multi-component protocols are commonly used for the rehabilitation of sprains, investigating one specific component, such as proprioceptive training, in a controlled research setting will enable us to reveal effectiveness of a single approach. Since proprioceptive training alone has the potential to improve multiple deficits after the sprain, this could save time for both therapists and sprained individuals. Balance training has already been established in literature as the most commonly used protocol of proprioceptive training for sprains [13, 14, 15, 16, 17]. In this context, it would be beneficial to compare the effectiveness of balance and PNF training for the first time. Hence, the objectives of this study were to investigate the effects of two supervised balance and PNF training programs on dorsiflexion ROM, pain, functional and balance performance in individuals with ankle sprain.
Methods
The present study was undertaken in accordance with the principles outlined in the Declaration of Helsinki and it was prospectively registered at a clinical trial registry (ID: NCT01853462). The study design consisted of randomized groups and pre-post treatment with a blinded assessor.
Participants
A total of 34 individuals who were referred to a physiotherapy center for ankle sprain rehabilitation were initially invited to participate. They had sustained a post-acute sprain to the ankle and experienced pain in the performance of functional or sports activities. To be included, it was required that the individuals were 18 to 40 years, with a clinical diagnosis of ankle sprain by an orthopedic specialist, and their sprain had been conventionally treated. Individuals with grade III sprains were excluded. Individuals who had sustained a sprain to the medial ligaments or the interosseous (syndesmotic) ankle ligament were not included. Additional exclusion criteria were: concurrent fracture, chronic ankle instability, history of ankle surgery, lower limb nerve injuries and further ankle injuries after the sprain. Individuals with any injuries that hindered participation in training were not included.
The eligibility criteria of the study were initially screened by the principal investigator, via an interview. In addition, all prospective participants were instructed to show any relevant documentation of the clinical diagnosis of the sprain and the results of diagnostic testing, such as radiographs, ultrasonography or magnetic resonance imaging, in order to confirm the grade and the ankle ligaments affected. An orthopedic specialist confirmed suitability for participation and obtained a thorough medical history of the ankle sprain, including information concerning the aetiology and mechanism of injury, conventional treatment of choice and symptoms. The principal investigator also performed a physical examination, including palpation of bony and ligamentous structures of the ankle and assessment for the presence of ligament laxity, swelling, hemorrhaging and tenderness. Ankle ROM and strength were also checked manually, in comparison to the uninjured ankle. During screening procedure, the investigators were unaware of the group the next participant would be allocated to and hence, concealed allocation was achieved. Of the 34 initially invited individuals with ankle sprains, 12 individuals were not eligible to participate. The rest 22 participants received written information sheets and verbal explanations for the study. Afterwards, they signed a consent form. Anthropometric and demographic data and sports activity level were also collected for each participant.
Two intervention groups, balance and PNF, were included. Group allocation was random and it was performed by an independent statistician, blinded to the study’s objectives, with a computer program (R software 3.1.2, blockrand package). Stratified randomization was utilized, ensuring that balance and PNF groups were balanced for gender, history of sprain to the injured ankle and sports activity level. High level was considered as participation in sports for more than 3 hours per week [22]. After commencement of the study, two participants discontinued training, and 20 participants completed the intervention. An articulation of participant flow is shown in Fig. 1.
