
Abstract
Background:
The issue of whether there exists an own-effect on facial recognition in the elderly remains equivocal. Moreover, currently the literature of this issue in pathological aging is little.
Objective:
Our study was thus to explore the issue in both of healthy older people and patients with AD
Methods:
In study 1, 27 older and 31 younger healthy adults were recruited; in study 2, 27 healthy older adults and 80 patients (including subjective cognitive decline (SCD), mild cognitive impairment (MCI), and Alzheimer’s disease (AD) groups) were recruited. Participants received the Taiwan Facial Emotion Recognition Task (FER Task), and a clinical neuropsychological assessment.
Results:
No significant differences on the FER test were found among our groups, except for sadness recognition in which our MCI and AD patients’ scores were remarkably lower than their healthy counterparts. The own-age effect was not significantly evident in healthy younger and older adults, except for recognizing neutral photos. Our patients with MCI and AD tended to have the effect, particularly for the sad recognition in which the effect was significantly evident in terms of error features (mislabeling it as anger in younger-face and neutral in older-face photos).
Conclusion:
Our results displayed no remarkable own-age effect on facial emotional recognition in the healthy elderly (including SCD). However, it did not appear the case for MCI and AD patients, especially their recognizing those sadness items, suggesting that an inclusion of the FER task particularly involving those items of low-intensity emotion in clinical neuropsychological assessment might be contributory to the early detection of AD-related pathological individuals.
Keywords
INTRODUCTION
Facial emotion recognition (FER), one of the essential components of social cognition [1], represents the ability to recognize facial emotional ex-pressions. Deficits in FER may contribute to difficulties in social communication, damage self-esteem, and even diminish the quality of life [2]. Indeed, normal aging and patients with neurodegenerative diseases were reported to show declined and defective FER due to neurological changes and neurodegeneration, respectively [3–6]. To help families realize aging’s and patients’ difficulties and improve their life quality, choosing an appropriate clinical assessment for early detection of deficits in FER is undoubtedly crucial.
In fact, literature shows that some characteristics of emotional stimuli could affect the accuracy of FER, including cultural, gender-, and age-based factors [7–10]. Culture and gender factors have been demonstrated in vast studies [9–11]. However, few studies have examined the effects of photo age on FER. Lamont, Stewart-Williams, and Podd [12], using neutral faces as stimuli, found that observers of different ages recognize faces of their own age more accurately and rapidly as opposed to those of other ages. Such finding suggests that the age of a face constitutes an important factor that influences how we attend to and encode faces.
Indeed, the own-age effect or the own-age bias [7] has been proposed and investigated over the last decade while the results were inconsistent. Riediger and colleagues [13] found that middle-aged and older observers performed well in their target ratings of happiness and anger by the age of the own-age photos than did young observers. The study of Riediger et al. [14] also supported this finding in older participants. In contrast, Borod et al. [15] found that the expressions of older posers were rated significantly less accurately than those of younger posers for all groups. Further studies by Ebner and Johnson [16], Murphy et al. [17], and Hühnel et al. [18] also reported similar patterns. In addition, some studies found that this effect exists only in younger observers [19, 20].
It should be noted that some methodologic limitations existed in all these studies. First, the gender of the stimuli and observers were exclusively female [17, 18], even though it is known that gender can influence the accuracy of the results [10]. Second, the numbers of photos and observers were too small [15, 18]. Third, the target emotions in these studies were inconsistent; besides, some examined the own-age effect by averaging all accuracies of emotions [19]. These factors not only make it difficult to conclude the type of emotion reported consistently enough to show the own-age effect, but also make it hard to analyze effects of distinct emotions for the findings that different types of expressed emotions showed different effects on FER [10]. In conclusion, gender imbalance, small stimuli and observer sample sizes, incomparable types of emotions were selected, and ignoring separate effects of different emotions were existing methodologic problems in prior studies. It might be the reason that the results of examining the own-age effect on FER were inconsistent.
Although the own-age effect on FER has been investigated in normal age groups, even in Taiwanese [21], no study has considered this issue in Alzheimer’s disease (AD) patients. Indeed, the disease of AD could affect the performances in FER gradually, as the disease progresses [5], and changes may be evident even in the early phases [22].
