
Abstract
Background:
The differentiation of idiopathic normal pressure hydrocephalus (iNPH) from neurodegenerative diseases such as Alzheimer’s disease (AD) and dementia with Lewy bodies (DLB) is often challenging because of their non-specific symptoms. Therefore, various neuroradiological markers other than ventriculomegaly have been proposed. Despite the utility of disproportionately enlarged subarachnoid-space hydrocephalus (DESH) for the appropriate selection of shunt surgery candidates, the specificity and neuropathology of this finding have not been sufficiently evaluated.
Objective:
Investigation of the clinicopathological features and comparison of the neuroradiological findings between DESH with postmortem neuropathological diagnoses (pDESH) and clinically-diagnosed iNPH (ciNPH) patients are the main purposes of this study.
Method:
In addition to the retrospective evaluation of clinicopathological information, quantitative, semiquantitative, and qualitative magnetic resonance imaging (MRI) indices were compared between pathologically-investigated 10 patients with pDESH and 10 patients with ciNPH
Results:
Excluding one patient with multiple cerebral infarctions, the postmortem neuropathological diagnoses of the pathologically-investigated patients were mainly neurodegenerative diseases (five AD, one DLB with AD pathologies, one DLB, one argyrophilic grain disease, and one Huntington’s disease). In addition to the common neuroradiological features
Conclusion:
Hippocampal atrophy and deformation with temporal horn enlargement seem to be characteristic neuroradiological findings of long-standing severely demented patients with DESH and neurodegenerative diseases, mainly advanced-stage AD.
Keywords
INTRODUCTION
Disproportionately enlarged subarachnoid space hydrocephalus (DESH) is a neuroradiological finding indicative of communicating hydrocephalus characterized by ventriculomegaly, dilated sylvian fissures, and, tight high convexity sulci [1]. This finding is now recognized as a characteristic imaging feature of idiopathic normal pressure hydrocephalus (iNPH) and known to predict neurological improvement and positive shunt outcome in patients with iNPH [1, 2]. Additionally, the DESH score comprised of five magnetic resonance imaging (MRI) findings (ventriculomegaly, dilated sylvian fissures, tight high convexity sulci, small callosal angle, and focal sulcal dilation) has been advocated as a useful marker to predict neurological improvement and prognosis after shunt surgery in patients with iNPH [3, 4].
Because the presence of neuropathological disorders is hypothesized to hinder shunt responsiveness in patients with iNPH, identification of these neuropathologies is important to avoid unnecessary invasive shunt surgeries with disappointing results in the clinical management of iNPH [5]. Notably, recent studies have reported that the iNPH-like morphological change can be observed in patients with neurodegenerative diseases including advanced-stage Alzheimer’s disease (AD), progressive supranuclear palsy (PSP), and dementia with Lewy bodies (DLB) [6 –9]. This raises the suspicion about the specificity of DESH. Furthermore, while some studies have compared the MRI findings between iNPH and clinically-diagnosed neurodegenerative diseases such as AD and PSP, the neuropathological and neuroradiological features in the pathologically-investigated cases with DESH on antemortem MRI have not been sufficiently evaluated [10 –13]. Because advanced-stage AD and PSP often showed characteristic morphological changes in advanced-disease stages (i.e., severe hippocampal atrophy and deformation with ventricular enlargement of AD and midbrain atrophy of PSP), we assumed that these morphological changes could be an imaging marker of neurodegenerative pathologies even in patients with DESH [14, 15]. These issues prompted us to explore in detail the neuropathological and neuroradiological findings using autopsied cases. This study has two main purposes: 1) investigation of clinicopathological and neuroradiological features in pathologically-investigated patients with DESH on antemortem MRI (pDESH); 2) comparison of neuroradiological features between pDESH and clinically-diagnosed iNPH (ciNPH) patients. Evaluation of pathologically-investigated cases is expected to provide new insights for the radiological diagnosis in patients with DESH.
