
Abstract
Background:
Although African Americans experience the highest risk of Alzheimer’s disease (AD), they are dramatically underrepresented in preclinical biomarker research. This is especially true for studies involving lumbar puncture as it may involve more perceived risk even for those participants who are otherwise supportive of research.
Objective:
To understand the unique concerns of African American participants regarding biomarker studies involving lumbar puncture who demonstrate support for AD research.
Methods:
Study participants were African American adults contacted through an AD research registry. We employed a novel method used to create hypothetical research studies varying on a set number of factors. The method is designed to collect potential patterns in decision making regarding research participation but differs from experimental vignette design in that the survey is administered with an accompanying qualitive interview to determine the meaning participants ascribe to factors independently and in conjunction with one another.
Results:
Sixty-one participants each reviewed three randomly selected research scenarios and created their “ideal” study involving lumbar puncture. Scenario variables included: disclosure of research results, racial and ethnic identity of the researcher, recruitment method, and amount of incentive.
Conclusion:
Findings indicate that transparency in the return of AD research results to be the strongest driver of participation, followed by race of the researcher and amount of incentive. Recruitment method had limited impact on hypothetical decision making.
INTRODUCTION
Although African American adults experience the highest rates of Alzheimer’s disease (AD), they are paradoxically and dramatically underrepresented in AD longitudinal studies and clinical trials [1–3]. Preclinical AD biomarker research presents additional recruitment and retention challenges as they must recruit and retain younger and non-symptomatic participants and they involve intimidating and invasive biomarker data collection methods such as lumbar puncture (LP) [4]. African American individuals are underrepresented as participants in such studies for a number of potential reasons. Many have offered issues of distrust of science, research, and health professionals as a potential cause [5, 6]. Others suggest that African American participants may feel greater apprehension about procedures such as LP than their White counterparts [7–9]. The disclosure of genetic risk factors and return of research results may also have unique consequences for some as the stigma of dementia may be greater for African American participants [10–12]. Fortunately, we know how to promote inclusive engagement. There is ample evidence of the importance of community located recruitment, incentives, and diversity on the research team [13, 14]. On a deeper level, there has been considerable discussion of principles of honesty, humility, transparency and the maintenance of shared goals with the community in question [15, 16]. Yet, practices to foster these through community engagement are underused in clinical research [17].
To date our efforts are stunted by a framing of the lack of diversity in research as a problem located in communities associated with distrust and unwillingness to participate. Rather, we might view this problem as additionally located within our community of researchers who have placed scant efforts into ensuring that research is accessible and acceptable to a broad range of participants. Representing a shift in focus toward the acknowledgement of discrimination and bias, some researchers have recently suggested that the very execution of clinical trials place barriers to diverse engagement [18–22]. These authors suggest that trials routinely implement practices that privilege, albeit unintentionally, White, well-educated, and resourced individuals such as recruiting among patients at large academic medical centers or using exclusion criteria that needlessly blocks participation. There is also little evidence on the critical factors that make research participation acceptable to various audiences [23–25]. Indeed, many of the studies on the acceptability of research practices, such as the use of broad consent and disclosure of research results are based on samples of largely White participants [26–28].
It is particularly important to understand the acceptability of research practices involving invasive data collection methods, such as LP. The collection of cerebrospinal fluid is crucial to AD research, yet studies involving LP have been shown to be especially unacceptable to those who have low levels of trust in research, such as African American participants [7, 9]. In our own Wisconsin Alzheimer’s Disease Research Center (ADRC), White participants are, indeed, more likely to be willing to undergo an LP. Of 700 participants enrolled in the ADRC Clinical Core and eligible for LP, race is the strongest predictor of participation. One third of African American participants opt for LP, in comparison to 65% of White participants [25]. Even in this sample of individuals motivated to participate in research (as indicated by their enrollment in the Clinical Core), there is difference between White and African American participants in terms of willingness to undergo LP.
For this study, we explored the acceptability of participation in AD research involving LPs among a sample of African American adults aged 40 and older who had existing relationships with AD research as participants in the Clinical Core or participants in the Wisconsin Registry for Alzheimer’s Disease but who had not participated in a research LP.