Study flowchart.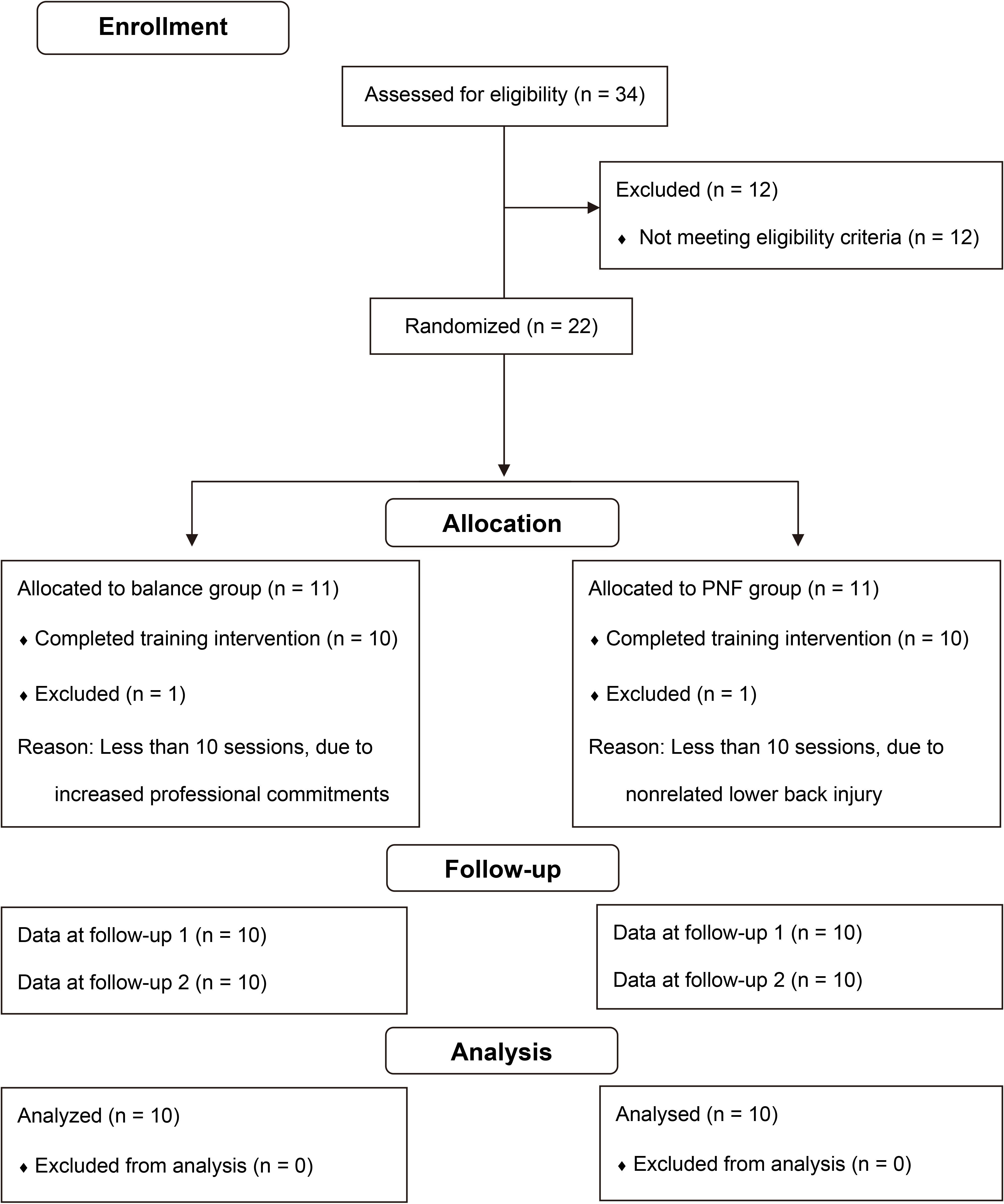
Assessment was performed in a private research laboratory by a blinded investigator, who is a physical therapist with more than 10 years experience in the assessment and treatment of ankle sprains. The blinded investigator was unaware to participants’ group allocation. In order to decrease the effects of fatigue on testing procedures, functional performance was assessed last. Each session lasted approximately one hour. Measures were recorded at baseline, at the end of training (follow-up 1) and eight weeks after training (follow-up 2).
