
Abstract
BACKGROUND:
Osteosarcomas are a rare, heterogeneous and malignant group of bone tumors that have a high potential for metastasis and aggressive growth patterns. Treatment of metastasized osteosarcoma is often insufficient and research is compromised by problems encountered when culturing cells or analyzing genetic alterations due to the high level of intratumoral and intertumoral heterogeneity. The chick chorioallantoic membrane (CAM) model, a 3D-in-vivo-tumor-model, could potentially facilitate the investigation of osteosarcoma heterogeneity at an individual and highly specified level.
OBJECTIVE:
Objective was to establish the grafting and transplantation of different primary osteosarcoma tissue parts onto several consecutive CAMs for tumor profiling and investigation of osteosarcoma heterogeneity.
METHODS:
Various parts of primary osteosarcoma tissue were grafted onto CAMs and were transplanted onto another CAM for five to seven consecutive times, enabling further experimental analyzes.
RESULTS:
Primary osteosarcoma tissue parts exhibited satisfactory growth patterns and displayed angiogenic development on the CAM. It was possible to graft and transplant different tumor parts several times while the tissue viability was still high and tumor profiling was performed.
CONCLUSIONS:
Primary osteosarcoma tissue grew on several different CAMs for an extended time period and neovascularization of serial transplanted tumor parts was observed, improving the versatility of the 3D-in-vivo-tumor-model.
Introduction
Sarcomas are a highly heterogeneous group of rare, malignant neoplasms of mesenchymal cells that are characterized by aggressive growth patterns and early metastasis [1]. Sarcomas are classified into two main subgroups; soft tissue sarcomas and bone sarcomas. Of the two subgroups, bone sarcomas make up for approximately 10% of all sarcomas [2]. Furthermore, osteosarcomas are the most common primary bone tumors of children, adolescents and young adults but still only account for approximately 5% of all childhood malignancies [3, 4]. Osteosarcomas arise mostly in the metaphysis of the proximal tibia or distal femur, are highly vascularized and a primary metastasis site is the lung [5, 6]. This contributes to the fact that five-year event free survival (EFS) of high-grade osteosarcomas is only as low as 54% despite the introduction of polychemotherapy as well as many technical advances in surgery in the last decades [7]. The etiology is unknown in most cases but the localization in the metaphysis is presumably due to the vast cleavage in the epiphyseal cartilage. A higher incidence is also linked with Li-Fraumeni Syndrome, hereditary retinoblastoma and Paget’s disease of the bone in older patients [8, 9]. Furthermore, modern surgical techniques have made limb salvage after resection of the tumor possible and resection with negative margins has been improved by neoadjuvant therapy and minimizes the risk of local relapse [10, 11]. However, despite multidisciplinary treatment approaches consisting of radiotherapy, surgery, oncology and pediatrics among others, outcomes still remain unsatisfactory and further investigation is necessary [8].
The chick chorioallantoic membrane (CAM) model has already been utilized in a variety of different oncological research applications involving the grafting of tumor cells or tumor tissue, metastasis, chemosensitivity and tumor angiogenesis [12–17]. The CAM is an extraembryonic, highly vascularized and non-innervated membrane that is formed during embryogenesis of the chick embryo [18, 19]. Furthermore, Sys et al. mentioned the CAM model particularly for the grafting of sarcoma cells which are otherwise difficult to culture in vitro [20] and Kunz et al. established the CAM model as a reliable method for the grafting of osteosarcoma cells derived from cell culture [21]. To our knowledge, the grafting of primary osteosarcoma tissue onto the CAM has not been performed until now and would resemble a big advance for the methodology of this model. It has to be mentioned that the time period for the investigation of tumor material on the CAM is limited to the time frame of the embryonic development to about eight days. It would also strongly improve the methodology if it would be possible to investigate grafted material on the CAM for a longer time period.