MATERIALS AND METHODS
We used a StoryDeck methodology designed to isolate the most salient factors effecting the decision to participate in LPs. Like an experimental vignette design, the StoryDeck is used to create hypothetical research study scenarios that vary on a set number of factors. Through participant judgement of hypothetical studies, we are able determine factors that not only contribute but drive decision making highlighting critical points of acceptability. Unlike the experimental vignette design, the StoryDeck is administered with an accompanying qualitive interview to determine the meaning participants ascribe to factors independently and in conjunction with one another. In this study, participants were asked to respond to three randomly generated, hypothetical research studies that varied on four factors each containing three possible variations using the StoryDeck administered through an interview. All scenarios involved biomarker data collection through LP. Variable factors were recruitment method (physician’s office, community event, close friend or family member recommendation) level of disclosure of research results (full, partial, no disclosure) incentive amount ($0, $100, $250) and the racial or ethnic identity of the researcher (African American, White, Native American). While each participant saw each factor among their three scenarios, the groupings varied. For example, one participant might have seen a scenario with a physician champion and an African American researcher. Another might have a physician champion matched with a White researcher. Scenarios were generally randomly generated. However, once a factor appeared in a scenario, it dropped out of the pool of factors to be used to create subsequent scenarios. In this way, each participant had experience with each possible factor. After the interviewer read each scenario, participants were asked about the likeliness of their participation in each presented study (definitely would, possibly would, maybe, probably not, not in a million years) (see Fig. 1). Finally, following the three randomly generated scenarios, participants were then presented with all possible variations of each factor to choose their “best possible” or ideal research study involving LP (see Fig. 2). In total, each participant reviewed three generated scenarios and created one of their own using the established pool of factors. Study procedures were approved by the University of Wisconsin Institutional Review Board #2020-1498.
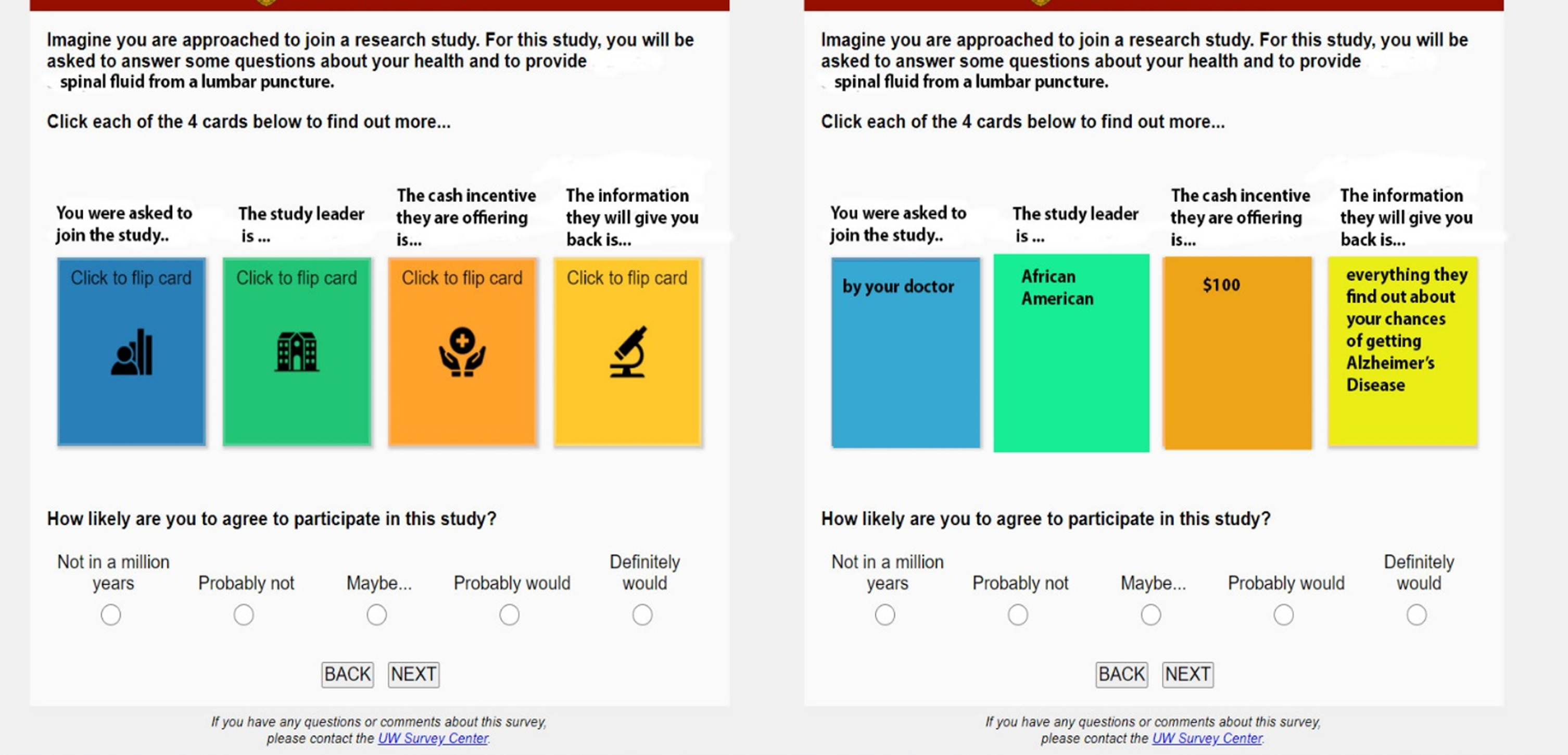
Screen shot of data collection instrument - random scenarios.
