
Abstract
Background
Peritonitis is a major cause of morbidity, mortality, and technique failure in peritoneal dialysis (PD) patients, especially when caused by enteric microorganisms (EM). We have implemented a treatment protocol specifically aimed at improving the outcome in EM peritonitis. The adapted protocol was applied in all PD patients 50 years and older presenting with peritonitis who were considered to be at risk of EM peritonitis and involves 3 interventions: 1) temporary discontinuation of PD without removing the catheter (peritoneal rest), 2) intravenous meropenem, and 3) meropenem intracatheter as lock (Mero-PerRest protocol).
Methods
In this observational study, we compared the outcome of 203 peritonitis episodes in 71 patients treated with the Mero-PerRest protocol, with 217 episodes in 104 patients treated with a more traditional intraperitoneal gentamicin-rifampicin-based regimen.
Results
In EM peritonitis episodes, the Mero-PerRest protocol resulted in a higher primary cure rate (90.0% vs 65.3%, adjusted odds ratio [OR] 4.54 [95% confidence interval (CI) 1.46 – 14.15]) and better technique survival (90.0% vs 69.4%, adjusted OR 3.41 [95% CI 1.07 – 10.87]). This effect was most distinct in patients with polymicrobial EM peritonitis (cure rate 87.5% vs 34.8%, p = 0.0003). Interestingly, primary cure rate (95.6% vs 84.7%, adjusted OR 3.92 [95% CI 1.37 – 11.19]) and technique survival (95.6% vs 85.6%, adjusted OR 3.60 [95% CI 1.25 – 10.32]) were also excellent in non-EM peritonitis episodes. Patient survival did not differ significantly.
Conclusion
The poor outcome of peritonitis caused by EM in PD patients aged 50 years and older could be improved by applying a treatment protocol involving temporary discontinuation of PD without catheter removal and intravenous and intracatheter meropenem.
Keywords
More than a decade ago, a cluster of EM peritonitis episodes with poor outcomes prompted the PD unit of the University Medical Center Utrecht (UMCU) to adapt its peritonitis treatment protocol. This adaptation was based on the assumption that EM peritonitis is most often related to (micro)perforations of colonic diverticula that fail to seal while continuing PD. It was also hypothesized that the favorable effect of PD-catheter removal in EM peritonitis is not caused by the removal itself, but by the ensuing peritoneal rest, allowing peritoneal defenses to seal these perforations. Furthermore, identification of patients at risk of EM peritonitis, permitting timely institution of adequate antimicrobial therapy, was assumed to be essential. As the prevalence of diverticular disease of the colon increases with age (8,9), elderly patients were considered to be at risk of EM peritonitis and were subjected to the adapted protocol.
According to the new protocol, all patients ≥ 50 years interrupted PD and received intravenous (IV) meropenem and a meropenem catheter lock at presentation with peritonitis. This strategy was continued for 1 week in cases of EM peritonitis, without removing the PD catheter. In cases of non-EM peritonitis, PD was resumed with appropriate intraperitoneal (IP) antibiotics when culture results became available. In the present study, we compared peritonitis outcomes in the UMCU with those of contemporary peritonitis episodes in PD patients ≥ 50 years treated at the VU University Medical Center (VUmc) Amsterdam that applies a traditional peritonitis treatment protocol using empirical IP antibiotics in all patients.
Methods
Study Populations
We analyzed all non-relapse peritonitis episodes in PD patients ≥ 50 years old in the UMCU and VUmc between 1 January 1998 and 31 December 2008.
Data Collection
In the UMCU, all peritonitis episodes were collected prospectively in a database. In the VUmc, all results of abdominal fluid cultures in adults obtained during the study period were acquired by an automated search of the electronic database of the Department of Medical Microbiology. Before further analysis, patients were assessed to determine whether they were indeed suffering from a PD-related peritonitis at the time of the culture.
Data collected were patient characteristics, start date of PD, PD modality, start date of the episode, initial leukocyte count in PD effluent, initial treatment, culture results, and outcome of peritonitis episode (i.e. primary cure, relapse, PD-catheter removal or exchange, transfer to hemodialysis [HD], or death).