Aim of this study was to establish the grafting and the transplantation of primary osteosarcoma tissue parts from one CAM onto another without compromising the tissue viability and morphology while enabling continuous experimental analysis. The focus hereby was to extend and increase the level of analysis of heterogenous tissue parts that are inherent to osteosarcomas and have to be taken into account for appropriate treatment regimens.
Material and methods
Tumors on the chorioallantoic membrane (CAM) model and transplantation
The CAM model was carried out as described in previous publications [22]. Fertilized chicken eggs were incubated in a ProCon egg incubator (Grumbach, Asslar, Germany) at 37.8°C and 63% humidity under hourly rotation for a four-day period until a window of approximately 1×1 cm was cut into the eggshell and sealed again with tape. The incubation continued for another four days until the CAM was roughened with a cotton swab before primary material was grafted onto it. After an eight-day growth period the tumor was explanted and divided to enable experimental analysis such as 3D volume measurements and perfusion measurements of the tumor. The remaining part of the tumor was then transplanted onto a new CAM. The procedure was repeated five to seven times for three different sections of the osteosarcoma from one patient.
3D volume and perfusion measurements
3D volume measurements were performed before and after tumor growth with a Keyence VHX-6000 according to the manual. Perfusion measurements on the basis of LASCA technology were carried out in accordance to the established protocol (Pion et al. 2020, in revision).
Results
The biopsy of the osteosarcoma was performed on a 12-year old patient who had undergone rotationplasty surgery. The biopsy was divided into different tissue parts in order to investigate characteristics of the tissue through further experimental procedures (see procedure in Fig. 1). An extensive analysis of the tumor diversity in osteosarcomas is of particular interest because of the high level of heterogeneity of this tumor entity. Thus, each tumor part was grafted onto the CAM in order to distinguish different characteristics such as growth patterns, morphology, angiogenesis etc. of the transplanted