Pain
The Greek version of the short form of the McGill Pain Questionnaire (GR-SFMPQ) was used to assess pain experience. Specifically, participants rated: i) pain sensation, on a 4-point scale, for 15 descriptive adjectives – the Pain Rating Index (PRI), ii) average pain intensity during the week before testing, on a visual analogue scale (VAS) and iii) present pain, on a 5-point verbal scale, the Present Pain Index (PPI). The GR-SFMPQ fulfills the criteria of reliability and sensitivity to pain fluctuations [23].
Dorsiflexion range of motion
Measurements of the sprained ankle were taken with a goniometer (Baseline; Irvington, NY). During testing, participants were in long sitting, on examination table, with the ankle and foot suspended over the end of the table and the subtalar joint in neutral position. Participants were instructed to actively dorsiflex the ankle, as far as comfortable, without pain. The axis of the goniometer was placed just distal to the lateral malleolus, the stationary arm was aligned with the head of fibula and the movable arm was aligned parallel to the plantar aspect of the calcaneus and fifth metatarsal [11]. Measurements were recorded in degrees, and the mean score of three measurements was computed. This testing method has shown intra-rater reliability measures greater than 0.90 [24].
Balance performance
A moveable tilting platform, the Biodex Stability System (BSS; Shirley, NY), was used to record in degrees the Stability Index (SI), which was the dependent variable and corresponded to the variance of the foot platform displacement. The SI was measured in single-leg stance, for the sprained ankle, for motions: in the saggital plane (anterior-posterior SI), the frontal plane (medial-lateral SI), and overall (overall SI). Low SI scores indicated increased stability and high SI scores decreased stability. An adaptation 15 sec trial was initially performed. Three trials of 20 sec followed, with open eyes, at medium (4 out of 8) stability level, without footwear [25], and the mean score was used for the analysis. During testing, the opposite leg was flexed off the platform, and the arms were at the side (Fig. 2). Between trials, 2 min resting was included [17]. For BSS balance measurements, intratester reliability has demonstrated intra-class correlation coefficients (ICCs) between 0.82 and 0.43 for the SI [26].
Balance performance testing.
Two tests, rising on heel and rising on toes were used to assess endurance of the ankle dorsiflexor and plantar flexor muscles, respectively. For the rising on heel test, participants were instructed to rise, as many times as possible, on the heel of the sprained leg. A pace of 60 beats per min was maintained by a metronome. During testing, which was performed without footwear, the opposite knee was approximately at 90
Rising on heel and rising on toes tests.
Ankle functional stability was assessed with two tests: single-leg hop for distance and single-leg hops for time, with footwear on. For the distance test, participants were instructed to hop, using the sprained leg, as far forward as possible, with free arms, and remain in the landing position for 2 sec (Fig. 4). The hopping distance was then measured. For the time test, participants covered as fast as possible a six-meter distance, with the sprained leg, using single-leg hops, and the trial was timed (Fig. 5). For the distance and time tests, all participants performed three maximal attempts with complete stabilization after landing, and no faults trials were recorded. For each test, the mean score of three trials was calculated. Participants rested for 30 sec between trials and 45 sec between tests. For the distance test, intra-class correlation coefficients range from 0.84 to 0.99, and or the time test they are between 0.66 and 0.77 [28]. Prior to functional performance testing, participants warmed up for 5 min.
Single-leg hop for distance test.
Single-leg hops for time test.
Balance training protocol
All participants received 10 training sessions, supervised by the same physical therapist, at a private rehabilitation center, within a six-week period. The duration of each session was 50 to 60 min. Participants were instructed to discontinue a session in cases of significant pain or fatigue. For the balance group, the designed protocol reflects clinical guidelines for the rehabilitation of sprains [29]. The balance training protocol is presented in Table 1. Balance activities were performed without footwear, apart from the hopping activities. Rest periods of 60 sec and 2 min were provided after each exercise and between different training types, respectively.