Definitions
Peritonitis was defined according to the criteria of the International Society for Peritoneal Dialysis (ISPD) (7).
Enteric microorganisms were defined as pathogens commonly found in the gut, including Enterobacteriaceae, enterococci, and anaerobic bacteria. All other pathogens were classified as non-enteric (non-EM).
Patients with ≥ 2 cultured pathogens were considered to have polymicrobial peritonitis.
Primary cure was defined as resolution of a peritonitis episode with antibiotic treatment alone.
Relapses were defined as peritonitis with either the same organism or a negative culture occurring within 4 weeks of completion of therapy of a prior (culture-positive) episode. A relapse was not counted as a separate episode of peritonitis; its outcome was allocated to the initial episode.
Technique survival was defined as the proportion of patients who stayed on PD after resolution of the peritonitis episode.
Death was attributed to peritonitis if it occurred within 30 days after presentation or was attributable directly to peritonitis.
Adapted Umcu Treatment Protocol (Mero-Perrest Protocol)
In the UMCU, PD was stopped without removing the catheter in patients ≥ 50 years old presenting with peritonitis. They were treated with meropenem IV (500 mg/day) (10) and meropenem instilled once daily into the PD catheter (125 mg in 25 mL of saline). If cultures showed EM, PD was discontinued for 1 week with continuation of IV meropenem and as lock. If clinically indicated (i.e. hyperkalemia, uremia-related symptoms, or volume overload), patients were temporarily treated with HD. After 1 week, PD was resumed and meropenem was administered IP (125 mg/L dialysate in all exchanges) for another week. Predefined deviations from the protocol included an already identified non-EM, a concomitant exit-site infection suspected to be the cause of peritonitis, and meropenem allergy. In case of culture of a microorganism resistant to meropenem, an appropriate antibiotic could be added to the regimen. Episodes in which Candida species were cultured were treated using a protocol reported elsewhere (11).
If cultures indicated non-EM, meropenem was discontinued and PD was resumed with IP antibiotics adapted to culture results for 2 weeks. In cases of culture-negative peritonitis, PD was resumed with IP cephalothin.
Peritoneal dialysis-catheter removal was performed as indicated by the ISPD guidelines (7).
To prevent fungal peritonitis, all patients were treated with oral fluconazole (50 mg/day) during antibiotic treatment for PD-related peritonitis.
To prevent exit-site infections and peritonitis with S. aureus, all patients routinely applied mupirocin at both the exit site and intranasally daily.
Vumc Treatment Protocol (Traditional Protocol)
In the VUmc, the standard antibiotic treatment for PD-related peritonitis was combined IP gentamicin (20 mg/L dialysis fluid in the first exchange and thereafter once daily in the long dwell) and rifampicin (50 mg/L in all exchanges). A different treatment was chosen in case of a known allergy or when culture results of a recent peritonitis episode or exit-site infection had required different antibiotics. Also, patients could be treated with IV antibiotics if systemic infection was suspected. From October 1996 to October 1999, patients were also treated according to the protocol of the CIPPER trial, comparing IP ciprofloxacin-rifampicin with IP cephradine (12). Subsequent antibiotic treatment was adapted based on culture results and clinical response. Antibiotic treatment was continued until 1 week after the PD effluent leukocyte count dropped below 0.1 x 109/L (minimum of 2 weeks, 3 weeks in S. aureus peritonitis). Peritoneal dialysis-catheter removal was performed as indicated by the ISPD guidelines (7).
No antifungal prophylaxis was given in the VUmc during episodes of peritonitis.
Intranasal mupirocin was used intermittently in S. aureus nasal carriers.
Statistical Analysis
All statistical analyses were performed with SPSS 20.0 and GraphPad Prism 5.01 (SPSS, Chicago, IL, USA; GraphPad Software, Inc., CA, USA).
For the analysis of peritonitis-episode outcomes we compared primary cure rate, relapse rate, catheter removal rate, need for temporary or permanent HD, technique survival, and patient survival using both strategies. Because the Mero-PerRest protocol was specifically designed to improve the outcome of EM peritonitis, our main analysis was the on-treatment analysis of EM peritonitis episodes. In addition, we also performed an on-treatment analysis of non-EM peritonitis episodes. Finally, to evaluate the efficacy and safety of the Mero-PerRest protocol in general, we performed an intention-to-treat analysis of all peritonitis episodes in PD patients ≥ 50 years old.