Likewise, only one study has investigated the FER performances in patients with subjective cognitive decline (SCD), and no performance differences between patients and healthy adults were found [5]. On the contrary, impaired FER in sadness [23, 24], anger [23, 24], and/or low-intensity emotion [25] have been reported in patients with mild cognitive impairment (MCI), especially those with multi-domains MCI [26]. Nonetheless, these studies in SCD and MCI groups did not particularly attend to the issue of the age effect of photos on the participants’ performances when choosing the stimuli of the FER test. Moreover, no research has investigated whether or not the own-age effect on FER exists in patients with AD pathology.
As mentioned before, the better quality of life and well-being of healthy people not only rely on normal fundamental neurocognitive function, such as learning and memory and executive function, but also social cognition in which FER is one of its important underlying abilities. Indeed, the underlying distributed neural networks, particularly mesial temporal and the related prefrontal regions, for these two aspects of cognition are interconnected and overlapping [53]. Literature regarding the possible role of fundamental neurocognitive-domain functions playing in early detection and patient’s care in people with SCD, who have been reported an ensuing AD pathology at brain autopsy [60, 61], and with MCI and AD is currently accessible. However, this is not the case for studies concerning the feasible role of social cognition in the early detection and patient’s care in both healthy and patient individuals. Given that normal neural substrates for both aspects of cognitive-domain functions are overlapping, and no research has considered the effect of photo age when exploring this issue, the present study thus was to explore the issue of whether there exists an own-age effect on FER in SCD individuals and the preclinical and demented AD patients. The study objectives were as follows.
First, given that effects of distinct emotions are various, we re-examine the issue of whether there exists an own-age effect on the FER performance in the healthy elderly individuals after minimizing the methodological limitations evident in those prior studies. Secondly, in light of clinical utilities (mainly the early detection and patient’s care in terms of quality of life) and literature relatively scanty in brain-damaged cases, the present study was extended to explore the similar issue of the first one in patients with SCD, amnestic MCI (aMCI), and very mild AD.
METHODS
Participants
A total of 138 participants, ranging from 20 to 85 years old, were recruited for our study. In experiment 1, 27 older participants, ranging from 55–85 years old, were enlisted through notices advertising our study in their communities, and 31 younger participants, ranging from 20–35 years old, who were either college students or working individuals, were recruited through notices advertising the study on the internet. In experiment 2, 27 older participants in experiment 1 were also used as control subjects, and 80 patients (55–85 years old), with memory complaints were invited from the Neurology Clinic of the National Taiwan University Hospital.
Patients were interviewed, screened at the clinic, and diagnosed by neurologists and a clinical neuropsychologist. Individuals who performed normally in the clinical neuropsychological assessment with a reported subjective decline in memory within five years [27] were classified into the SCD group. Individuals whose performances on the episodic-memory task was 1.5 standard deviation or more below the normative data with normal performance on other neuropsychological assessments were classified into the MCI group [28]. Individuals who met the established criteria of the National Institute on Aging and Alzheimer’s Association and had a clinical dementia rating (CDR) of 0.5 points were divided into the very mild dementia due to AD group. Twenty-seven community-dwelling volunteers without memory complaints were recruited into the healthy control (HC) group. Thirty-one younger volunteers were recruited into the younger group. Exclusion criteria included a current or past history of alcohol or substance abuse, intellectual disability, brain injury, stroke, endocrine dysfunction, neurological disorders, or psychiatric disorders. All participants had normal or corrected vision and hearing abilities. Patients with cardiovascular disease and its risk factors were excluded if their cardiovascular disease status exceeded 4 points on the Hachinski Ischemic Score (HIS) [29].
Measurements
FER task
To assess the FER ability, we designed the FER Task. The stimuli were taken from the database of the East Asian face expression stimuli [21], consisting of 628 photos, including male and female, younger and older Taiwanese presenting seven face emotion expression categories (happiness, sadness, anger, surprise, fear, disgust, and neutral). All individuals in these photos produced prototypical expressions based on the Facial Action Coding System [30, 31]. We excluded photos in the database with different background and brightness which results in 406 photos (58 individuals with seven expressions each) selected as the emotional stimuli in our pilot study. They were colored, front-view head shots on white backgrounds.