For the PNF group, two different techniques, rhythmic stabilization (RS) and combination of isotonics (COI) [20] were applied to the sprained leg of participants, who were positioned in supine, on a physical therapy table, facing the therapist. Each PNF technique was applied for both lower extremity diagonals, at the end of the upper and lower diagonal’s range, with the knee in extension. During application, timing for emphasis was implemented for the ankle and foot, and the therapist resisted against the occurrence of hip and knee motions. The therapist’s hands were placed according to PNF principles, depending on the technique and diagonal pattern under application. Maximal resistance was provided, in conformity with each individual’s needs.
The RS protocol comprised alternating isometric contractions for 10 sec, with no intended motion [20]. The COI protocol included combined concentric, stabilizing and eccentric contractions of the agonistic muscles, without relaxation, for 15 sec; the duration of each contraction was 5 sec [20]. Training consisted of 5 to 15 repetitions per set, depending on the exercise tolerance of each individual [29]. Between the sets, 30 sec rest was included [20]. The RS protocol was performed first and the COI protocol followed, after 2 min rest. Each protocol lasted approximately 20 min, including rest intervals. Prior to the application of each protocol, instructions were provided regarding the correct performance of the pattern and maximal effort was required for all repetitions. At the end of each session, for both groups, training included forward and backward walking on toes and heels for 4 min, with 60 sec of in-between rest. During the study, participants were instructed to refrain from any form of additional supervised training.
Statistical analysis
The non-parametric Friedman test was used to determine the within-group differences for all outcome variables across time points, with a two-tailed significance level of
Characteristics of participants in the balance and PNF groups
Characteristics of participants in the balance and PNF groups
Balance group scores and Friedman test results for each outcome measure
At baseline, follow-up 1 and follow-up 2, means (SD) are reported, except to the PPI, rising on heel, rising on toes and total rises ordinal data for which median scores (minimum, maximum) are reported;
PNF group scores and Friedman test results for each outcome measure
At baseline, follow-up 1 and follow-up 2, means (SD) are reported, except to the PPI, rising on heel, rising on toes and total rises ordinal data for which median scores (minimum, maximum) are reported;
Participants’ characteristics are displayed in Table 2; these were similar for the balance and PNF groups. At baseline, no significant (
Table 3 shows significant (
For the PNF group, Table 4 shows significant (
For the functional performance measures of the PNF group, post-hoc analysis showed that significant (
In terms of the between-group differences, most comparisons against baseline lacked significance (
Discussion
The main finding of this study is that for individuals with ankle sprain both balance and PNF groups significantly improved dorsiflexion ROM and most measures of functional performance eight weeks after training. Eight weeks after training, solely the balance group significantly improved performance in frontal plane balance test and reported significant reduction in pain. For all significant improvements, the effect sizes were large, indicating clinical significance.
In our study, participants exhibited limited dorsiflexion ROM at baseline. As shown in Tables 3 and 4, dorsiflexion means for the balance and PNF groups were 8 and 7 degrees. After training, normal dorsiflexion ROM means were recorded, for both groups (Balance: 15 degrees; PNF: 13 to 15 degrees). The signifi- cant ROM gains, observed in our results, could be attributed to the specific proprioceptive training protocols utilized. In particular, the balance program included wobble board activities. As the deflection angle of the board utilized is 22 degrees (Thera-Band; Akron, Ohio), backward board’s tilts should have produced dynamic stretching of the ankle plantar flexor muscles, and hence dorsiflexion ROM was improved for the balance group. Moreover, PNF techniques were applied against resistance at maximal, non-painful ROM. It is suggested that PNF techniques are able to activate body’s inhibitory reflexes to induce relaxation of muscles [18]. Muscle relaxation has probably promoted increased stretch magnitudes during application in our study, resulting in the ROM gains observed. To our knowledge, this is the first study investigating the effects of proprioceptive training on ROM following ankle sprain.