For the analysis of patient outcome, we compared patient survival, technique survival, catheter intervention rate (i.e. removal or exchange), and HD transfer rate on an intention-to-treat basis. For this, we divided patients developing peritonitis into those experiencing at least 1 EM peritonitis episode (EM peritonitis-prone patients) and those that never experienced such an episode (non-EM peritonitis-prone patients).
Continuous data are expressed as mean ± SD. Differences between centers were analyzed by Student's t-tests. Dichotomous data were analyzed with Fisher's exact test.
Differences in primary cure rate, technique survival, and patient survival of peritonitis episodes adjusted for confounders were analyzed using logistic generalized estimating equations (GEE), a technique suitable for longitudinal data analysis between a continuous variable and several time-dependent and time-independent covariates (15). Generalized estimating equations adjust for clustering of measurement results at the patient level. In the analyses of these outcome measures, the dichotomous variable “center” was the determinant. Next to the crude model, we constructed an adjusted model with age, gender, and PD duration as confounders. Age and PD duration were added as continuous variables, gender as a categorical.
P-values < 0.05 were considered to be statistically significant (2-tailed).
Results
Patient and Peritonitis Episode Characteristics
During the study period, 420 non-relapse peritonitis episodes in patients ≥ 50 years old were available for analysis: 203 in the UMCU in 71 individuals and 217 episodes in 104 individuals in the VUmc (Figure 1). Patient and peritonitis episode characteristics are summarized in Table 1. The Mero-PerRest protocol was applied in 163 episodes (80.3%); the gentamicin-rifampicin protocol in 160 episodes (73.7%).
Patient and Peritonitis Episode Characteristics
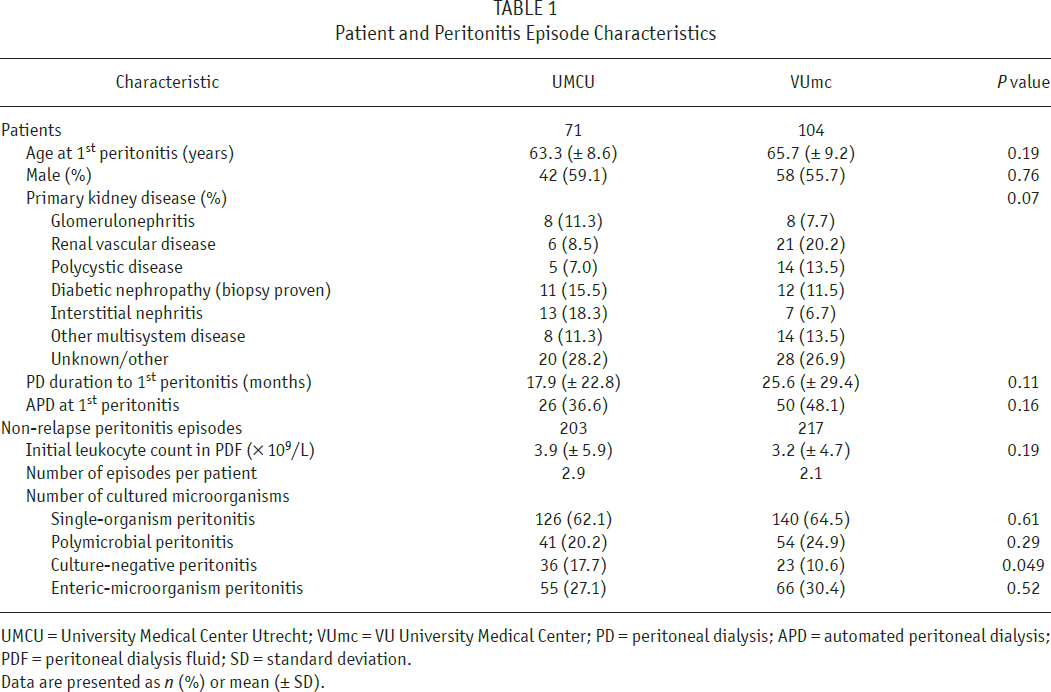
UMCU = University Medical Center Utrecht; VUmc = VU University Medical Center; PD = peritoneal dialysis; APD = automated peritoneal dialysis; PDF = peritoneal dialysis fluid; SD = standard deviation.