MATERIALS AND METHODS
Subjects
This is a retrospective, double-center, consecutive case series. The subjects belonged to one of the following two categories: 1) autopsied patients with DESH on antemortem MRI, and 2) patients with clinically-diagnosed iNPH. They were selected by searching the available medical records between January 2013 and December 2020. Patient backgrounds were standardized by applying the following inclusion criteria: 1) pDESH: neuroradiological diagnosis of DESH on MRI, and neuropathological diagnoses according to the published criteria of AD, DLB, argyrophilic grain disease (AGD), Huntington’s disease, and iNPH in postmortem pathological evaluation [1 , 16–20], 2) ciNPH: clinical diagnoses according to the published criteria in clinically-diagnosed iNPH [21]. This study was approved by our institutional review boards, and informed consent was obtained from patients or bereaved families to use the data for academic purposes. The privacy of patients was completely protected. This retrospective double-center study was carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
MRI protocol and image analysis
All patients underwent MRI examination using either a 1.5-T scanner (MAGNETOM Aera®; Siemens Healthcare, Erlangen, Germany) or 3-T scanner (Ingenia; Philips Medical Systems, Best, The Netherlands) with a 20-channel Head/Neck coil. In addition to 5-6 mm-thick axial T2-weighted image (T2WI), 3D T1-weighted image (3DT1WI) with 1.25 mm-thick magnetization-prepared rapid gradient-echo (MPRAGE), 0.65 mm-thick fast low angle shot (FLASH) or 0.75 mm magnetization-prepared spoiled turbo multiple gradient echo sequence with inversion pulse for QSM (MPQSM) was obtained. Additionally, the multiplanar reconstruction technique was performed to make a 1 mm-thick sagittal and oblique coronal plane perpendicular to the hippocampus body or anterior commissure - posterior commissure line.
The neuroradiological features were evaluated using quantitative, semi-quantitative, and qualitative markers.
Quantitative markers
Ventricular dilation was quantified using Evans’ index and MR hydrocephalic index (MRHI) on axial T2WI [12, 22]. The callosal angle, midbrain area and midbrain-to-pons (MtP) ratio were measured using the reconstructed oblique coronal and sagittal 3DT1WI [23, 24]. To assess the shape and dilation of the temporal horn, three quantitative indices were measured on the oblique coronal reconstructed 3DT1WI. Hippocampal angle (HPA) and inferior horn area (IHA) represent the angle between two lines parallel to the long axes of the bilateral hippocampal heads, and area of the bilateral inferior horn of the lateral ventricle, respectively. The ratio between the IHA and HPA (i.e., IHA/HPA) was referred to as the “IHPA index” [15].
Semiquantitative and qualitative markers
Degrees of medial temporal atrophy were semi-quantitatively assessed using the well-known Scheltens’ MTA score [25]. Additionally, the DESH score categorized from 0 to 10 by the presence of ventriculomegaly, dilated sylvian fissures, tight high-convexity, small callosal angle, and focal sulcal dilation was assessed [3]. Finally, the presence or absence of the hummingbird sign indicating midbrain atrophy was visually evaluated [14].
For the imaging analyses, two raters, a neuroradiologist and neurologist with 16 years (rater 1, K.S.) and 12 years (rater 2, Y.U.) of neuroradiologic experience with MR imaging of dementia, who were blinded to all the patients’ information independently evaluated all MR images. In cases of interobserver disagreement, final decisions were reached by unanimous consensus.
Statistical analysis
Statistical analyses were performed using IBM SPSS statistics 24 (IBM SPSS Inc, Chicago, IL, USA). The Welch t-test for normally distributed data (age and Mini-Mental State Examination score: MMSE), Mann-Whitney U tests for non-normally distributed data (disease duration, modified Rankin scale, Barthel index, MRHI, IHA, IHPA index, and MTA score), and Fisher’s exact test for categorical data (gender, hummingbird sign) were performed for comparisons between two subject groups. Additionally, to remove the effect of longer disease duration, analysis of covariance (ANCOVA) using disease duration as a covariate was performed for normally-distributed variables (Evans’ index, callosal angle, midbrain area, MtP ratio, DESH score, and HPA). Resulting p values were considered as statistically significant if < 0.05. Considering the pre-established hypotheses (i.e., more severe medial temporal atrophy in pDESH than ciNPH) and risk of the type II error due to excessive adjustments, Family-wise error adjustments were not performed in this study [26].
RESULTS
Clinicopathological features
After excluding three patients without MRI examination and one patient without cerebrospinal fluid (CSF) removal test, 10 pathologically-investigated patients with DESH and 10 clinically-diagnosed iNPH patients were included in this study. Patients’ characteristics are summarized in Table 1. Based on their classic triad symptoms, DESH on MRI, and improvement of symptoms after CSF removal tests, all 10 ciNPH patients received the diagnoses of probable iNPH according to the published Japanese guideline [21]. After the CSF removal tests, all patients showed more than 10%improvement from the baseline on the 3-m timed up and go test [27]. Except for two oldest-old patients, eight patients were shunted by neurosurgeons. Because nearly half of them were transferred to other rehabilitation hospitals and long-term care sanatoriums, it was difficult to follow the clinical course of all patients after shunt surgeries.