tumor tissue. After a period of seven days, tumors that had grown on the CAM were divided into two parts, whereby one tissue part was transplanted onto a new CAM while the other tissue part could be used for further experiments, such as investigation of proteomic and genomic landscapes, as well as 3D volume measurements and perfusion measurements. Moreover, tumor morphology can be analyzed by performing immunohistochemistry and RNA can be extracted for further experiments. With this approach, tumor parts can be compared at various levels and tumor diversities can be studied.
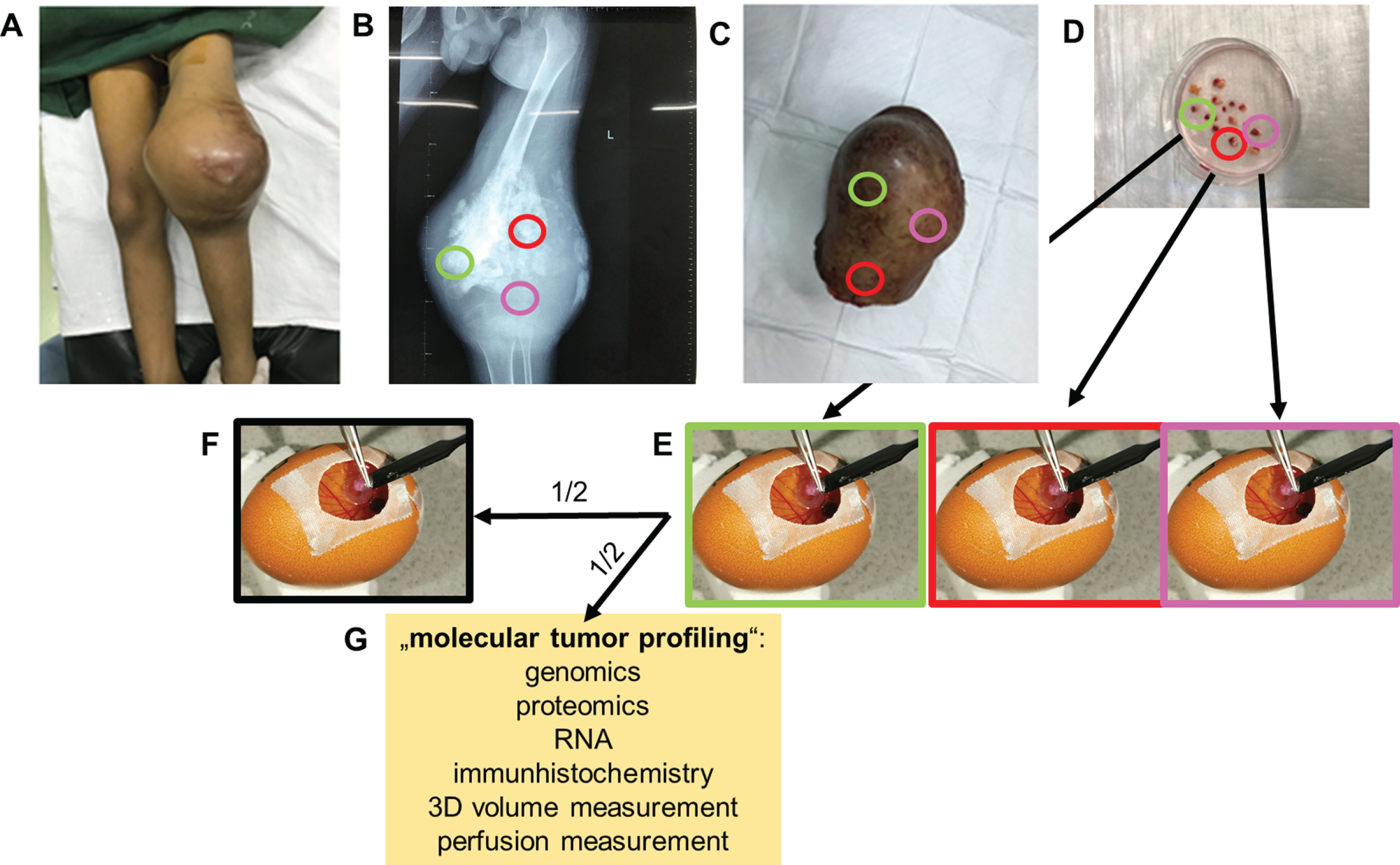
Molecular tumor profiling with the CAM model. A. Patient with an osteosarcoma of the distal femur; B. X-ray image of an osteosarcoma; three colored circles illustrate tumor heterogeneity; C. Excised osteosarcoma after rotationplasty surgery; D. Division of the osteosarcoma into various tissue parts; E. Grafting of the osteosarcoma parts onto the CAM; F. Transplantation of one tumor part onto a consecutive CAM; G. Assessment of molecular tumor profiles through further experimental procedures.
The various osteosarcoma tissue parts (see colored circles in Fig. 1) proved to be vital and exhibited satisfactory growth processes within the CAM model (see Fig. 2). Transplantation of tumors from one fertilized egg onto a consecutive egg was conducted for five to seven times, e.g. from 6th to 8th osteosarcoma generation, whereas transplanted tumor areas demonstrated an increase in tumor size, indicating tumor growth, which was already observed macroscopically. On a macroscopic level, the tumor parts showed differences, both within a generation as well as between the transplantations. These differences were clearly reflected in the color and the tissue morphology. From the 3rd to 6th generation of tumors partial necrosis of the tumor tissue occurred. Moreover, vascular response of the CAM towards the tumors was observed for each osteosarcoma section and each generation, indicating that angiogenic development took place in all osteosarcoma parts during the growth period on the CAM. Angiogenesis displayed in each generation could be studied by performing perfusion measurements using Laser speckle contrast analysis (LASCA) technology (see Fig. 3).