Data are presented as n (%) or mean (± SD).
Culture Results
Table 2 shows all organisms cultured in the 420 non-relapse peritonitis episodes. In 29.1% (UMCU) and 33.9% (VUmc), respectively, EM were found, with E. coli, Klebsiella, and Enterococcus being the most common species in both centers. About half of the cultures revealed gram-positive, non-Enterococcal organisms.
Causative Microorganisms of All 420 Non-Relapse Peritonitis Episodes
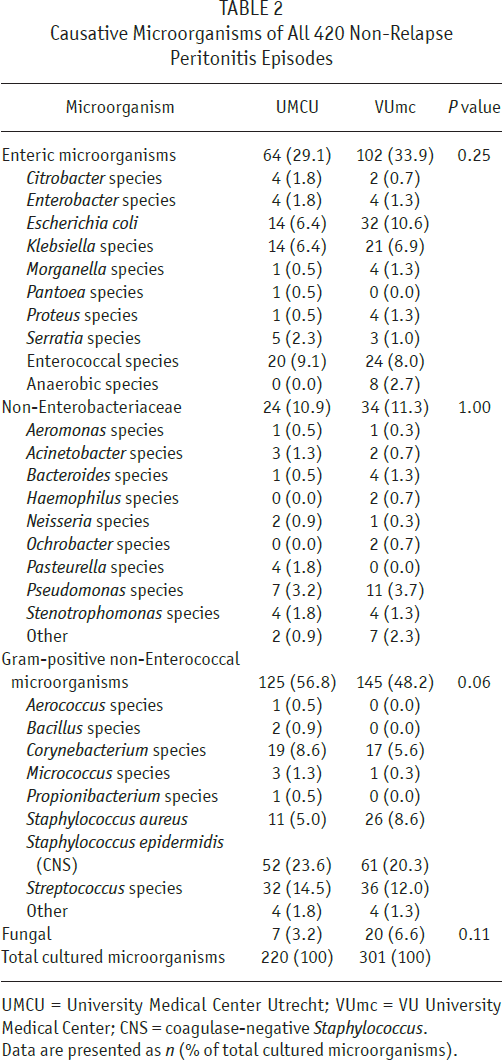
UMCU = University Medical Center Utrecht; VUmc = VU University Medical Center; CNS = coagulase-negative Staphylococcus.
Data are presented as n (% of total cultured microorganisms).
In the UMCU, microbial sensitivity results could be retrieved retrospectively in 65% of the episodes in which the MeroPerRest protocol was applied (106/163 episodes). In 97/106 episodes (91.5%), all microorganisms cultured were sensitive to meropenem. In 3 episodes (2.8%), bacteria resistant to meropenem were found (Stenotrophomonas species, n = 2, and Enterococcus faecium, n = 1). Candida species were cultured in 6 episodes (6.7%). In the 35.0% of cases in which sensitivity data could not be retrieved, no clinical resistance to meropenem was observed. In the VUmc, microbial sensitivity was retrieved in 88.1% of the episodes treated with gentamicin-rifampicin protocol (141/160 episodes). In 124/141 episodes (87.9%), all cultured bacteria were sensitive to the gentamicin-rifampicin combination, but in 6/141 episodes (4.3%), resistant bacteria were found. Candida species were cultured in 11 episodes (7.8%). No extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae or methicillin-resistant Staphylococcus aureus (MRSA) were detected in either the UMCU or the VUmc cohort.