Patients’ characteristics
Data are shown as absolute numbers or the mean±standard deviation. ciNPH, clinically-diagnosed idiopathic normal pressure hydrocephalus; m, month; MMSE, Mini-Mental State Examination; MRI, magnetic resonance imaging; N.A., not applicable; pDESH, pathologically-proven patients with disproportionately enlarged subarachnoid-space hydrocephalus; y, years. *Welch t-test; †Fisher’s exact test; ‡Mann-Whitney U test; |Disease duration from symptom onset to MRI (m); | |Due to the severely demented condition, it was difficult to perform MMSE at the same time as the other clinical scales and MRI.
In pDESH patients, clinical records such as admission summaries were retrospectively checked to evaluate the clinical diagnoses and symptoms until the timing of MRI examinations. Because of the absence of the classic triad (i.e., cognitive impairment, gait disturbance, and urinary incontinence), antemortem diagnostic CSF removal tests were not performed in any of the pDESH patients. None of these patients had iNPH as their most likely clinical diagnosis at the time of death. In addition to the longer disease duration, pDESH patients showed worse cognitive and functional scales including lower MMSE and Barthel index, and higher modified Rankin scale than those of ciNPH patients (p≤0.001, 0.001, 0.001, and 0.002, respectively). The postmortem neuropathological diagnoses of pDESH patients were composed of both neurodegenerative pathologies (AD in five, DLB comorbid with AD in one, DLB in one, AGD in one, Huntington’s disease in one) and non-neurodegenerative pathology (multiple cerebral infarctions in one) (Table 2). Although periventricular white matter rarefaction and ependymal tears that were similar to those of iNPH were detected, no specific neuropathologic changes such as subarachnoid hemorrhage, meningitis or aqueductal stenosis sufficient to cause hydrocephalus were identified in any of the pDESH patients (Fig. 1).
Clinicopathological features of pathologically-proven DESH patients