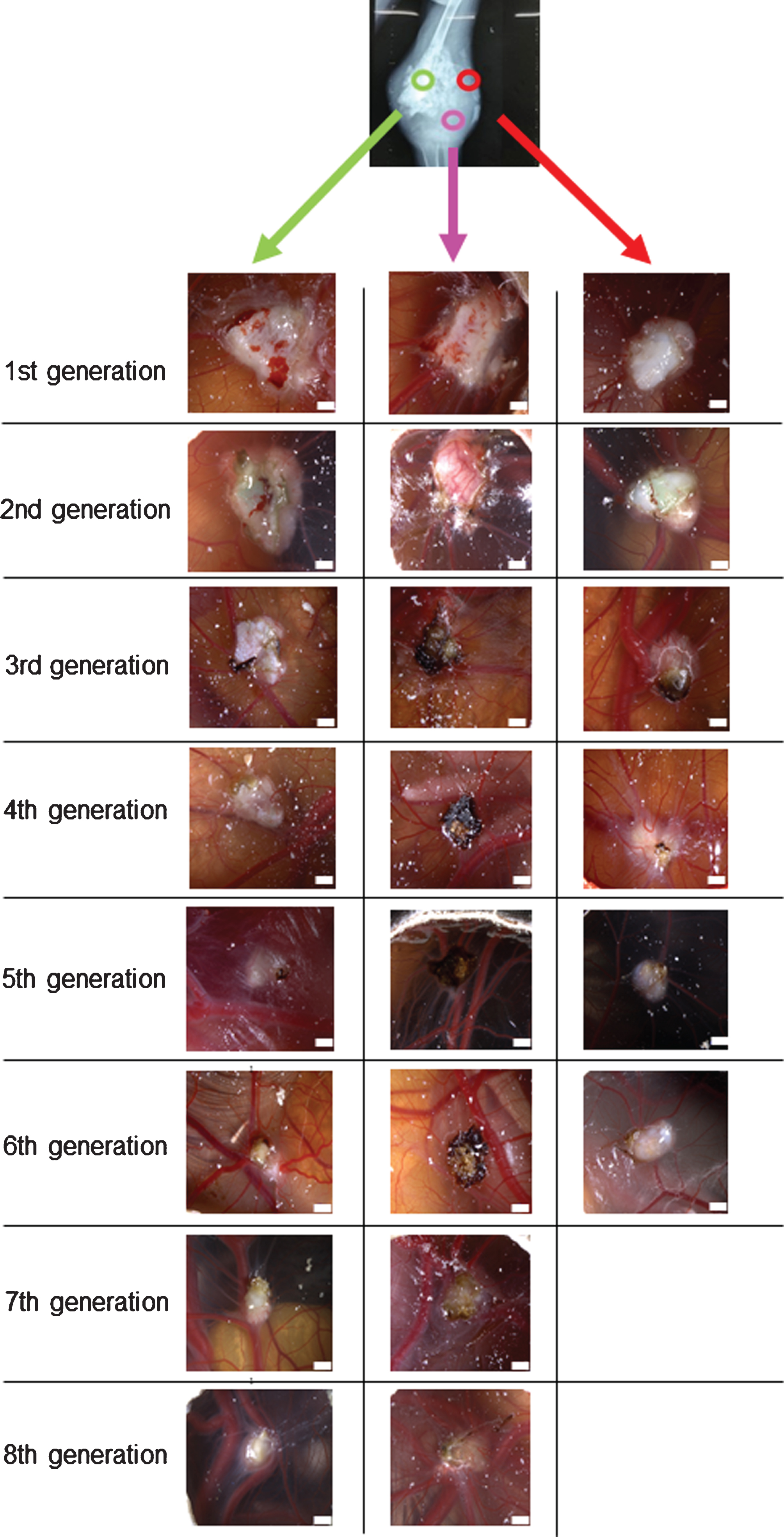
Transplantation of various osteosarcoma parts onto the CAM. Various osteosarcoma parts were transplanted up to seven times from one CAM to another. The osteosarcoma sections demonstrated different growth patterns, macroscopic structure and neovascularization. Scale bar = 1000°μm.