Our Task used the multiple forced-choice rating, and the 5-point Likert scale to measure the accuracy and the intensity (ranging from 1: very slightly or not at all to 5: extremely) of each photo, respectively. The response options appeared in black on a white background below the photos, presented in the same order. For reducing the practice effect, the presentation order of emotional faces was identical for each participant. The lists were pseudo-randomized with the constraint that no more than two faces of the same face presenter or the same facial expression were repeated in a row. Stimulus presentation and response collection were controlled using E-Prime [32] and were displayed on a 14-inch notebook.
During the FER Task, one face was presented at a time. Participants were asked to judge the emotion of the face quickly by pressing one of the response buttons on a button box. Then they were instructed to rate the intensity of the selected emotion of the photo. The instruction was, taking a happy expression for example, “how intense does this image look in terms of happiness?”). The photos and the response options were always presented for reducing the need of memory.
A pilot test was designed to establish the applicability of the tasks. An additional 20 younger adults and 20 healthy older adults were recruited to rate the emotional category and the intensity of the 406 emotional faces. The procedure and design were the same as in the normal experiment. After the pilot test, we removed disgust from our emotion category because disgust was highly mislabeled as anger thus showed lower accuracy, and it tended to be seen as a subtype of anger [33]. Besides, although the results showed fear was highly mislabeled as surprise, we removed surprise, not fear, because it has been reported to be the most difficult emotion to decode [10, 34]. Moreover, we also screened out the photos from 21 individuals because the accuracy of these was lower than 50% of the overall score. One hundred and fifty-five pictures, in which there are 9 old female and male, 6 young female, and 7 young male photos for each of the 5 emotion types and neutral, were finally selected as stimulating materials for the FER Task. The age of older pictures ranges from 55–80 years old; the age of younger pictures ranges from 20–30 years old.
Neuropsychological assessment
All participants underwent a neuropsychological assessment conducted by a neuropsychologist or a project coordinator. Mini-Mental Status Examination (MMSE) was performed initially. To rule out the possibility of deficits in intellectual ability, participants’ intellectual quotient (IQ) performances on the Wechsler Adult Intelligence Scale-Third Edition (WAIS-III) or WAIS-IV were collected through the record of their recent neuropsychological examination. The Logical Memory Subtests I and II of the Wechsler Memory Scale-III [35, 36] were performed to obtain the scores for episodic memory. To rule out perceptually based face processing deficits, the Short Form Benton Facial Recognition Test [37] was administrated. For emotional status evaluation, all older participants underwent the Taiwan Geriatric Depression Scale (TGDS) [38] test. For patients with SCD, MCI, and AD, a neuropsychologist also interviewed their informant to complete the CDR.
Procedure
All participants have explained the purpose of the research and signed an informed consent form, which was approved by the institutional review board of the National Taiwan University Hospital. Detailed demographic data are shown in Table 1. Information regarding participants’ age, education, medical history, current health status, and medication regimen was obtained through a semi-structured interview. All older participants underwent the TGDS and the HIS. The MMSE or/and neuropsychological assessment were then administered for all participants. Finally, the FER Task was presented.
Demographic Characteristics and Cognitive Status of Younger and Older Observers in Experiment 1
Values are expressed as mean and standard deviation or mean/maximum score and standard deviation with the exception of those denote percentage and number of individuals for gender. IQ, intelligence quotient.
Statistical analysis
All statistical tests were performed using the Statistical Package for Social Sciences (SPSS version 22.0). Demographics and clinical characteristics were compared using a one-way/two-way analysis of variance (ANOVA) or chi-square tests. As the results of ANOVA revealed significant between groups, Scheffe’s pairwise-comparison analysis was used for post-hoc pairwise-comparison analysis. To test whether the own-age effect existed in older adults in distinct emotions (experiment 1), and the same issue in SCD, MCI, and AD patients in distinct emotions (experiment 2), two mixed-effects analysis of covariance (ANCOVAs) with three factors was utilized. To control any demographic and/or neuropsychological performance variables found to be significantly associated with individual emotion recognition measures, the factor of education was controlled in experiment 1, and age, education, and IQ were controlled in experiment 2. Dunn-Bonferroni pairwise comparisons were set for the post-hoc analysis following ANCOVAs, and the level of significance was fixed at <0.05.