AD, Alzheimer’s disease; AGD, argyrophilic grain disease; BS, bedridden state; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; CI, cerebral infarction; DLB, dementia with Lewy bodies; F, forgetfulness; GI, gait impairment; HD, Huntington’s disease; IR, irritability; LBD, Lewy body disease; MMSE, Mini-Mental State Examination; mRS, modified Rankin scale; N.A., not applicable; NFT, neurofibrillary tangle; PD, Parkinson’s disease; R, rigidity; RBD, REM sleep behavior disorder; TDP, TAR DNA-binding protein 43. *Due to the severely demented condition, it was difficult to perform MMSE at the same time as the other clinical scales and MRI.
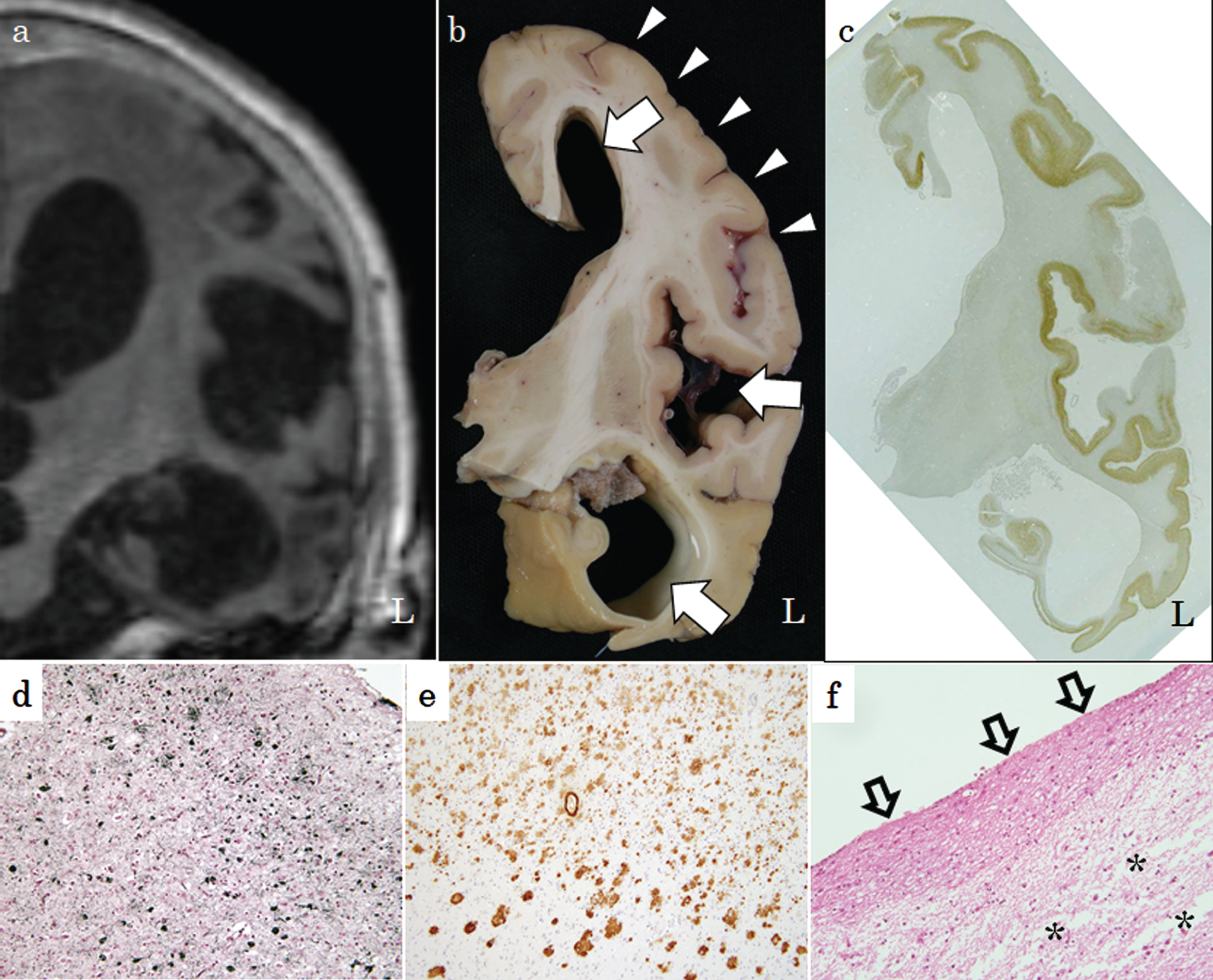
Coronal 3DT1WI and neuropathological findings of a demented 81-year-old female. Ventriculomegaly with dilated left temporal horn and Sylvian fissure (b; arrows) accompanied by tight high convexity (b; arrowheads) on a macroscopic specimen is consistent with that of MRI (a). Diffuse positive staining for anti-phosphorylated tau antibody was detected on AT8 immunostaining (c). Gallyas-Braak silver and anti-human amyloid-β (12B2) staining of the left temporal cortex reveals numerous neurofibrillary tangles and senile plaques (d, e). Severe periventricular white matter rarefaction and ependymal tears (open arrows) were detected on hematoxylin-eosin staining (f).
MRI features
Representative coronal and sagittal 3DT1WI of pDESH and ciNPH patients are presented in Fig. 2. Results of all quantitative, semiquantitative, and qualitative markers are shown in Fig. 3 and Table 3. Compared to the ciNPH patients, pDESH patients revealed lower HPA, higher IHA, IHPA index, and MTA score (114.4±26.2, 392.3±225.0, 3.9±3.0, and 3.8±0.6 versus 151.0±16.4, 213.3±71.4, 1.4±0.5, and 2.4±0.8; p = 0.004, 0.008, 0.001, and 0.002, respectively). On the other hand, no statistical differences were observed in Evans’ index, MRHI, callosal angle, midbrain area, MtP ratio, DESH score, or rate of hummingbird sign between them (p = 0.42, 0.91, 0.13, 0.43, 0.28, 0.70, and 1.0, respectively). In pDESH group, the sole non-neurodegenerative patient with multiple cerebral infarctions showed the highest HPA, second lowest IHA, and lowest IHPA index suggestive of mild hippocampal deformation and temporal horn enlargement.