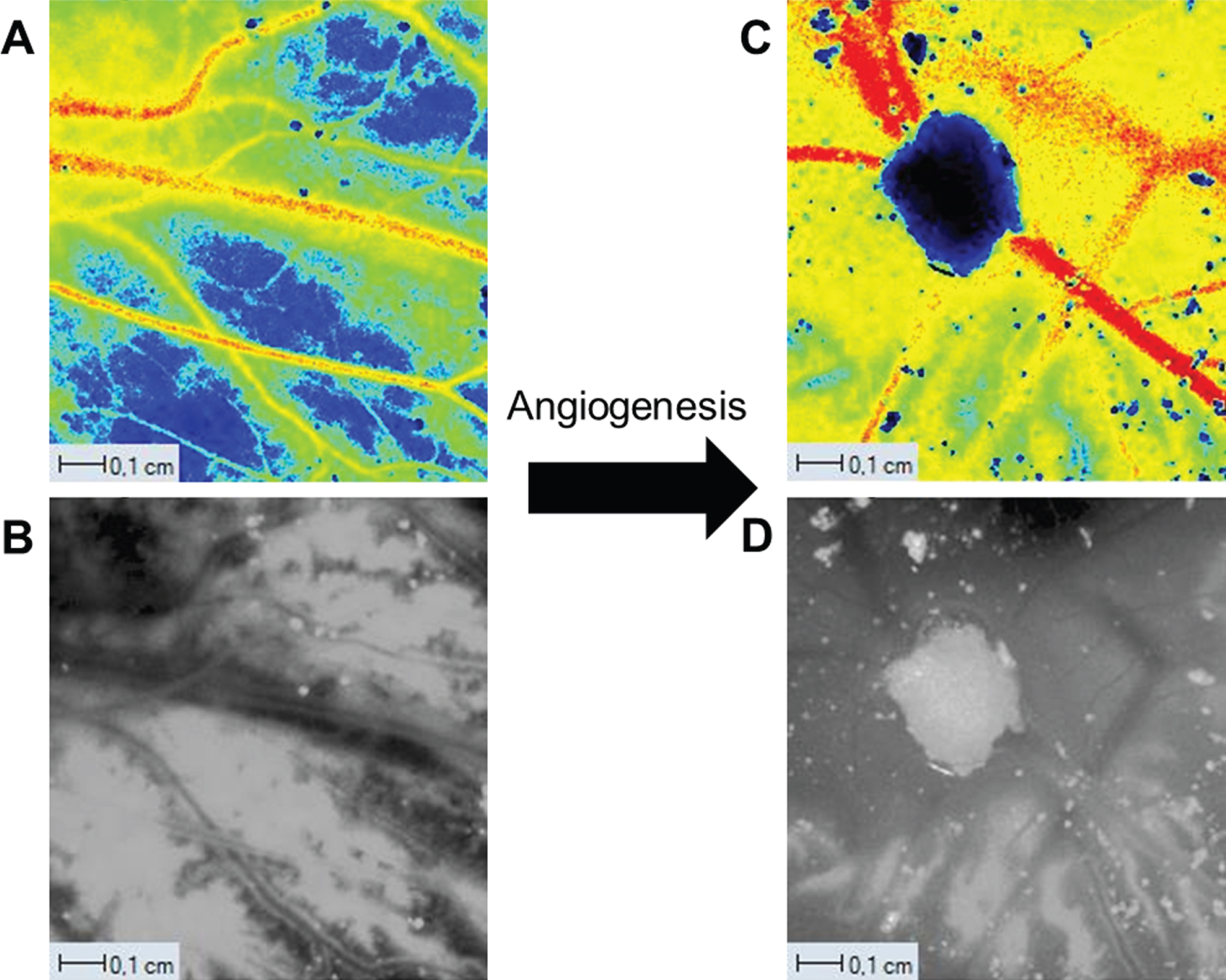
Perfusion measurements. A. Perfusion image of the CAM; B. Monochrome intensity image of the CAM without osteosarcoma; C. Perfusion image of the CAM with an osteosarcoma; D. Monochrome intensity image of the CAM with an osteosarcoma.
