
Abstract
BACKGROUND:
During pregnancy, many pregnant women experience lumbopelvic pain due to mechanical, systemic, and hormonal reasons and this pain and fear of movement (kinesiophobia) causes daily life limitations.
OBJECTIVE:
To examine low back pain (LBP), kinesiophobia, disability, and related conditions that develop together during pregnancy.
METHODS:
The was a cross-sectional and analytical study. The presence, severity, and duration of pain in the lumbopelvic region were questioned. Postpartum LBP was evaluated using a self-administered questionnaire, disability using the Oswestry Disability Index (ODI), pain intensity using a visual analog scale (VAS), physical activity levels using the physical activity level during pregnancy questionnaire and the international physical activity questionnaire short form, and kinesiophobia was evaluated using the Tampa Scale for Kinesiophobia.
RESULTS:
The study comprised 120 pregnant women with a mean age of 27.4
CONCLUSION:
LBP in pregnant women has a higher frequency than in the normal population, regardless of age, gestational week, and gravida. Obesity appears to be a risk factor for LBP and increases disability. Kinesiophobia in pregnant women is significantly associated with obesity and disability. Unless there are contraindications, a physically active pregnancy process and regular exercise should be recommend.
Introduction
Nearly half of all pregnant women experience low back pain (LBP) during or after pregnancy. Most women recover from pregnancy-related LBP within 3 months of delivery; however, postpartum follow-up studies have shown that approximately 8–20% of pregnant women still have persistent non-specific LBP. Mechanical and hormonal changes lie in the etiology of LBP [1].
Physical activity is defined as any body movement created by skeletal muscles that causes energy expenditure [2]. Physical activity can be classified in several ways: sleep, work, and leisure activities. Leisure time activities include sports and exercise activities, household (such as gardening, cleaning, or house repair), and other activities [3]. Exercise, which is often confused with physical activity, is expressed as planned, individually structured, and repetitive body movements aimed at improving physical fitness [4].
Pregnancy is associated with important physiologic and psychological changes in a woman’s life that can lead to a sedentary and low level of physical activity. Adopting a sedentary lifestyle during pregnancy poses a long-term risk for the development of maternal and fetal obesity, the risk of gestational diabetes, pregnancy-induced hypertension, and cardiovascular disease [5]. To prevent these complications, health professionals should motivate pregnant women to be physically active and exercise.
Kinesiophobia is the fear that develops due to the belief of susceptibility to injury. It is associated with lower levels of physical activity due to susceptibility to injury. Kinesiophobia should be continually evaluated in clinical settings. According to the available data, it has been observed that kinesiophobia is affected by a small number of chronic musculoskeletal diseases (e.g., LBP, osteoarthritis, and osteoporosis) [6].
Decreased activity levels in pregnant women can lead to disability, which is closely related to fear of movement (kinesiophobia) in patients with chronic LBP. In some clinical practices, women with pelvic pain are taught to avoid activities that increase pain. This situation may lead to fear of movement and avoidance behavior that goes beyond normal, namely kinesiophobia, and may cause chronic pelvic pain associated with pregnancy despite termination of pregnancy. Due to this pain and kinesiophobia, pregnant women experience limitations in their daily lives. In our study, we aimed to evaluate LBP, disability, and physical activity levels together with kinesiophobia in pregnant women during pregnancy. These closely related clinical conditions will affect the individual’s comfort and quality of life both during pregnancy and in the post-pregnancy period.
Materials and methods
Sample selection
The research was planned as a cross-sectional and analytical study. Simple random sampling was perfomed. The study population was determined at the gynecology and obstetrics outpatient clinic. The inclusion criteria were as follows: Being aged 20–40 years, having pain in the lumbopelvic area, having no history of LBP before pregnancy, and having no orthopedic or systemic problems that might cause LBP.
The presence of lumbopelvic pain was investigated using a questionnaire. Sociodemographic (age) and pregnancy-related data (gravida, gestational week, trimester, menstruation date) of the patients were recorded. Body mass index (BMI) was recorded. The presence, severity, and duration of LBP were questioned and evaluated using self-administered questionnaires or interviews. Disability was evaluated using the Oswestry Disability Index (ODI) [7], LBP intensity was evaluated using a visual analog scale (VAS, 0–10 cm), and physical activity levels were evaluated using the physical activity level during pregnancy questionnaire [9, 10] and the international physical activity questionnaire short form [11, 12]. Kinesiophobia was evaluated using the Tampa Scale for Kinesiophobia [13].