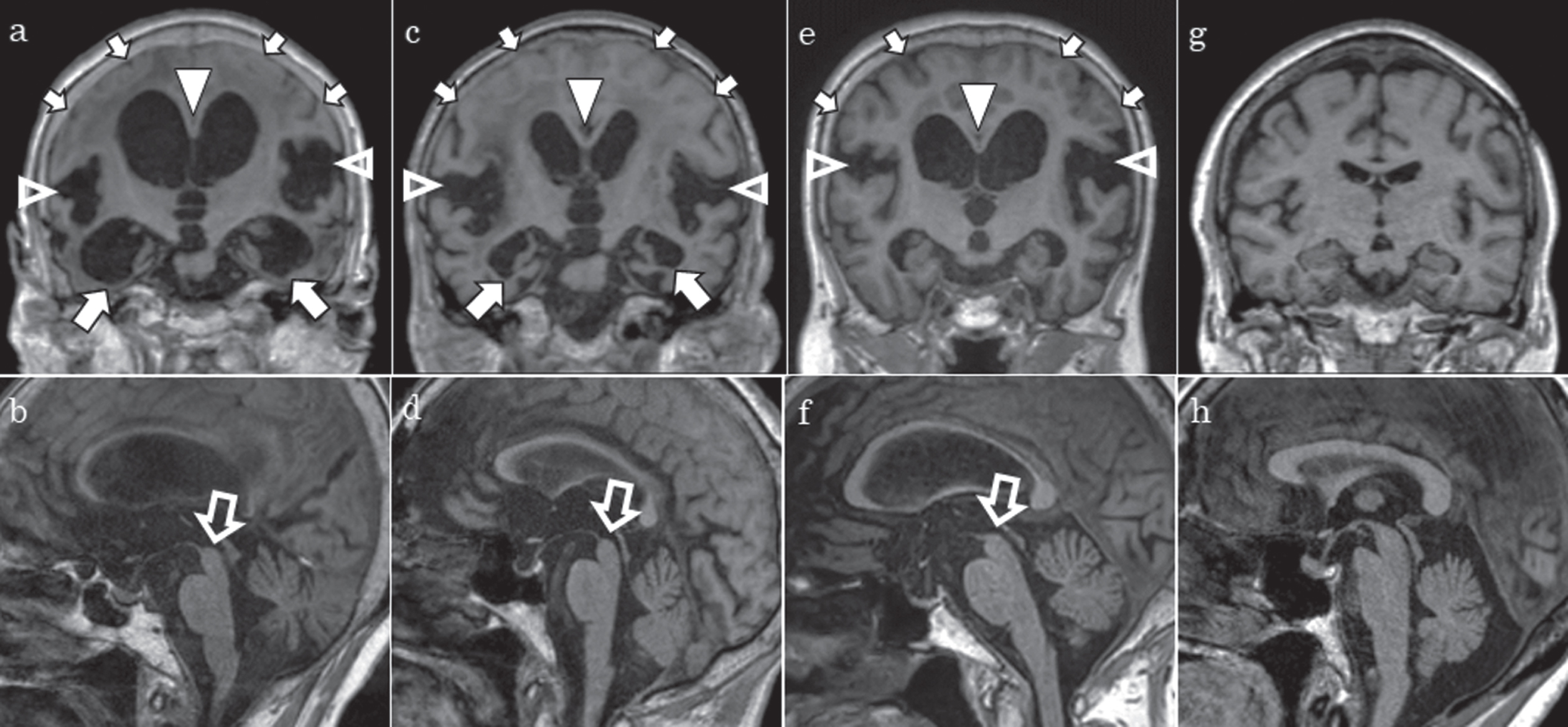
Representative coronal and sagittal 3DT1WI of pDESH, ciNPH, and healthy subjects. a, b) An 81-year-old patient with pathologically-proven AD. c, d) A 91-year-old patient with pathologically-proven AGD. e, f) A 79-year-old patient with clinically-diagnosed iNPH. g, h) A 78-year-old healthy reference. Compared with a clinically-diagnosed iNPH patient and healthy reference (e, g), AD and AGD patients (a, c) showed severe atrophy and long vertical and elliptical deformation of the hippocampus accompanied with marked dilation of the inferior horn (arrows). In contrast to the healthy reference (g, h), other findings including tight high convexity, dilated sylvian fissures, small callosal angle, and midbrain atrophy were almost identical among these patients (a-f; arrowheads and open arrows). 3DT1WI of a healthy elderly subject (g, h) was exhibited as a reference of the above-mentioned neuroradiological findings. AD, Alzheimer’s disease; AGD, argyrophilic grain disease; iNPH, idiopathic normal pressure hydrocephalus
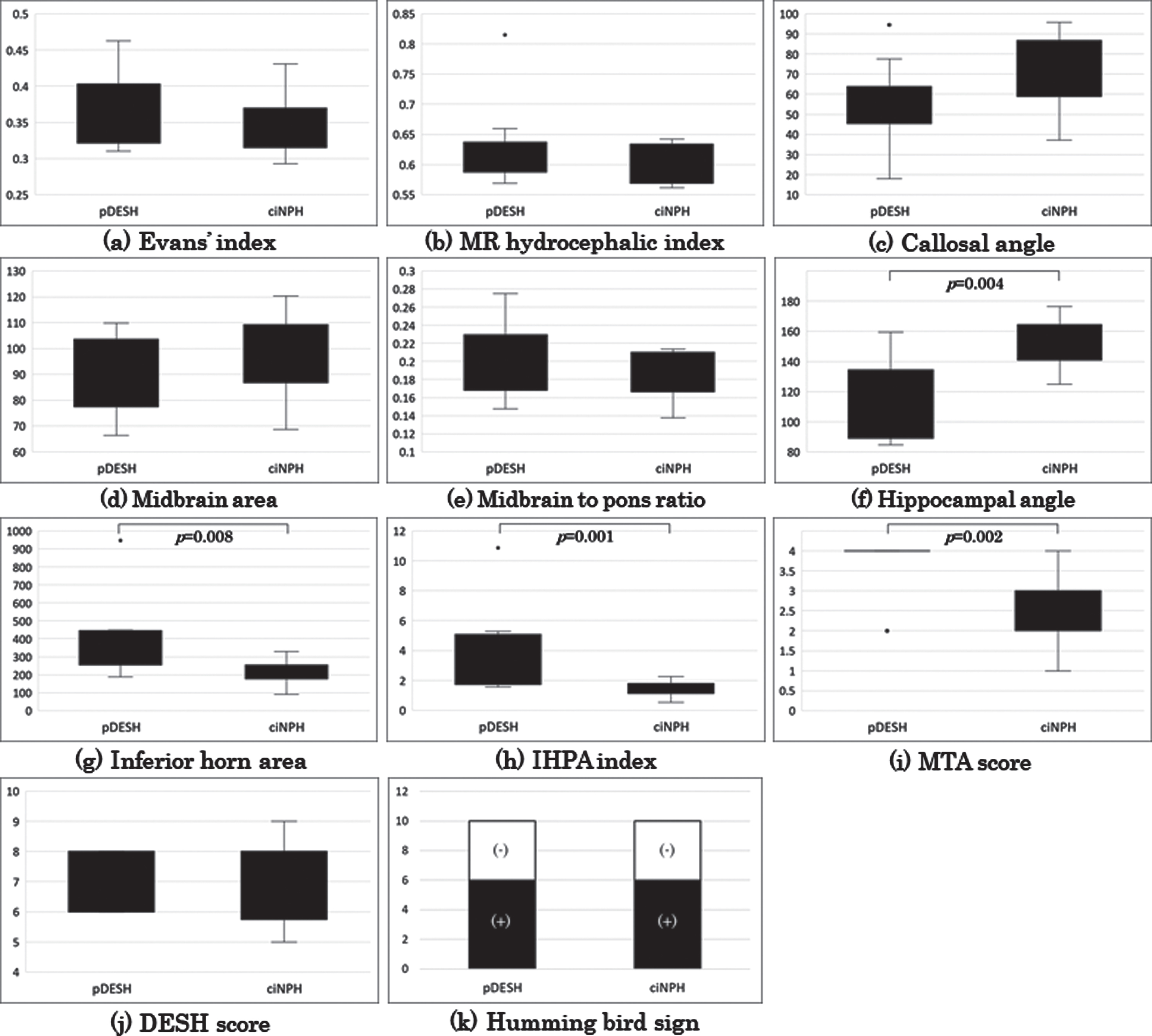