Effect sizes were analyzed with partial eta squared (
RESULTS
Experiment 1
Demographics and clinical characteristics
Table 1 presents group comparisons of demographics and clinical characteristics in experiment 1. A significant difference was observed regarding education and age, which indicated that the education levels of younger groups were higher than those of the older groups (F(1, 56) = 18.61, p < 0.001,
Does the own-age effect of FER exist in normal aging?
To examine this issue in different emotions, we conducted a mixed-effects ANCOVA with three factors: group age (young versus old, between-subjects), photo age (young versus old, within-subjects), and stimulus emotion (within-subjects). To control the possible effects of education, we included education as a covariate. The dependent variable was the proportion of correct classifications for each stimulus emotion in different photo ages (i.e., younger and older faces). The results are shown in Table 2.
Results of ANCOVA on Decoding Accuracy as a Function of Emotion, Photo Age, Group Age, and Their Interactions in Experiment 1
No main effect of group age, photo age, and emotion was revealed. However, a significant two-way interaction of photo age× emotion (F(4, 220) =5.086, p = 0.001,
To examine the three-way interaction in more detail, we further performed a simple interaction analysis, revealing a significant simple interaction effect of photo age× emotion for both younger and older observers. We further conducted a simple main effect analysis. In recognizing happiness, sadness, and fear, there is a significant simple main effect of photo age for both younger and older observers. The younger faces were more accurate than the older ones for both groups in fear and sadness recognitions, while the reverse was occurred in performing happiness. In recognizing anger, no significant simple main effect of photo age was observed for both younger and older observers. However, for the possibility that the effect of angry might be eliminated by other emotions due to analyzing in terms of total accuracy, we conducted separate ANCOVAs for each emotion with education as a covariate. The results showed that a significant main effect of observer age appeared only in anger recognition (F(1, 55) = 5.604, p = 0.021,
Experiment 2
Demographics and clinical characteristics
Table 3 presents group comparisons of demographics and clinical characteristics. The results showed main effects of age (F(3, 103) = 12.83, p < 0.001), education (F(3, 103) = 3.184, p = 0.027), IQ (F(3, 103) = 4.643, p = 0.004), and MMSE score (F(3, 103) = 10.41, p < 0.001) across four groups. Post hoc pairwise-comparison analyses using Scheffe’s method indicated that the age of the HC group was younger than that of the aMCI and AD groups, and the age of SCD group was younger than that of the AD group. The education level in the aMCI group was significantly lower than that in the SCD. Individuals in the HC and SCD groups showed higher IQ scores than did individuals in the AD group, whereas the aMCI group did not differ significantly from other groups. HC, SCD, and aMCI groups had higher scores on the MMSE than AD groups. No differences in terms of other demographics, clinical characteristics, or neuropsychological performance were found between HC and SCD groups.
Demographic Characteristics and Cognitive Status of SCD, MCI, AD, and Normal Control Groups in Experiment 2
SD, standard deviation; HC, healthy control; SCD, subjective memory decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease; IQ, intelligence quotient; MMSE, Mini-Mental Status Examination. ap < 0.001; HC versus MCI. bp < 0.001; HC versus AD. cp < 0.001; SCD versus AD. dp < 0.05; SCD versus MCI. ep < 0.05, eep < 0.001; HC versus AD. fp < 0.05, ffp < 0.001; SCD versus AD. gp < 0.05; HC versus MCI. hp < 0.05; MCI versus AD.
Is the own-age effect evident in the patients while performing the FER?
To investigate this issue in SCD, aMCI, and AD groups, and to evaluate the FER abilities in these groups, a mixed-effects ANCOVA with three factors: group (between-subjects), photo age (young versus old, within-subjects), and stimulus emotion (within-subjects), was conducted. To control the possible effects of age, education, and IQ, we included these factors as covariates. The dependent variable was the proportion of correct classifications for each stimulus emotion in different photo ages (i.e., younger and older faces). The results are shown in Table 4.