Excision of tumor material was performed for further experimental procedures (see Fig. 4). After the excision of the tumor, subsequent volume measurements were performed (see Fig. 5) prior to the division of the tumor into two parts of which one was transplanted onto a newly incubated CAM model and the other was utilized for further molecular tumor profiling.
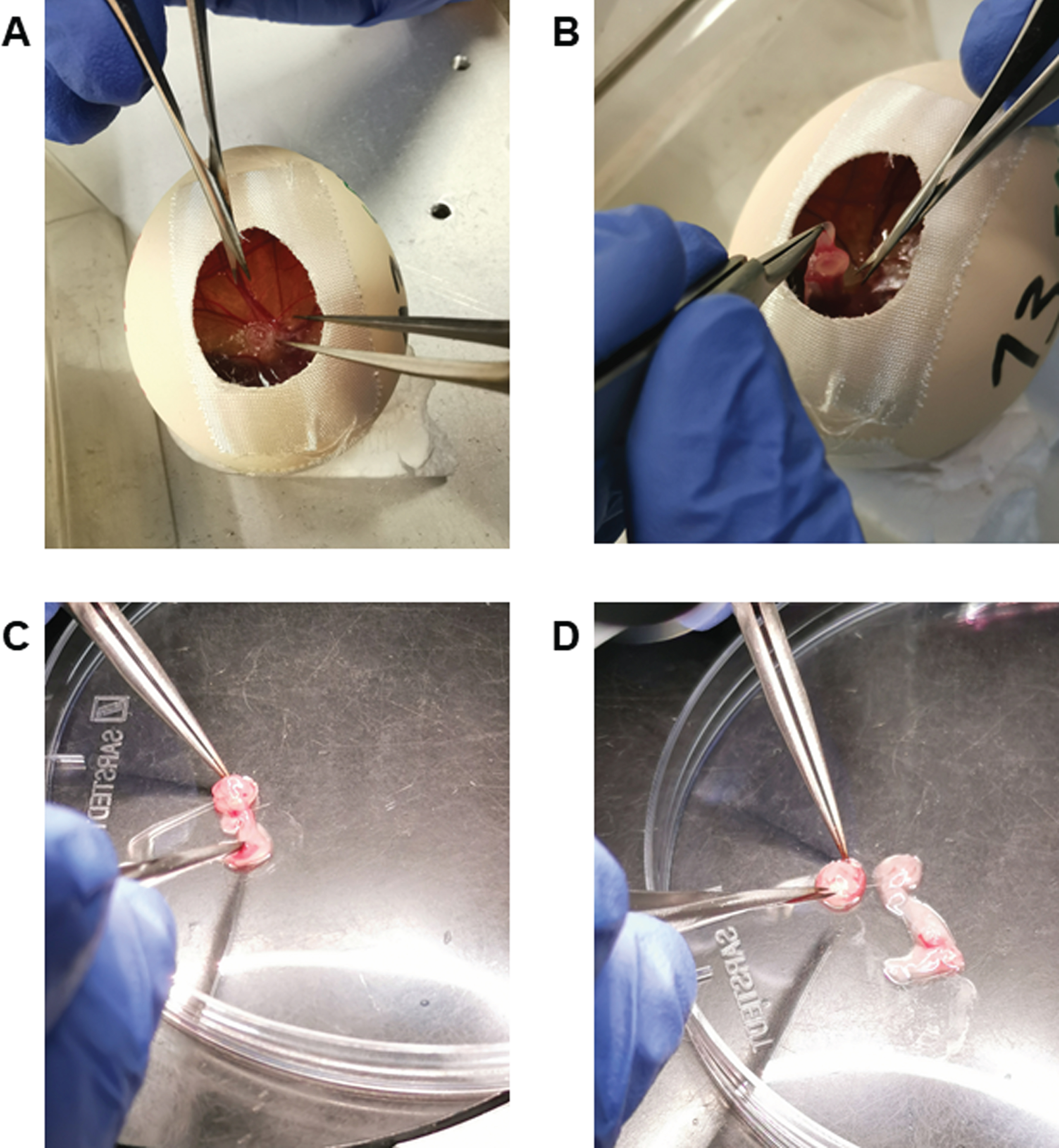
Excision of tumor from the CAM. A. Tumor on the CAM; B. Excision of tumor from the CAM with pincers; C. Separation of tumor material from the CAM in a petri dish; D. Completed separation of tumor material from the CAM.