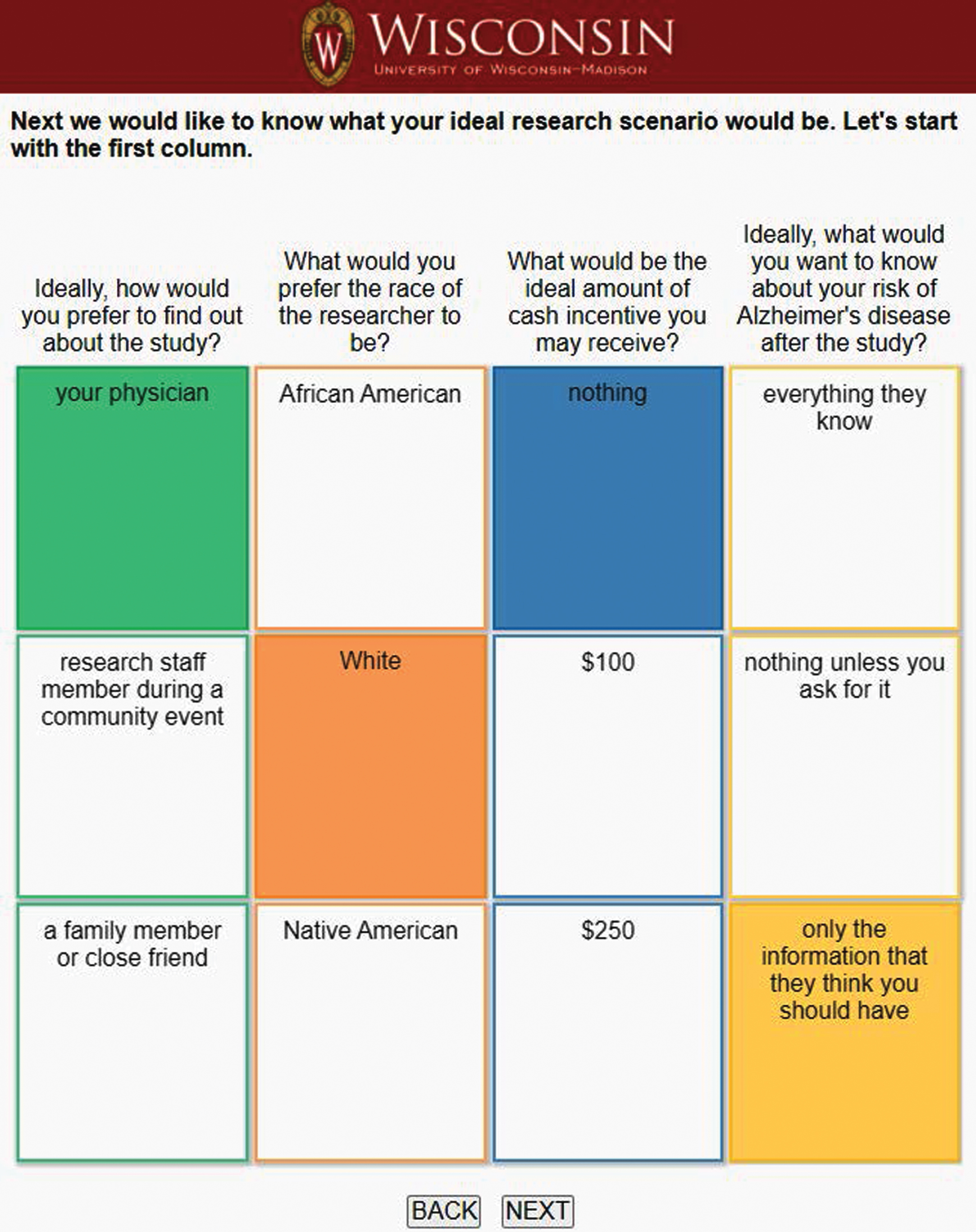
Screen shot of data collection instrument - ideal scenarios.
Rationale for factor selection
Variable factors for scenarios were limited to four. We have found in previous studies that having too many factors, while perhaps beneficial in that it produces more data, quickly becomes confusing and tedious to participants and have settled on four factors in the past [29]. In general, this is a limitation of the StoryDeck methodology that we believe is balanced by the rich data the method provides on the factors chosen. For this study each factor represented in scenarios connects to an existing body of literature on willingness to participate in research. However, previous studies have not been able to show the relative importance of factors for decision making, an advantage of the StoryDeck. Each factor selected for this study is detailed below.