To exclude osteodegenerative changes, the exclusion criteria were as follows: A history of LBP before pregnancy, a history of spinal/orthopedic abnormality or surgery, multiple pregnancy, chronic systemic diseases (spondyloarthropathies, diabetes mellitus, hypertension, thyroid disease), and age
Oswestry disability index (ODI)
The ODI has become one of the principal condition-specific outcome measures used in the management of spinal disorders. It consists of 10 questions with a total of six options. The points given for each question answered were: A
Pregnancy physical activity questionnaire (PPAQ)
PPAQ was developed in 2004 and has since been widely used in the evaluation of physical activity in pregnant women. The questionnaire includes activities that are important determinants of physical activity in pregnant women and measures the duration, frequency, and intensity of physical activity in pregnant women [9]. PPAQ is a semi-quantitative survey and it determines how much time pregnant women spend on activities such as household/caregiving activities (13 activities), professional activities (five activities), sports/exercise (eight activities), transportation (three activities), and inactivity (three activities). Tosun et al. [10] found that the Turkish version of this questionnaire was valid and reliable in evaluating the physical activity levels of pregnant women. Activities are classified according to their type (household/caregiving activities, occupational activities, and sports/exercise).
International physical activity questionnaire-short form (IPAQ-SF)
IPAQ-SF was developed by the International Consensus group in Geneva in 1998 to assess the physical activity levels of individuals at an international standard. Then, in 2000, it was accepted as a valid and reliable scale in 12 different countries [11]. Sağlam et al. [12] showed that the short and long forms were valid and reliable in Turkish. With this questionnaire, the physical activity levels of individuals in the last 7 days are evaluated under 4 headings (vigorous activities, moderate activities, walking, and sitting). According to these scores, individuals are divided into three groups “inactive,” “minimally active,” and “very active” (physical activity that increases health).
Tampa scale for kinesiophobia (TSK)
The TSK is a 17-item questionnaire used to assess the subjective rating of kinesiophobia or fear of movement. The original questionnaire was developed to discriminate between non-excessive fear and phobia among patients with chronic musculoskeletal pain. Several studies have found the scale to be a valid and reliable psychometric measure. As the score increases, the severity of kinesophobia increases. Most authors agree that a value of
Statistical analysis
Statistical Package for the Social Sciences (SPSS) version 20.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical data are shown as percentages and frequencies and compared using the Chi-square test. Numerical data are shown as ratio, mean standard deviation, and median (minimum/maximum). As a result of the power analysis, considering the type 1 error as 0.05 and the power of the test as 0.80, the minimum sample size was calculated as 86. Effect size (ES) can be expressed as the expected difference between two means or two ratios according to the outcome variable of interest to reveal a clinically meaningful difference. This is an indicator of the practical relevance of the research results. It is calculated by taking the ratio of the difference between the means to the standard deviation before treatment. The ES was interpreted as defined by Cohen: 0.50 is a large effect.
The normality of data distribution was evaluated using the Kolmogorov-Smirnov test and histogram analysis. For each parameter, a comparison was performed between the two groups according to the presence of LBP. The independent samples Student
Sociodemographic, obstetric, and clinic data of the grou
Sociodemographic, obstetric, and clinic data of the grou
Abbreviations: BMI: body mass index, VAS: visual analog scale, LBP: low back pain.