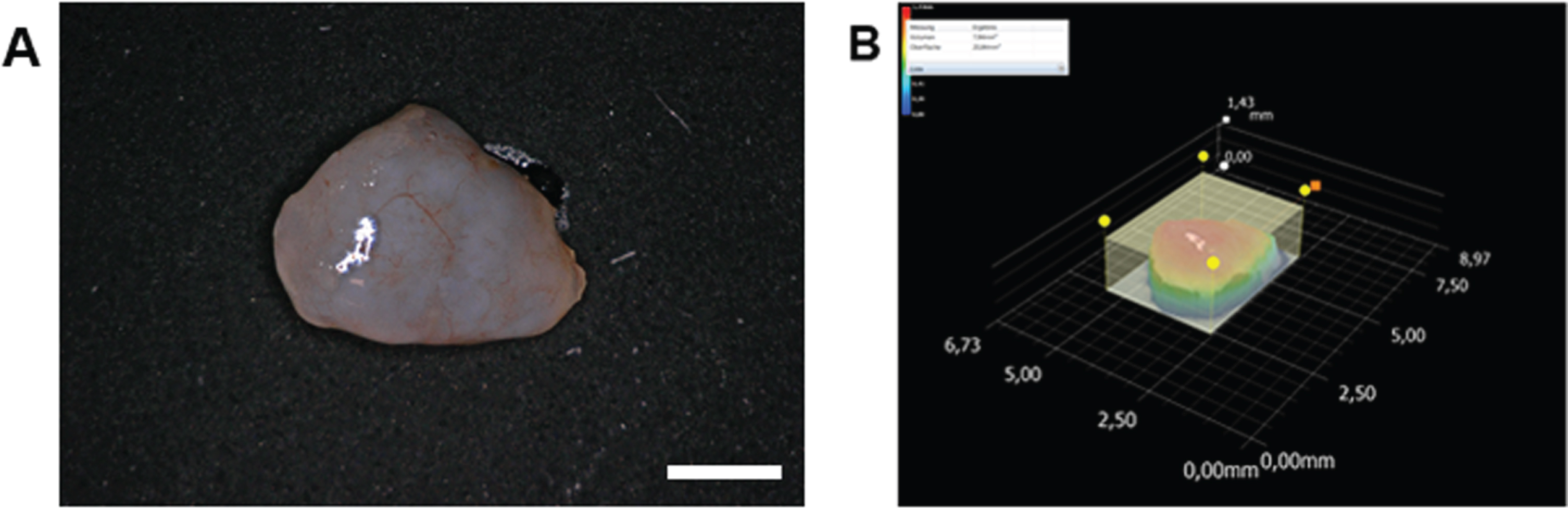
3D volume measurement of an osteosarcoma. A. Excised osteosarcoma; B. 3D osteosarcoma volume measurement. Scale bar = 1000°μm.