Box plots and stacked column chart of all quantitative, semiquantitative, and qualitative markers. Evans’ index (a), MRHI (b), Callosal angle (c), Midbrain area (d), MtP ratio (e), HPA (f), IHA (g), IHPA index (h), MTA score (i), DESH score (j), Hummingbird sign (k). ciNPH, clinically-diagnosed idiopathic normal pressure hydrocephalus; HPA, hippocampal angle; IHA, inferior horn area; MRHI, magnetic resonance hydrocephalic index; MTA, medial temporal atrophy; pDESH, pathologically-proven patients with disproportionately enlarged subarachnoid-space hydrocephalus
Comparison of quantitative, semiquantitative, and qualitative indices
Data are shown as absolute numbers or the mean±standard deviation. ciNPH, clinically-diagnosed idiopathic normal pressure hydrocephalus; DESH, disproportionately enlarged subarachnoid-space hydrocephalus; HPA, hippocampal angle; IHA, inferior horn area; MRHI, MR hydrocephalic index; MTA, medial temporal atrophy; MtP, midbrain to pons; pDESH, pathologically-proven DESH. *Analysis of covariance adjusted for duration at MRI; †Mann-Whitney U test; ‡Fisher’s exact test; §Cohen’s d, r, and φ were calculated for Welch t-test, Mann-Whitney U test, and Fisher’s exact test, respectively.