A total of 120 pregnant women with a mean age of 27.4
Boxplot of Oswestry score according to LBP.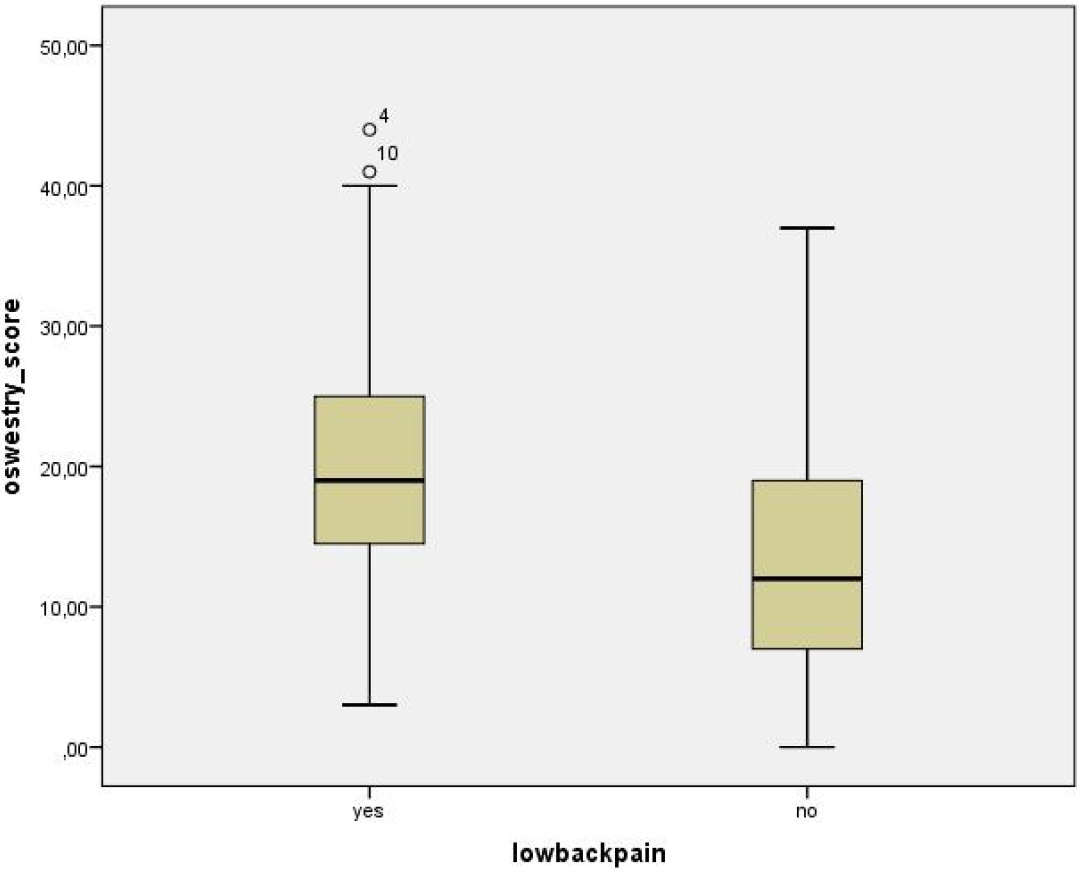
The comparison of two groups according to the presence of low back pain
Abbreviations: BMI: body mass index, VAS: visual analog scale. Independent samples Student
When we divided the group according to LBP, the age (
Boxplot of body mass index according to severe kinesiophobia.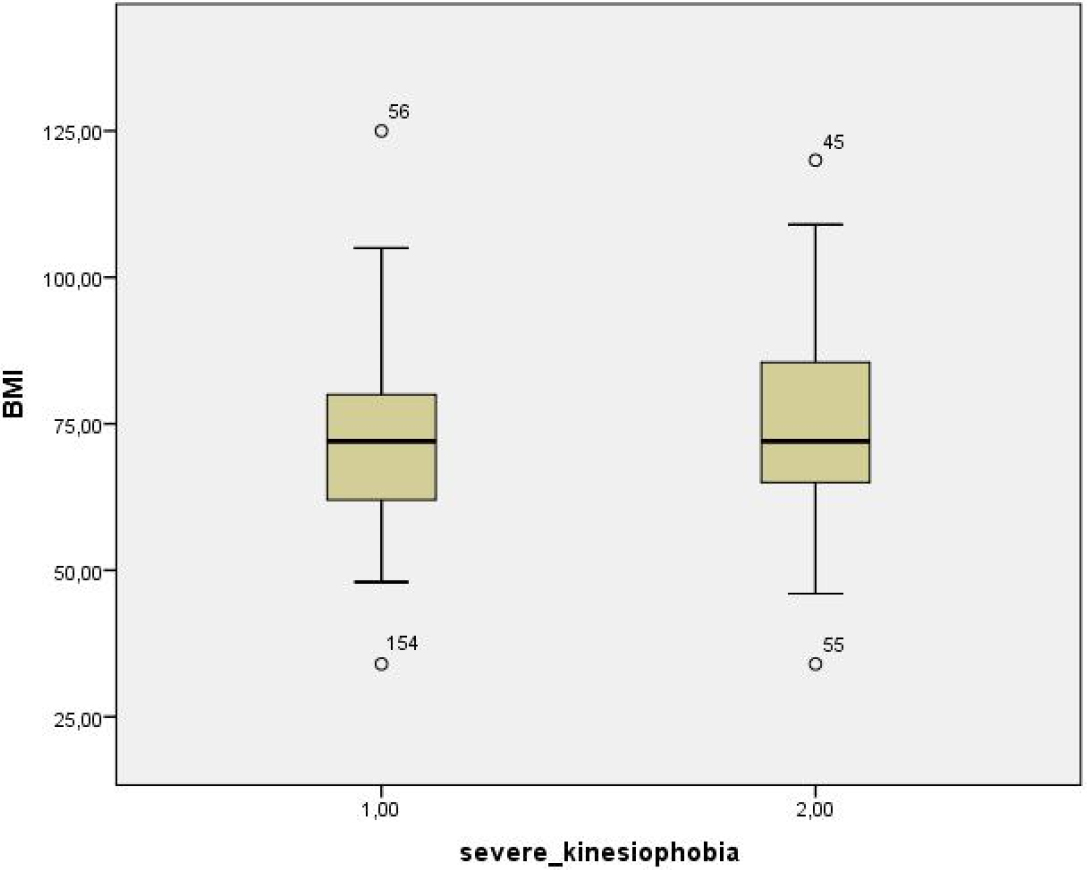
In correlation analysis, the ODI score was positively correlated with Tampa score (
More than two-thirds of pregnant women have LBP and almost one-fifth report pelvic pain. In our study, this rate was 42.3%. It usually develops after the 6th month and may continue until the postpartum 6th month. Our study group mostly consisted of young age, last-trimester, and physically inactive pregnant women. Most of the women in the study had moderate disability. Several biomechanical, hormonal (relaxin), and psychologic changes during pregnancy are held responsible for LBP [15]. These two conditions can develop together or separately and typically increase with the progression of pregnancy and change with work, daily activities, and sleep. In a meta-analysis, a low level of evidence was observed that exercise reduced pregnancy-related LBP and a moderate-low level of evidence that it reduced functional disability [16]. It has been observed that exercise reduces pain and disability related to lumbopelvic pain with a low level of evidence [17]. In our study, pain intensity and disability scores were positively correlated. Increasing the severity of LBP increases the individual’s disability due to physical activity limitations. Although the effects are small, pregnancy-specific exercises and physiotherapy seem to be effective in reducing low back or pelvic pain compared with prenatal care alone [18].
In our study, BMI was higher in our pregnant group with LBP. In addition, disability scores were positively correlated with BMI. LBP symptoms are higher in overweight pregnant women. LBP and obesity are both rising epidemics. This situation can be explained by more than one mechanism. Obesity contributes to poor lumbar perfusion and spinal structural abnormalities. The adipose tissue of patients with obesity secretes some types of cytokines, pro- and anti-inflammatory, which have some systemic effects [19].
In addition, the disability score was higher in the pregnant group with LBP. From this point of view, we can say that LBP increases disability in pregnant women. Encouraging women to solve their LBP before they become pregnant is important in preventing pain. Regular moderate physical activity by pregnant women reduces the risk of obesity and overweight. Regular physical activity helps maintain normal mental and physical well-being. Lack of physical activity is observed in pregnant women due to reasons such as fatigue, time constraints, and pregnancy disorders. In our study, we found that the disability scores of pregnant women negatively correlated with high sports and exercise activity scores. This supports the positive effect of physical activity in pregnant women against disability [20].