In our findings, most functional performance measures significantly improved eight weeks after training for both balance and PNF groups (Tables 3 and 4). For individuals with ankle sprain, significant functional improvement has also been found following participation in 10 sessions of balance and strength training, stretching and running activities [13]. These findings support our results; in opposition to our study however, balance training was solely one component of the rehabilitation protocol [13]. The effects of PNF training have been investigated in individuals with chronic ankle instability, and no significant functional gains were demonstrated, compared to no exercise [19]. In our study, we found functional gains, which could be attributed to the fact that the applied PNF program focused on entire lower extremity, and not just the ankle, as occurred in the chronic instability study [19]. It seems that PNF training incorporating knee and hip neuromuscular control strategies is required in order to achieve significant functional improvement. In our study, measures in heel rises and distance hop tests were significantly improved eight weeks after training solely for the balance group. This may be justified by the specificity of the balance protocol, which included heel rising activities on wobble board and firm surfaces and distance hop tasks in various directions (Table 1).
In our study, ten 50–60 min sessions of proprioceptive training produced no significant changes in most measures of balance performance, for both groups (Tables 3 and 4). For the balance group, nevertheless, significant improvement was observed in the frontal plane balance test, eight weeks after training. In relation to these results, negative findings on balance performance have been demonstrated in individuals with acute sprain, four months post-injury, following participation in balance training and running activities [15]. In opposition to our protocol, however, the effects of training were assessed in comparison to the uninjured side, and baseline measurements were not performed owing to the acute phase of the sprain [15]. Furthermore, 18 sessions of strength and balance training (duration: 10 min per session) caused significant gains on dynamic balance measures in three individuals under 18 years of age, with post-acute ankle sprain [14]. Direct comparisons with our findings may be attempted with caution, due to differences in the type and duration training and participants’ age.
Balance performance in our study was assessed in single-leg stance on a tilting platform of medium stability. The applied proprioceptive training programs, however, included a small number of weight-bearing exercises using solely the injured leg, and this was the case for the balance program. This is a possible reason for the significant recordings in the frontal plane balance test, found eight weeks after training for the balance group. On the contrary, application of PNF exercises in non-weight bearing positions under static conditions may have resulted in the non significant findings observed for the PNF group. Our findings suggest that balance protocols may be beneficial after sprains for improving measures of balance performance on unstable surfaces; however, these balance protocols should contain a considerable number of dynamic exercises in sprained-leg stance. The PNF protocols are not recommended for improving balance performance in ankle sprains.
In our study, solely the balance group reported significant reduction in pain eight weeks after training for all GR-SFMPQ components (Tables 3 and 4). For ankle sprains, effectiveness on pain has been investigated for rehabilitation programs that comprised wobble board training, mobilization techniques, cryotherapy [16, 17] and strengthening exercises [17]. Findings showed significant reduction in pain following rehabilitation; nevertheless, similar pain reduction was also found following bandage support [16, 17] and immobilization [16], indicating that pain relief may have resulted from natural sprain’s recovery. In opposition to these multi-component rehabilitation programs, which were initiated at the acute phase of the injury, we applied post-acute (2.6 to 3.0 months after sprain; Table 2) balance or PNF training to all participants. For individuals with ankle sprain, our findings indicate that the combined application of RS and COI techniques is not effective in reducing pain eight weeks after training; hence this is not recommended in clinical practice for pain relief. This is the first study investigating the effects of proprioceptive training on pain as a single approach, and not as one component of a rehabilitation program. Further studies are required to confirm our findings.
Limitations of this study include the relatively small sample size (
Conclusion
This study shows that both balance and PNF programs resulted in clinically significant improvements in dorsiflexion ROM and most functional performance measures in individuals with ankle sprain, eight weeks after training. The balance program also caused clinically significant improvements in frontal plane balance test and pain, eight weeks after training. The PNF program was not capable of improving balance performance and pain, eight weeks after training. For future studies, long-term effectiveness of balance and PNF training programs in ankle sprains is worth investigating.
Footnotes
Conflict of interest
None to report.