Results of ANCOVA on Decoding Accuracy as a Function of Emotion, Photo Age, Group, and their Interactions in Experiment 2
The results revealed a significant main effect of group (F(3, 100) = 7.342, p < 0.001,
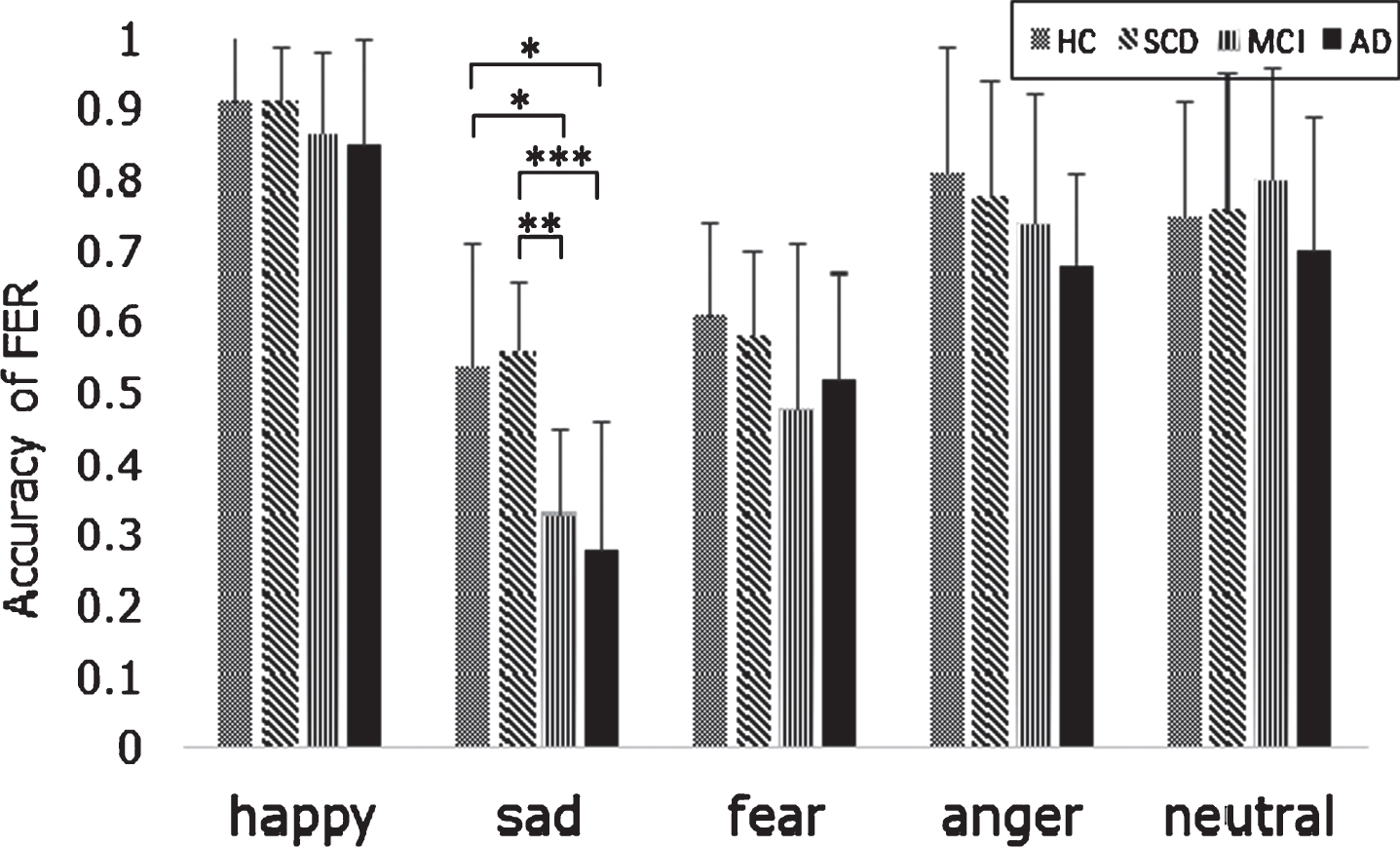
Group differences in accuracy of facial emotion recognition (FER). Total point of the accuracy of FER is one. HC and SCD groups performed significantly better than aMCI and AD groups only in sad recognition of the Facial emotion recognition task. HC, healthy control; SCD, subjective memory decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease; error bar means standard divivation; *p < 0.05, **p < 0.01, ***p < 0.001.