DISCUSSION
This is the first study to investigate the neuropathological and neuroradiological findings in pathologically-investigated patients with DESH on antemortem MRI. A new aspect of this study was to compare the MRI findings between pathologically-investigated patients with DESH and clinically-diagnosed iNPH patients. Neuroradiological analyses using quantitative, semiquantitative, and qualitative analyses showed both similarities and differences between pDESH and ciNPH irrespective of iNPH-related symptoms. As expected, in addition to the common features including high DESH score, small callosal angle and midbrain atrophy between pDESH and ciNPH groups, more severe hippocampal atrophy and deformation with temporal horn enlargement (i.e., lower HPA, and higher IHA, IHPA index, and MTA score) was detected in pDESH group. Notably, most of pDESH patients suffered from neurodegenerative diseases including six cases with AD neuropathologies, and no patients suffered from PSP neuropathologies. This result clarifies two implications: 1) significance of medial temporal impairment to detect neurodegenerative pathologies, especially advanced-stage AD in patients with DESH; 2) non-specificity of DESH in patients with neurodegenerative diseases.
Ventriculomegaly with Evans’ index > 0.3, a neuroradiological hallmark of iNPH, is a non-specific finding in elderly patients. In fact, a recent study with large numbers of healthy subjects demonstrated that the upper cut-off level of Evans’ index is higher than 0.3 in the elderly [22]. Therefore, various neuroradiological markers other than ventriculomegaly (e.g., a small callosal angle, dilated sylvian fissures, obliteration of the sulci at the convexity, and aqueductal flow void sign) have been proposed as substitutes [23 , 29]. Against this background, a multicenter prospective study evaluating 100 patients in Japan has validated DESH as a worthwhile MRI finding for the diagnosis of iNPH [1]. Furthermore, the DESH score reflecting the five MRI findings (ventriculomegaly, dilated sylvian fissures, tight high convexity, small callosal angle, and focal sulcal dilation) has been proposed as a useful marker to predict neurological improvement and prognosis after shunt surgery in patients with iNPH [3, 4].
Although DESH is known to be specific and useful to distinguish from atrophy due to AD, DESH-like morphological change has been reported in patients with neurodegenerative pathologies including advanced-stage AD, PSP, and DLB [6 –9]. Additionally, neuropathological changes of AGD and Huntington’s disease were also observed in this study. These results imply that advanced-stage neurodegenerative diseases may show iNPH-like morphological changes, not only ventricular dilation but also small callosal angle, dilated sylvian fissure, and tight high convexity (i.e., DESH). Interestingly, despite the lack of PSP-related neuropathological changes, more than half of patients revealed midbrain atrophy, a neuroradiological hallmark of PSP, in this study. A recent study also clarified the presence of PSP-like midbrain atrophy in patients with DESH and iNPH [12]. Similarly, midbrain atrophy and moderate ventriculomegaly with tight convexity were reported in a patient with pathologically-proven DLB [6]. Direct compression of the superior surface of the rostral midbrain due to an increase of the CSF in the third ventricle seems to cause a morphological change similar to the hummingbird sign [30]. Considering the non-specificity of DESH related findings (i.e., ventriculomegaly, dilated sylvian fissures, tight high convexity, small callosal angle) and midbrain atrophy among patients with iNPH and neurodegenerative diseases, especially PSP, it is important to explore a more specific neuroradiological feature to differentiate these disorders.