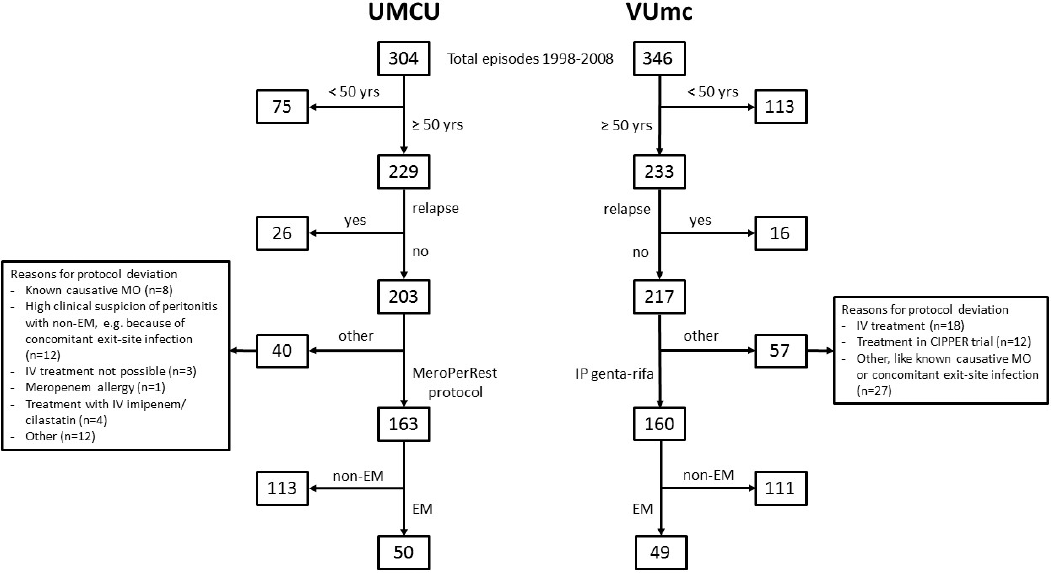
Flow chart of the study. UMCU = University Medical Center Utrecht; VUmc=VU University Medical Center; yrs = years; MO = microorganism; EM = enteric microorganisms; non-EM = non-enteric microorganisms; IP genta-rifa = intraperitaneal gentamicin-rifampicin; IV = intravenous.
In episodes of EM peritonitis, multiple organisms, including Candida species, were isolated in 48.0% in the UMCU and 47.0% in the VUmc.
Outcome of Peritonitis Episodes
Fifty episodes in the UMCU (in 30 patients) were caused by EM and were treated according to the Mero-PerRest protocol, and 49 episodes (in 37 patients) in the VUmc were initially treated with the gentamicin-rifampicin protocol (Figure 1). The primary cure rate was significantly higher with the Mero-PerRest protocol (90.0%) than with the gentamicin-rifampicin protocol (65.3%), even after adjustment for possible con-founders (adjusted odds ratio [OR] 4.54, 95% confidence interval [CI] 1.46 – 14.15) (Table 3). Relapse rates did not differ (8.0% vs 12.2%, p = 0.52). In both centers, HD was necessary in 8 episodes (16.0% vs 16.3%). While this was mostly temporary in the UMCU (7 of 8), the majority of the VUmc episodes (6 of 8) led to permanent HD transfer, possibly due to a higher catheter removal rate (30.6% vs 4.0% in the UMCU, p = 0.0004). Technique survival was significantly lower with the gentamicin-rifampicin protocol (69.4% vs 90.0% with the Mero-PerRest protocol, adjusted OR 3.41, 95% CI 1.07 – 10.87). Patient survival tended to be better with the Mero-PerRest protocol (92.0% vs 81.6% with the gentamicin-rifampicin protocol), but statistical significance was not reached (Table 3).