We further checked in detail in sadness across groups to account for the possibility that the own-age effect in sadness might be diminished by averaging total emotion. A mixed-effects ANCOVA in sadness with two factors: photo age (young versus old, within-subjects) and group age (young versus old, between-subjects) was conducted. No significant interaction between photo age and group (F(3, 100) = 1.261, p = 0.292) was found. However, a tendency of aMCI and AD groups performed more accurately in recognizing older faces compared to younger ones, while HC and SCD groups did reversely was found (see Fig. 2). To further explore the mislabeled emotional type presented by aMCI and AD groups, two-way mixed ANOVAs were conducted between two groups. Post-hoc analysis using the Bonferroni method found that the scores of judging sadness to anger and neutral were not significantly different from those of correctly judging. To further consider the effect of different photo age, we conducted separate one-way ANCOVAs between the four groups. The dependent variable was the proportion of wrong classifications from sad to anger and to neutral in younger and older faces, respectively. The results showed a significant difference (F(3, 100) = 4.692, p = 0.004,
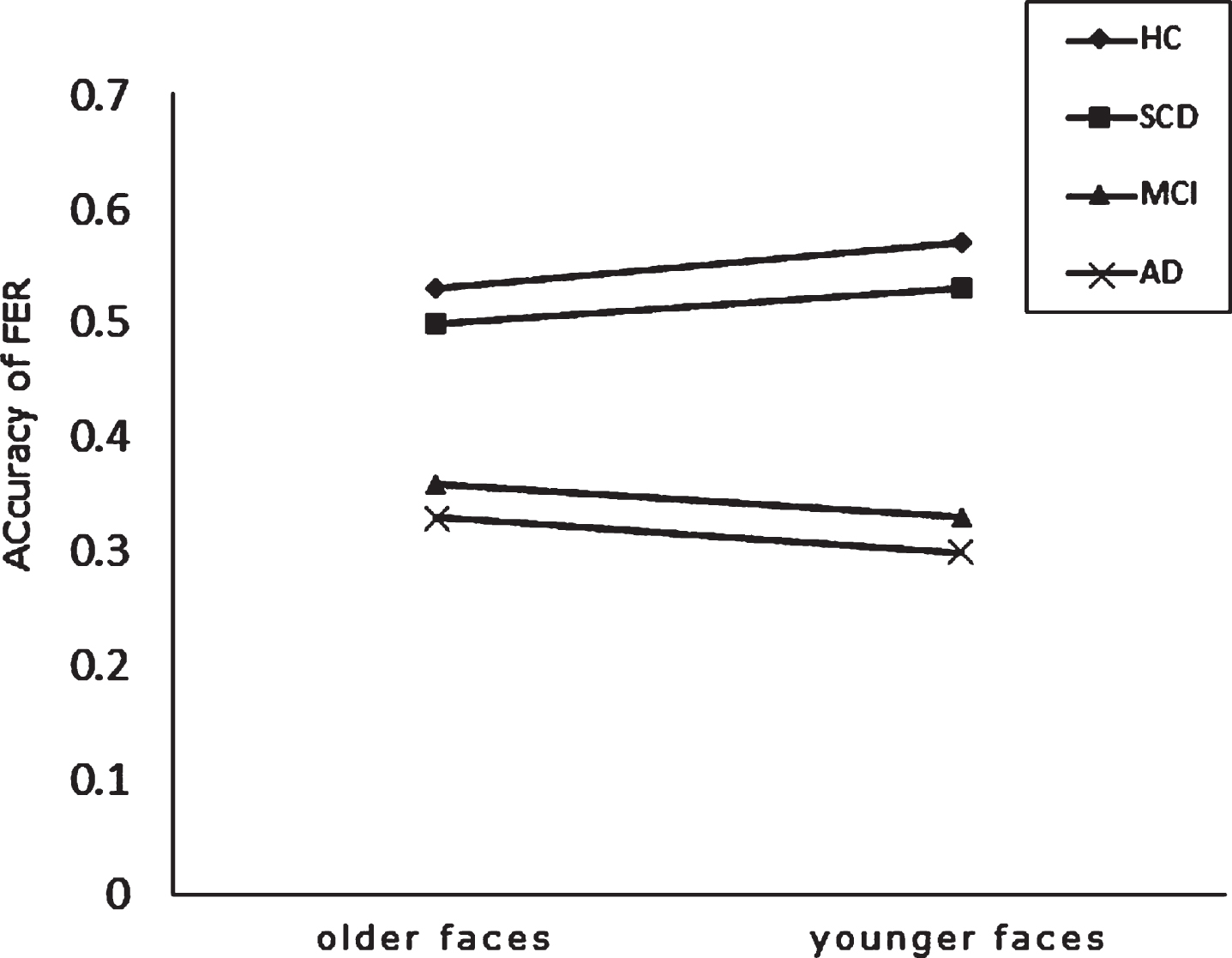
The profile presented group performances (total score of accuracy is one) when recognizing sadness in photos of younger and older performers. No significant interaction between photo age and group was found. However, aMCI and AD groups tended to perform more accurately in recognizing old-aged photos compared to young-aged ones, while HC and SCD groups did reversely. HC, healthy control; SCD, subjective memory decline; MCI, mild cognitive impairment; AD, Alzheimer’s disease.