Recruitment method: This factor has been tied to willingness to participate in research by a number studies [14, 28]. Overall, community-based, and word-of-mouth approaches have been found successful for recruitment of underrepresented groups.
Disclosure of research results: There has been much discussion of the ethics of blinded versus transparent biomarker research [30–33] and some regarding disclosure of results as a barrier to participation [28].
Amount of incentive: While common practice across the research enterprise, the use of financial incentives has not received a great deal of systematic study with a few exceptions [34, 35]. In practice, researchers try to offer financial incentives large enough to motivate participants to join the study but not so large as to be coercive.
Race of the researcher: Racial or ethnic concordance is another motivator for African American participants to engage in research that is strongly supported [13, 37].
Of course, there are many other factors that might have been included in scenarios such as institution (hospital or university), existing connection to study team members or form of consent (broad, tiered or study specific). Two of these have been used in previous studies with other groups of African American participants [29] (Passmore et al., unpublished data). In each, institution has been shown to have an interesting but limited impact on decision making. Conversely, the issue of form of consent has been shown to have a strong impact on participant decision making. Each of these were purposely excluded in this study so that we could add to knowledge on the factors that were included. Race of the researcher was included as previous findings were somewhat inconclusive about the meaning of the race of the individual researcher and diversity on the study team.
While we have used physical cards in previous versions of the StoryDeck, we created a virtual deck for this study to afford the ability to conduct remote data collection during the pandemic. Our team created a draft instrument working with the University of Wisconsin Survey Center. It was then presented to the community advisory board (CAB) maintained by the Wisconsin Alzheimer’s Institute, Milwaukee office. CAB members provided feedback on factors, scenario length and language accessibility. The instrument was refined based on this feedback before data collection began.
Sample
As noted, our sample was comprised of individuals with an existing connection to the University of Wisconsin Madison Alzheimer’s Disease Research Center (UW ADRC) or the Wisconsin Registry for Alzheimer’s Prevention (WRAP). Participants were reached in a few ways. Initially, members of the research team attended center events (e.g., health fairs) to distribute flyers and raise awareness of the study. Potential participants were contacted through existing lists of enrolled participants in the WRAP study or the ADRC Clinical Core. Participants were eligible if they identified as African American, were 40 years of age or older, and had not participated in LP for research purposes. We were interested in exploring hesitancy to participate in LP among this group to attempt to understand why among a pool of individuals inclined to engage in AD research, African American participants refused LP significantly more frequently than their White counterparts [25].
Data collection
When participants indicated interest, an interview with a team member was scheduled. Due to public health restrictions related to COVID-19, interviews were conducted via zoom. The interviewer shared their screen to use the online version of the StoryDeck to guide discussion (see Figs. 1 and 2). Interviews were conducted by graduate students who self-identify as people of color and were audio recorded (not video recorded). During interviews, participants were shown three randomly generated research scenarios using the virtual StoryDeck. After the interviewer read the scenario, participants were asked about the likeliness of their participation in each presented study (definitely would, possibly would, maybe, probably not, not in a million years). They were further asked to explain their reasoning and decision-making process with reference to each characteristic. In these semi-structured interviews, questions varied based on the participant’s decision. For example, if a participant chose that they “definitely would not” participate in the relevant scenario, the interviewer would first inquire about what led them to that decision. They would follow that with probes regarding each factor in the scenario (i.e., “Did the fact that you found out about this study from a physician influence your decision? How so?). After participants fully explained their decision relative to each factor, they were probed about factor interactions (i.e., did it matter that that the researcher was White? Would it have been different if they had been African American?), although much of this also emerged in the initial discussion of the scenario. This process was repeated for each of the three random scenarios. Finally, participants were presented with the screen from which they were asked to create their “ideal” study involving LP (see Fig. 2). If a participant found no studies involving LP to be acceptable, they were asked to create the research scenario that came closest. Once they completed that task, they were asked to explain their decision making in the same manner as they were regarding randomly generated scenarios.
Analysis: Quantitative
In the randomized StoryDeck portion of the survey, the experiment was designed such that each participant saw each unique level of each factor exactly once, hence, each participant had three recorded measurements. No condition was imposed regarding which factor levels were shown in conjunction with other variables, that is, the randomization between the factors was independent. To assess how the experimental factors (recruitment method, return of research results, incentive, and researcher race) affected the participants likelihood of study participation (an ordinal variable), a mixed-effects ordinal regression model was fit to the data using the ‘ordinal’ package in R (V 4.2.2) using a logistic link function [38]. The experimental factors were modeled as main, fixed effects, while the effect of study participant was modeled as a random effect to account for the heterogeneity induced via the repeated measurements design. The proportional odds assumption of the model was found not to be violated (p > 0.05 for each factor).