Outcome of Peritonitis Episodes in UMCU vs VUmc: Crude and Adjusted Odds Ratios for Primary Cure, Technique Survival, and Patient Survival
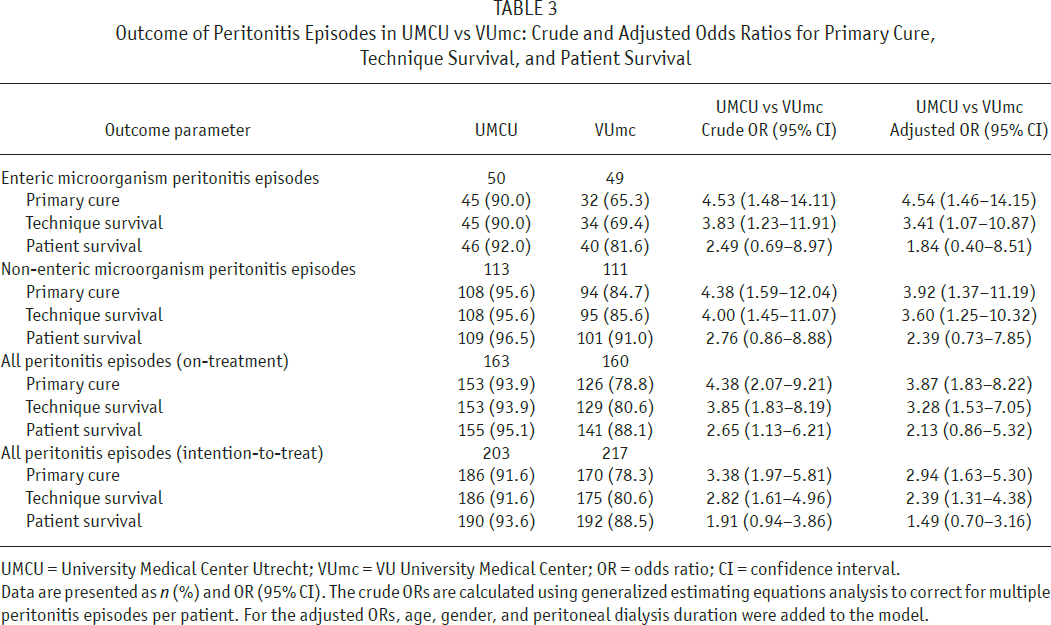
UMCU = University Medical Center Utrecht; VUmc = VU University Medical Center; OR = odds ratio; CI = confidence interval.
Data are presented as n (%) and OR (95% CI). The crude ORs are calculated using generalized estimating equations analysis to correct for multiple peritonitis episodes per patient. For the adjusted ORs, age, gender, and peritoneal dialysis duration were added to the model.
In the VUmc, roughly two-thirds of all EM peritonitis episodes were cured by antibiotics alone. Interestingly, this was the case in only 34.8% of polymicrobial episodes, whereas this figure was 92.3% for single-organism episodes (p < 0.0001, Figure 2). In the UMCU, the overall cure rate of EM peritonitis episodes was 90.0%, and this was entirely due to the much higher cure rate in polymicrobial EM peritonitis of 87.5%, which was comparable to that in single organism EM peritonitis in both the VUmc and UMCU.
In 113 non-relapse episodes in the UMCU in 51 patients and 111 episodes in the VUmc in 62 patients, cultures showed non-EM peritonitis (Figure 1). The relapse rate was higher in the UMCU (9.7% vs 1.8% in the VUmc, p = 0.02), probably due to a lower catheter removal rate (1.8% vs 9.9%, respectively, p = 0.01). Nevertheless, primary cure rate and technique survival were better with the Mero-PerRest protocol (both 95.6%) than with the gentamicin-rifampicin protocol (84.7% and 85.6%, respectively), which was statistically significant (adjusted OR 3.92, 95% CI 1.37 – 11.19 and adjusted OR 3.60, 95% CI 1.25 – 10.32, respectively). Patient survival did not differ significantly (96.5% vs 91.0% with gentamicin-rifampicin protocol) (Table 3).
Intention-to-treat analysis including all 420 episodes showed that the adapted UMCU protocol was associated with a significantly higher primary cure rate (91.6% vs 78.3% in VUmc with traditional treatment, adjusted OR 2.94, 95% CI 1.63 –, 5.30) and technique survival (91.6% vs 80.6% with traditional treatment, adjusted OR 2.39, 95% CI 1.31 – 4.38). Patient survival did not differ significantly (93.6% vs 88.5% with VUmc protocol) (Table 3).
Patient Outcomes
Overall, technique survival was significantly better using the Mero-PerRest protocol (76.1% vs 58.7% with the gentamicin-rifampicin protocol, p = 0.02), and the number of catheter interventions was significantly lower (8.5% vs 40.4% in the VUmc, p < 0.0001) (Figure 3A). As shown in Figure 3B these differences were mainly caused by the significantly poorer outcome in EM peritonitis-prone patients treated with the gentamicin-rifampicin protocol.