The grafting of rat and mouse tumors onto the CAM and the transplantation of these tumors as well as the transplantation of human neoplasms was first reported by Murphy et al. [23, 24]. However, the transplantation of human neoplasms was only moderately successful. Better results for tumor growth of human neoplasms were observed by Dagg et al., who transplanted various sarcomas onto the CAM but did not investigate the transplantation of osteosarcoma [24]. Grafted and transplanted sarcomas demonstrated rapid tumor growth and an initial transplantation of tumor material onto a newly incubated CAM model was performed successfully [25]. Ismail et al. demonstrated the transplantation of human ovarian tumors but only a second generation of tumors was generated here as well [26]. However, no separation between the various tumor areas was performed and subsequent differentiation of the different tumor parts concerning their growth behavior, angiogenesis and drug responsiveness was not investigated.
Sarcomas are characterized by their intratumoral and intertumoral heterogeneity, highlighting the necessity for the comparison of various tumor sections even while analyzing the same tumor. Especially osteosarcomas represent a very heterogeneous group, both at the intratumoral as well as at the intertumoral level [27]. Intratumoral heterogeneity can be caused by chromosomal aneuploidy, alterations of genes, genomic instability, as well as the presence of hypermutated regions. In addition, various gene mutations, such as mutations of TP53, MDM2, ATRX, DLG2 and RB have been linked to osteosarcomas [27]. However, 95% of osteosarcomas occur sporadically [27]. As shown in Fig. 2, we observed a temporary necrosis from the 3rd to 6th generation of the tumor tissue (pink part of the resected tissue) followed by macroscopically detectable revitalized tumor growth. This recurrent growth after necrosis could be caused by the presence of cancer stem cells in osteosarcomas which influence tumor growth, metastasis formation and drug resistance [28]. The diversity of these factors, contributing to the heterogeneity of osteosarcomas, highlights the role of extended investigation of intratumoral and intertumoral heterogeneity.
The grafting of human osteosarcoma cell lines was already successfully performed in various studies [21, 29–32]. However, to our knowledge, we reported the use of the CAM model for the grafting of osteosarcoma primary material for the first time and studied the tumor diversity by transplanting various osteosarcoma parts from one CAM to another. Differences between the generations and within the different parts were observed hereby, displaying the intratumoral heterogeneity of the osteosarcoma. Since osteosarcomas are bone sarcomas, these tumors consist of hard, calcified parts that make it a lot more difficult for these tissue parts to grow on the CAM than it is the case for soft tissue sarcomas.
Moreover, angiogenesis –the process of new blood-vessel growth –has an essential role in development, reproduction and repair [33] and plays a crucial role in tumor development [34]. It is described as one of the main hallmarks of cancer by Hanahan and Weinberg [35]. The development of blood vessels was also observed in the transplanted osteosarcomas, indicating that angiogenic proliferation had taken place during the tumor development on the CAM. The role of vascular endothelial growth factor-A (VEGF-A) for the angiogenesis of osteosarcomas has already been described [36]. Moreover, VEGF-A expression is increased by resistin which is expressed in high quantities in osteosarcomas [36]. The high level of vascularization of the CAM could also offer a possibility to study the behavior of various tumor parts for potential therapy, such as targeting resistin signaling in osteosarcomas. Moreover, long-term drug testing could be performed, due to the possibility of serial transplantations of tumor parts. This could also enable the detection of differences in drug responsiveness of various tumor parts which would improve innovative therapeutic approaches towards these types of cancers.
In summary, the 3D-in-vivo-CAM-model is well suited for the grafting and transplantation of primary osteosarcoma tissue which could offer further opportunities for tumor profiling of several tumor sections. This could potentially increase the versatility of this model and offer new pathways towards personalized medicine.
Conclusion
The utilization of the CAM model for the extended investigation of tumor heterogeneity in osteosarcomas proved to be possible, improving the versatility of the 3D-in-vivo-tumor-model. This could potentially facilitate the next step in the development of the methodology towards a precise individualized cancer model that addresses both the patient and the tumor individually.
Conflicts of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
We thank Dipl.Biol. Manfred Depner and Lucia Denk for their expert technical assistance.