Analysis: Qualitative
Interviews were audio recorded and professionally transcribed. We completed analysis on the process of participant decision making guided by an iterative coding of the transcripts facilitated by the use of Nvivo software for data management [39]. Two members of our team performed qualitative analysis with one functioning as the primary coder. Following a period of immersion in the data set, some initial codes were identified. Coding took place in two phases. Our initial pass included the preliminary codes, initial coding relative to scenario factors, and conscious open coding to label and identify emergent categories. This phase was followed by axial coding which aimed to identify connections across and between categories [40, 41]. This process revealed a set of thematic codes. Coders met weekly to develop/define emergent codes, clarify concepts and resolve discrepancies in coding. Feedback was also routinely sought from the larger study team. Interpretation of qualitative findings and connections between codes were also team based. The reader should note that the quotations found in the results section were chosen based on their ability to clearly convey themes or concepts. They are not the totality of quotations for any theme or concept.
RESULTS
Quantitative
Table 1 presents participant characteristics of our sample (n = 61). The majority were African American women who had experience with AD. Most had college education and a quarter had gone on to graduate school.
Participant characteristics (n = 61)
The contingency tables between each factor level and observed response totals for the randomized StoryDeck portion of the project can be seen in Tables 2 and 3.
Counts of report likelihood scores for each level of the experimental race and information factor*
*In example, a hypothetical scenario with a Black MD received a ‘probably’ score (in terms of perceived participation) 19 times across the study.
Counts of report likelihood scores for each level of the experimental financial incentive and resource factor*
*In example, a hypothetical scenario with a $0 incentive received a ‘definitely’ score (in terms of perceived participation) 3 times across the study.
As a whole, participants found 36% of reviewed scenarios acceptable (definitely would, possibly would participate). Only five participants rejected all scenario variations or stated slightly differently, 92% of participants found at least one research scenario involving LP to be acceptable. Those few participants who rejected all scenarios frequently reported fear of needles or pain.
In addition to judging random scenarios, each participant created their “best possible” or ideal” research scenario. Figure 3 presents the results of “ideal” research scenarios created by participants and illustrates the relative importance of each factor in participant decision making. Participants preferred research studies lead by African American researchers, in which they would receive the highest incentive and full disclosure of research results. To a lesser extent, participants preferred studies recruiting through a physician’s office rather than in at community events.
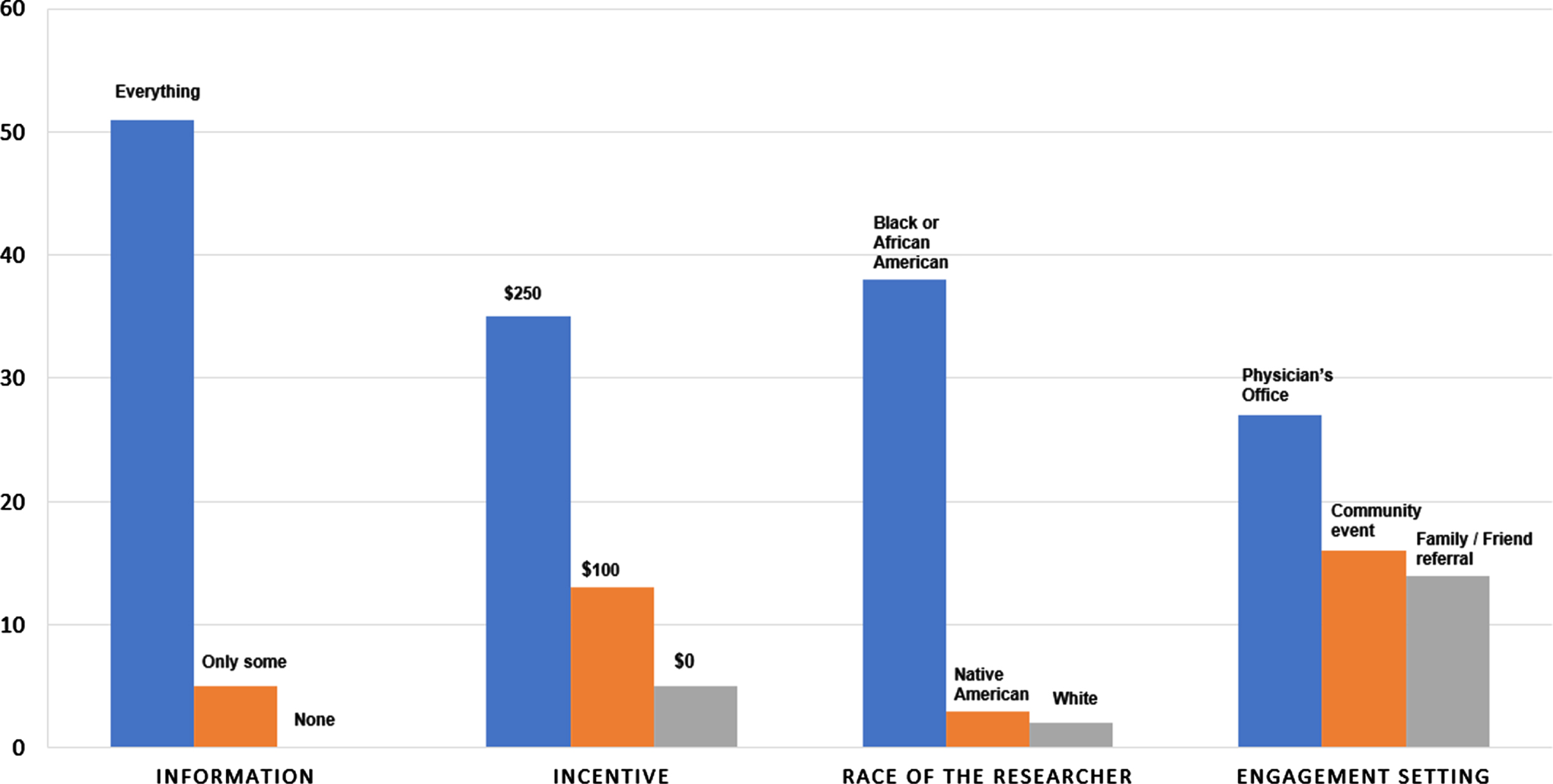
Number of “ideal” research scenarios where characteristic appeared.