For more accurate differentiation between iNPH and neurodegenerative disease, various neuroradiological features have been examined. A recent study advocated MRHI reflecting the largest width of the bilateral collateral trigones of the lateral ventricles divided by the inner skull maximum diameter as being more useful in differentiating PSP from iNPH than the callosal angle or Magnetic Resonance Parkinsonism Index [12]. The different pattern of the ventricular dilatation involving anterior horns rather than collateral trigones in PSP, could contribute to the differentiation between PSP from iNPH patients. However, MRHI was almost equivalent between pDESH and ciNPH in this study. Compared to ciNPH, pDESH patients were more severely demented with longer disease duration. Marked damage of gray and white matter by advanced-stage neurodegenerative pathologies may have resulted in the lateral ventricle dilation with high MRHI being indistinguishable from that of ciNPH. On the other hand, there were statistically significant differences in indices reflecting medial temporal impairment (i.e., HPA, IHA, IHPA index, and MTA score) between pDESH and ciNPH. This result is consistent with the utility of a narrower temporal horn for the diagnosis of iNPH [31]. Because the hippocampus and temporal horn of the lateral ventricle are vulnerable to AD neuropathologic changes, it is reasonable to use these indices for the diagnosis of pDESH, mainly composed of advanced-stage AD [15]. Interestingly, these indices showed abnormal values even in patients with DLB and AGD. This result indicates the possibility of more severe medial temporal impairment in demented patients with comorbidity of DESH and neurodegenerative pathologies other than AD. Considering the chronological volumetric changes of neurodegenerative disease and longer disease duration of pDESH groups, hippocampal atrophy and deformation with temporal horn enlargement can be expected to reflect severely advanced neurodegenerative pathologies [32].
Like that of iNPH, the pathophysiology of DESH is not yet well understood. In this study, specific neuropathological changes other than neurodegenerative pathologies and multiple cerebral infarctions causing ventriculomegaly were not identified. We speculate that some kinds of impaired CSF circulatory comorbidity with ventriculomegaly subsequent to white matter atrophy caused by advanced-stage neurodegenerative pathologies and infarctions may result in a morphological change similar to that of DESH. Recently, iNPH is being considered as not merely a mechanical problem but rather as a reflection of a vicious, self-perpetuating cycle caused by multiple factors including chronically altered CSF dynamics, blood-brain barrier damage, and glymphatic dysfunction [33]. Interestingly, impaired glymphatic function is directly associated with ventriculomegaly, the hallmark lesion of iNPH [34]. Considering the similarity of impaired glymphatic clearance and blood-brain barrier between iNPH and AD, further study to evaluate these structures will also be necessary to understand the pathophysiology of DESH.
The relatively small number of patients is a limitation of this study. Thus, it was difficult to directly compare the neuroradiological features between pDESH patients with neurodegenerative pathologies and those with non-neurodegenerative pathologies. Despite the significant difference in HPA between pDESH and ciNPH patients, the small sample size and non-normal distribution confined the statistical analyses of other indices to eliminate the effect of disease duration. More cases were necessary to remove the effect of confounds on statistical analyses. Additionally, in this study there were no patients with PSP, which was reported to be the most common etiology of iNPH [6]. Taking into consideration the similarities of the clinical and radiological profiles between iNPH and PSP, further study to clarify the differences for the differentiation between pathologically-proven PSP and DESH will be required. Due to the nature of our Brain Bank in a medical long-term care sanatorium, autopsies were performed mainly in long-standing severely demented patients. Thus, it was difficult for us to obtain the neuroradiological data from patients at the early disease stage of pDESH. A prospective long-term observational study evaluating patients with neurodegenerative pathologies will be required to comprehend the clinical and neuroradiological course of pDESH. Despite the clinical diagnosis of iNPH by effective CSF removal tests, neuropathological evaluation was not performed in ciNPH patients. Furthermore, the clinical course of all ciNPH patients after shunt surgeries could not be followed because nearly half of them were transferred to other rehabilitation hospitals and long-term care sanatoriums. So, the possibility of conversion to other clinical diagnoses due to latent neurodegeneration such as mild AD neuropathology was not definitely excluded [35, 36]. Therefore, clinicians should recognize that medial temporal impairment is an imaging marker of advanced-stage neurodegenerative diseases.
In conclusion, morphological changes reflecting DESH can be detected in pathologically-investigated demented patients irrespective of the iNPH-related symptoms. Hippocampal atrophy and deformation with temporal horn enlargement can serve as an imaging marker of neurodegenerative pathologies, mainly AD, in severely demented patients with DESH.