Clinical utilities
Because sadness recognition presents a remarkable opportunity to discriminate patients who showed deficits in FER, we conducted the ROC curve analysis in sadness scores between SCD and aMCI. The results indicated that the sadness accuracies in younger and older faces were different between SCD and aMCI groups (area under the curve [AUC] of younger faces = 80%; AUC of old faces = 77%). According to the Youden index [39], the data showed that using a cutoff score of 0.35 for the accuracy in younger faces and a cutoff score of 0.36 for the accuracy in older faces yielded the most desirable combination of sensitivity (91%) and specificity (39%) in younger faces and sensitivity (81%) and specificity (39%) in older faces respectively for identifying significant differences between the SCD and aMCI groups on the FER.
DISCUSSION
Our study examined whether the own-age effect exists in healthy adults and patients with SCD, aMCI, and very mild AD when performing the FER Task. Our discussion presents in two parts: the results in healthy adults and patients, respectively.
Does the own-age effect of FER exist in healthy adults?
Methodologically, studies on the own-age effect mostly involve in two age-related factors, the cohort-effect and the photo age effect. Considering the cohort-effect, no group age effect was found in terms of average accuracy of emotion recognition. However, having analyzed distinct emotion stimuli, the old observers performed better than younger ones in anger recognition. Our results were inconsistent with those findings of previous studies that performances of older adults were inferior to those of their younger counterparts in sadness, fear, and anger recognitions [40–42]. The discrepancy might be due to the higher educational level in our healthy older participants. Although the effects of higher education on preventing MCI and AD remain equivocal, favorable study findings indicated that people with higher education not only performed cognitive tests better than those with lower-educated ones, but also delayed the onset of cognitive impairment [43]. Besides, Pietschnig et al. [5] also reported that higher-educated individuals did have better performance on the FER. Accordingly, it appears that higher education facilitates protective effects not only on the decline of cognitive function [44] but also of emotional recognition.
In respect to the issue of the photo age effect, the present study found that the younger-face was significantly easier than the older-face recognition for both younger and older observers in fearful and sad recognition; however, the reverse was found in happiness. The first results were consistent with those of previous studies [45, 46]. Such an outcome, as suggested by researchers [47, 48], may be attributed to age-related changes of older faces (e.g., wrinkles and folds) that were more dissimulated, mixed, and fragmental than younger ones. However, our results in happiness were inconsistent with those findings of prior studies [13, 49]. The discrepancy might be due to two methodologic limitations. First, our posed photo stimuli were less spontaneous in nature, thus they were less ecological valid than spontaneous ones [17, 50]. Second, the intensities of our happy photos in younger faces were significantly lower than those of the older faces in happiness (see Supplementary Table 2). That is, because the younger performers in our photos tended to present low-intense happy expressions than the older performers, both younger and older observers tended to misrecognize happy expressions to neutral ones in younger photos.
Taken together, the present study did not find the own-age effect on FER in older observers. Likewise, it was also the case for younger observers, with the exception of neutral recognition. Given our results consistent with most studies [15–18], the own-age effect on FER appeared not remarkable, irrespective of younger or older healthy people. However, the present results were inconsistent with other prior studies displaying the own-age effect evident in older adults when performing happiness and anger recognitions [14, 20], and in younger adults [19, 20] when performing the happiness, anger, and sadness ones. The inconsistency might be due to the unrepresentative sample [19, 20]; limited stimuli of the measure [14], and the discrepancy of the emotional rating format [13], particularly, the last one. The forced-choice approach used in our and most studies for measuring each of the photos’ stimuli is different from the multi-dimensional response format (measuring the percentage across all emotions for every individual photo) used in Riediger and coworkers’ study [13]. In fact, the type of emotional experiences in real life is always multi-faceted [51]; thus, the latter is more ecologically valid in nature. Nevertheless, whether this methodologic discrepancy can fully attribute to the inconsistent results remains further investigation.