These findings are confirmed in the analysis of the random scenarios. From the preliminary model fit to the data, the return of research results was the most significant experimental factor under study (p < 0.0001) using a likelihood ratio test (LRT). Compared with offering prospective participants no research results, offering them only partial disclosure did not significantly increase the odds of being in a higher participation category (OR = 1.37, 95% CI = (0.66, 2.85), p > 0.05) however offering patients all research results did substantially increase the odds of participation (OR = 12.87, 95% CI = (5.37, 30.83), p < 0.0001).
The amount of financial incentive was also significantly related to the likelihood of study participation (LRT, p = 0.002). Compared with no financial incentive ($0), the odds of participation were higher when participants were offered $100 (OR = 2.57, 95% CI = (1.18, 5.58), p < 0.05) and even higher when participants were offered $250 (OR = 4.2, 95% CI = (1.86, 9.46), p < 0.001). The overall effect of researcher race was also significantly related to study participant likelihood (LRT p < 0.01). The model indicated that switching from an African American researcher to a Native American researcher did not significantly affect the odds of participation (OR = 0.60, 95% CI = (0.29, 1.23), p > 0.05), but a White researcher significantly decreased the likelihood of participation compared with an African American researcher (OR = 0.34, 95% CI = (0.03, 0.19), p < 0.01). Finally, the overall effect of recruitment method was not significantly associated with participation (LRT p > 0.05) (see Table 4).
Fixed effects portion of model summary from the mixed-effects ordinal regression, showing the estimated odds ratio (OR), the 95% confidence interval for the OR and Wald-type p-values
Qualitative
Qualitative analysis also confirmed the importance of the return of research results in participant decision making. Initially, many participants perceived information as a direct benefit for research participation and as a way to potentially improve their health or the health of their families. For example,
“... having all the information is helpful because you know how to, how you should look at your family history. You know, did it start before, did it start now, will it start later, will it affect my grandkids? So I’d like to know everything, so you know what to tell people.” (57-year-old woman, Ideal Scenario: African American researcher; full disclosure; community event recruitment; $250 incentive)
In addition and, perhaps on a deeper level, being provided with all information was also symbolic of transparency, a characteristic that is indicative of trustworthiness [13, 16], for several participants like this 49-year-old man,
“No. I mean, if they tell me everything that they knew about the research, I mean, that would push me more so of really wanting to go forward with it because a person is being transparent. So that would, really, you know, let me know that you’re not trying to hide anything.” (Ideal Scenario: African American researcher; full disclosure; community event recruitment; $250 incentive)
While the participant quoted above noted the attribution of transparency in a positive sense with full disclosure, most participants expressed this same phenomenon negatively in response to scenarios without the return of research results. Thus, withholding information was seen as suspect reflecting a power imbalance and something that generally in the words of one participant “sort of discredits them.” Several participants also expressed suspicion around “holding back information.” Some examples are presented below.