Pregnant women mostly did household and caregiving activities in the study. Regular physical activity has been proven to provide many benefits for the mother and fetus. Improvement of cardiovascular function, prevention of excess weight gain, reduction of discomfort in the musculoskeletal system, reduction in muscle cramps and lower extremity edema, psychological well-being, and prevention of gestational diabetes and gestational hypertension can be listed as maternal benefits [21]. Traditionally, pregnant women were advised to reduce their physical activity levels. Studies have shown that physical activity has no negative consequences on the mother or the fetus or an increase in complications such as abnormal fetal growth [22, 23]. Physical activity is a determinant of quality of life in pregnant women. The development of physical activity programs for pregnant women should be supported in prenatal care [24, 25, 26]. In their meta-analysis, Rodríguez-Martínez et al. [27] recommended a moderate-intensity exercise program for pregnant women, including aerobic, resistance, and strengthening exercises, three times per week. The World Health Organization recommends pregnant women perform at least 150 minutes of moderate-intensity aerobic physical activity per week unless there is a contraindication.
Kinesiophobia is defined as the fear of movement or re-injury. In our correlation analysis, we found that disability scores were positively correlated with pain intensity and kinesiophobia scores. Accordingly, we can say that the severity of LBP and fear of movement increase physical disability in pregnant women. In a systematic review investigating the effects of kinesiophobia on pain, disability, and quality of life, there was strong evidence that kinesiophobia was associated with higher pain levels and lower quality of life. High kinesiophobia becomes a determinant of the development of disability over time with a moderate level of evidence [28].
Kinesiophobia should be reviewed in all pregnant women with pain symptoms, pregnant women with severe kinesiophobia should be motivated to be physically active, and LBP treatment should be performed if kinesiophobia is caused by lumbopelvic LBP.
In people with chronic musculoskeletal pain, kinesiophobia is a determinant of pain, proprioception, and functional performance [29, 30]. Pain avoidance behavior is important for disability and affects treatment success [31]. Only a few articles in the literature have investigated kinesiophobia in pregnant women. In the study conducted by Ebina et al., high kinesiophobia was observed in the depressive group and kinesiophobia was found to be an independent predictor for late pregnancy and postpartum depression [32]. In the study of Gutke et al., quality of life-related disability and kinesiophobia were found to be a minor determinant, and pain intensity was found to be a major determinant for lumbopelvic pain [33]. Fernando et al. found that pregnant women who developed high fear-avoidance behavior in the last trimester developed lumbopelvic pain with a high frequency until the postpartum 6th month [34]. We showed that kinesiophobia was associated with both LBP and high BMI, causing physical disability in pregnant women.
Many factors affect LBP in pregnant women, and it seems that these factors also increase kinesiophobia and disability, one of which is obesity. It is not possible to clearly distinguish these situations that mutually affect each other. For example, someone who is overweight during pregnancy will have a physically inactive pregnancy, and the opposite is also true. Someone who is physically inactive during pregnancy will be overweight. Both conditions are closely related to disability and kinesiophobia.
The limitations of our study are the sample size, compiling the results of literate pregnant women from only one center, and the lack of follow-up information about LBP in the post-pregnancy period.
Conclusion
LBP in pregnant women has a higher frequency than in the normal population, regardless of age, gestational week, and gravida. Obesity appears to be a risk factor for LBP and increases disability. Kinesiophobia in pregnant women is significantly associated with obesity and disability. A sedentary lifestyle can have negative effects on the health of both mother and baby; therefore, unless there is a contraindication for pregnant women, we should recommend a physically active pregnancy process and regular exercise.
Author contributions
Idea, writing, design, sources, analysis and/or interpretation, literature review, supervision, critical review: T.T.K.; data collection and/or processing: A.Ö.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
The study was approved by the Regional Committee for Ethics in Medical Research of Kahramanmaraş Sütçü İmam University Date: 24.01.2023; Protocol no: 07) and was performed in accordance with the principles of the Declaration of Helsinki.
Funding
None to report.
Informed consent
An informed consent form was obtained from all participants.
Footnotes
Conflict of interest
The authors declare no conflicts of interest with respect to the authorship and/or publication of this article.