Is the own-age effect evident in the patients while performing the FER?
Our study examined the FER performances in SCD, aMCI, and very mild AD patients after minimizing the methodologic problems. FER deficits were found in the MCI and AD groups in recognizing sadness only (see Fig. 1). Furthermore, these patients tended to mislabel sadness for anger and neutral expression when perceiving younger and old faces respectively. Our results supported the previous findings indicating that FER deficits occurred in MCI and early-stage AD patients [6, 52], but not in SCD patients compared to healthy older adults [5].
Davidson, Putnam, and Larson [53] proposed that the neural network responsible for emotion involving the orbital prefrontal cortex, ventromedial prefrontal cortex, dorsolateral prefrontal cortex, amygdala, hippocampus, hypothalamus, anterior cingulate cortex (ACC), insular cortex, and ventral striatum. Based on the locationist hypothesis, each of the distinct emotions has its underlying neural substrate [54]. In fact, a recent study found that the ACC plays an essential role in processing sadness-related information [55]. Accordingly, it appears feasible to speculate such sad recognition problems possibly due to the ACC dysfunction which might indirectly result from pathological changes of the hippocampal cortices and related regions commonly evident in early AD and aMCI [56]. Nevertheless, given that a small group of the patients (particularly early AD) was sampled in our study, and the mechanism for the results of defective recognition of sadness remains unclear, further investigation on a large scale is necessary.
Regarding the issue of the own-age effect, the present study found that aMCI and very mild AD patients tended to have such effect compared with the healthy compartments (see Fig. 2). However, it was not significant, and the accuracy of FER in recognizing the own-aged photos remained low.
In short, our study found that aMCI and very mild AD patients showed defective FER in sadness with a tendency to mislabel it to anger and neutral in younger and older faces, respectively. Accordingly, it appears that a measure with low-intensity of FER (i.e., sadness) can be sensitive to detect patients with very mild AD and aMCI. Our results also revealed that a tendency of the own-age effect occurred in patients.
To our knowledge, our study is the first one to investigate several issues, including the own-age effect on FER in patients with AD, and is also one or two studies examining FER functioning in individuals with SCD. However, some limitations were existed in the present study: 1) The educational level of all participants in this study was relatively high, especially in the SCD group. 2) The measuring format (i.e., the forced-choice approach) and the type of photos (posed and static photos) were less ecological validity. 3) aMCI group was not classified into single or multiple domains. 4) Given the doctrine of “ZhongYong” responding style to the odd-level rating scale in most Taiwanese/Chinese people [57, 58], our participants might have a biased rather than a true rating on the 5-point Likert scale for the intensity of each emotional photo stimulus. 5) The confounding effect due to the incomparable intensity of facial-emotion stimuli between younger and older individual photos in our study might influence the results though currently adequate matching means remains unavailable. 6) Our task lacked the measurement of reliability and validity. 7) The sample sizes were relatively small. Further studies on these issues are thus requisite.
In summary, although the own-age effect was not evident in healthy adults, the tendency of such an effect appeared in patients with aMCI and very mild AD in sadness recognition. Our study elucidated the potential pathophysiological mechanism underlying the relationships between AD and the sad recognition problems. Nevertheless, due to small sampling in our study and still lacking neuroimaging evidence, future research with a larger sample size and regarding the neuroimaging confirmation is needed. Even though different ages of photos showed no effect on FER, including photos of older individuals as clinical stimuli might increase the medical relationship with older patients. Nevertheless, the hit rates of certain expressions in our stimuli database were low. Further research using the multi-dimensional response format and the dynamic and spontaneous photos might eliminate the problem.
Footnotes
ACKNOWLEDGMENTS
Thanks to Joshua Oon Soo Goh for providing the stimuli. Thanks to Cheng-Chang Yang for commenting on a revision of the manuscript. Data collection was assisted by Yu-Hsiang Cheng and Yu-Hsuan Sun. Finally, we thank all the participants and their families for their involvement and support in this study. This study was partially supported by grants from the Ministry of Science and Technology, Taipei, Taiwan (MOST 109-2410-H-468-013).