“You know, ... I would say the main factor that keeps me concerned is about the information, the sharing the information. If it feels like they’re holding back information, then that’s what’s kind of keeping me at bay.” (65-year-old woman, Ideal Scenario: African American researcher; full disclosure; close friend/family recruitment; $100 incentive).
“Because if they find something, why not tell me, you know? Why would you hold that back from me? (65-year-old woman, Ideal Scenario: African American researcher; full disclosure; physician recruitment; $250 incentive)
“... so that makes me skeptical, and so I’d probably, I don’t know... ” (40-year-old woman, Ideal Scenario: African American researcher; full disclosure; no preferred recruitment method; $100 incentive)
“... saying nothing unless you ask for it, it’s kind of like holding stuff back and that would make a person question, you know, the whole research thing, so... ” (62-year-old woman, Ideal Scenario: African American researcher; full disclosure; close friend/family recruitment; $250 incentive)
Incentives
Most participants preferred the highest offered incentive ($250) which also confirmed the findings of our quantitative analysis. Participants saw incentives as rightful compensation for their time and effort. They did not, however, frequently frame the inclusion of the highest incentive in ideal scenarios as a strong motivator for participation. For example,
“... if you’re going to like take up my time and stab my body like that’s not going to be nothing.” (44-year-old woman, Ideal Scenario: African American researcher; full disclosure; physician recruitment; $100 incentive)
It is also interesting to note that participants framed both the incentive and the return of information as “benefits” of participation. In response to a scenario with only the possibility of information and no dollar incentive
“Well, it says your information they give you is limited, and you don’t get nothing for doing the study. Well, that’s why ... I don’t want to do the study, and then I don’t get nothing, and then they don’t give me no information either.” (61-year-old man, Ideal Scenario: African American researcher; full disclosure; close friend/family recruitment; $250 incentive)
Race of the researcher
Fewer participants than expected, given the strong quantitative findings in both random and ideal scenarios, reported that race of the researcher influenced their judgement of acceptable scenarios. Some verbalized sentiments interpreting the race of the researcher as “not important” or not something “that matters.” However, those participants who did indicate that they preferred African American researchers noted that they would be more relatable, understanding, and trustworthy. The following participant quotes illustrates this sentiment.
“I would probably prefer if it was an African American researcher because I would hope that the researcher would be sensitive to the way that African Americans have been used as guinea pigs in the past, and that for that reason, they might be more ethical in going about their study and more sensitive to, you know, to our past in that respect.” (62-year-old woman, Ideal Scenario: African American researcher; full disclosure; community event recruitment; $250incentive)
And,
“I mean, I want to say that it doesn’t matter, but we know that it does, right? And so I think that having a researcher of color makes me feel a little bit more comfortable. It makes me feel more confident that my concerns are going to be addressed, and that my, that I’m going to be, you know, a little bit more cared for. So, you know, I don’t think it’s like a super strong preference. I think some of, I think, honestly, the thing in the last box, to me, the yellow, is what matters the most. But there is kind of a bonus to having a researcher that looks like me, you know.” (62-year-old woman, Ideal Scenario: African American researcher; full disclosure; no preferred recruitment method; $100 incentive)
By the same token, while some participants saw a Native American researcher as preferable as a person of color, participants still saw African American researchers as preferable overall.
“Just in these last two years with my sister, two sisters having Alzheimer’s, I just don’t think it’s the same between African Americans and another race ... I’d rather be with somebody who would, you know, explain it to me in my community or within the same race as I am.” (58-year-old woman, Ideal Scenario: African American researcher; full disclosure; community event recruitment; $250)
Recruitment encounter
Participants expressed a slight preference for a recruitment encounter with a physician in interviews. For example,
“My doctor knows my history, and so does my family member. But my doctor might see something in me or in my medical, personal medical history that he might, you know, recommend it for me.” (66-year-old man, Ideal Scenario: African American researcher; full disclosure; physician recruitment; $0 incentive)
And,
“Professionalism, you know. You know, the respectability that you get. I mean, you know, as a certified physician, you just ... trust comes easier.” (54-year-old man, Ideal Scenario: African American researcher; full disclosure; physician recruitment; no incentive)
In contrast, family and friends were trusted to have good intentions but were not necessarily seen to have the necessary competence to correctly judge the value or safety of the research opportunity.
“... I would rather hear it from a physician, someone that is, knows more in the medical field. A family member or a close friend, unless they’re a doctor, no.” (72-year-old woman, Ideal Scenario: African American researcher; full disclosure; physician recruitment; $100 incentive)
Recruitment at community events was also frequently determined to be less than desirable and some participants linked this to a lack of personal connection as did the man quoted below.
“And then I’m just meeting them at a community event that I may or may not trust, yeah, would send even more red flags up to me.” (55-year-old man, Ideal Scenario: African American researcher; full disclosure; physician recruitment; $250 incentive)
DISCUSSION
Overall, our findings are encouraging as almost all participants were able to identify at least one research study scenario involving LP in which they would be willing to participate. We also confirm the importance of several factors in the decision to participate in research involving LP. While each of the factors included in scenarios (race of the researcher, incentive, return of research results, and recruitment method) are represented in the existing literature, our data offers a higher level of specificity that may be helpful for researchers interested in how participants, even those favorably inclined to engage in research, may value studies involving invasive biomarker data collection, like LP. We find that the most significant driver of decision making for our participants is, both qualitatively and quantitatively, the return of research results. However, we would not argue that researchers should simply return “all information” gained through research as our participants indicate. This is a complex issue that was simplified in our scenarios. As noted by ethicists, researchers may gather information that is misleading, medically unimportant or unactionable which may be potentially damaging to participants [42, 43]. Thus, disclosure of research results in practice must balance the principle of beneficence and respect for participant autonomy [44]. The lesson that our participants have to teach us is not about a desire for total disclosure of results despite the potential for harm. Instead, our study points to 1) the importance of research results as a key form of reciprocity in biomarker research participation for our participants and 2) the strongly charged nature of non-disclosure for communities experiencing historical and current marginalization. Indeed, the former point is a critical lesson with implications for all research. Participants repeatedly and strongly express a preference of research transparency. Further, our African American participants clearly expressed concerns about being kept in the dark by researchers. They find the lack or limitation of disclosure to be indictive of what might be called “untrustworthiness” and what participants referred to as “hiding” or “holding back” information, potentially paramount to making the hypothetical participant a “guinea pig.” As such, we conclude, as have many others, that transparency is a fundamental feature of trustworthiness and a prerequisite for inclusive research [45, 46]. Our more unique contribution is that disclosure was not only a preference of our participants but a driver of decision-making. What our data cannot tell us is the extent to which transparency can include a clear explanation of why some results are not returned, especially in contexts where there may be legitimate reasons to not return results. This would be an interesting follow-up to the current study.
Secondarily, the presence of a Black or African American researcher was shown to add a measure of “trustworthiness” and comfort to study scenarios even when the incentive was low or when information sharing was limited. This was demonstrated in the StoryDeck quantitative and qualitative results. Other studies support this finding of race of the researcher as a motivator for research participation [13, 36]. The lack of diversity in science is thus perhaps tied to the lack of diversity in research participation in multiple ways. Research, its design and conduction, is representative of culture and cultural values that are “read” by potential participants and considered in the decision to participate in research [13]. Researchers, especially White researchers and predominantly White research teams should consider how they represent their research to prospective participants with the knowledge that many elements of the offer to participate in research may be interpreted as indications of untrustworthiness. Indeed, given the history of research abuse perpetrated against vulnerable populations [47] and ongoing contexts of discrimination in health care settings [48] expecting the creation of trust without transparency is, understandably, impractical.
Limitations
There were several limitations to this study. Some of these relate to the StoryDeck methodology which can only be used with a limited number of variable factors. This limits our exploration of decision making. Moreover, the StoryDeck, especially when using a web-based data collection method, requires a simplification of factors which results in a loss of nuance. For example, the disclosure of research results is much simplified in our data collection and does not reflect complex issues of process or ethics. We believe that the benefits of the methodology such as the ability to identify drivers of decision making and to dive deeply into the meaning of the chosen factors outweigh some of these limitations. Nonetheless, we would also like to see future studies that address other factors influencing decision making regarding LP studies. In addition, our sample was somewhat skewed toward college-age women. The reader may be interested in a previous study using the StoryDeck with a majority male sample which includes a similar discussion of related issues [29]. Finally, we have reason to believe that social desirability effects influenced our data, particularly with regard to incentives and race of the researcher. Such effects are difficult to avoid although we hope that we have minimized some, at least around race of the researcher, by having racially concordant interviewers.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the Wisconsin Alzheimer’s Institute and University of Wisconsin, Center for Community and Nonprofit Studies for support of participant recruitment and data collection.
FUNDING
The project was supported by a supplement of the Wisconsin Alzheimer’s Disease Research Center (ADRC) award from the National Institute on Aging (P30-AG062715). We acknowledge that the intellectual and technical contributions of Colin Longhurst of the Biostatistics and Epidemiology Research Design Core were also supported by the ADRC. This work also received support from the University of Wisconsin, Institute for Clinical and Translational Research (NCATS: UL1 TR002373). The StoryDeck methodology was refined with support from the National Human Genome Research Institute (R21 MD015130).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.