In the VUmc, 54/104 patients (51.9%) had no EM peritonitis but experienced 104 episodes of non-EM peritonitis. In this group, mortality was 16.7% and technique survival 70.4%. The number of catheter interventions related to peritonitis was 27.8%. The remaining 50 patients (48.1%) were EM peritonitis-prone, experiencing 66 EM peritonitis episodes and 47 non-EM peritonitis episodes. Thirty-two percent of them died, but the mortality difference with the non-EM group did not reach statistical significance (p = 0.11). Death was attributable to EM peritonitis in 75.0% of cases. Technique survival in this group was poor and significantly lower than in VUmc patients not having EM peritonitis (46.0% vs 70.4%, p = 0.02), and catheter interventions were performed in 54.0% of the patients (vs 27.8% in non-EM peritonitis, p = 0.01). Of these interventions, 21/27 (77.8%) were performed in the course of EM peritonitis (Figure 3B and Supplemental Table 1).
In the UMCU, 37/71 patients (52.1%) had no EM peritonitis but experienced 86 episodes of non-EM peritonitis. The mortality (18.9%) and technique survival rates (75.7%) did not significantly differ from the non-EM peritonitis group in the VUmc, but the catheter intervention rate was significantly lower using the adapted UMCU protocol (8.1% vs 27.8%, p = 0.03). The remaining 34 patients (47.9%) were EM peritonitis-prone, experiencing 55 EM peritonitis episodes and 62 non-EM peritonitis episodes. In marked contrast to the VUmc, mortality (17.6%) and technique survival rate (76.5%) in the EM peritonitis-prone patients were virtually the same as in non-EM peritonitis-prone patients in the UMCU. All deaths (n = 6) occurred in the course of EM peritonitis. In the UMCU, the catheter intervention rate in patients with EM peritonitis episodes (8.8%) was not different from that in patients not prone to EM peritonitis and markedly lower than in EM peritonitis-prone patients in the VUmc (54.0%, p < 0.0001). Technique survival in EM peritonitis-prone patients was significantly better using the Mero-PerRest protocol (76.5%) than with the gentamicin-rifampicin protocol (46.0%, p = 0.007) (Figure 3B and Supplemental Table 1).
Discussion
The present study shows that in patients ≥ 50 years old, application of a peritonitis treatment protocol involving temporary discontinuation of PD without removing the PD catheter while giving IV meropenem and as catheter lock resulted in a markedly improved overall primary peritonitis cure rate and PD technique survival compared with a traditional IP peritonitis treatment protocol. This effect was most distinct in patients with EM peritonitis, for which the protocol was specifically designed. Interestingly, the beneficial effect seemed to be more pronounced in the subgroup of cases of polymicrobial EM peritonitis.
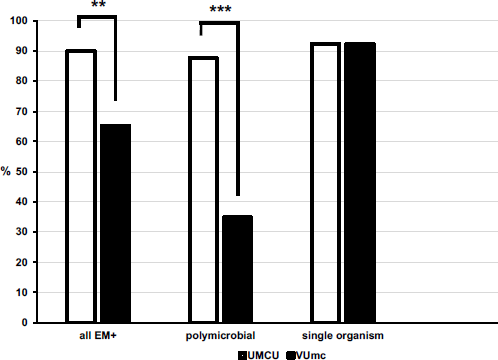
Primary cure rate of polymicrobial and single-organism EM peritonitis episodes. Primary cure rates with the Mero-PerRest protocol compared with IP gentamicin-rifampicin of polymicrobial EM peritonitis episodes (24 vs 23 episodes, respectively) and single-EM peritonitis episodes (26 vs 26 episodes, respectively). On-treatment analysis.
The primary cure rate of EM peritonitis episodes reported in the literature is poor, averaging only ∼55% (1–3,5,16). In this respect, the primary cure rate for EM peritonitis in the VUmc (65.3%), which used a traditional IP peritonitis treatment protocol, was quite good. Nevertheless, application of the Mero-PerRest protocol improved the primary cure rate in EM peritonitis further to 90.0%. A significant reduction in catheter removal rate and a tendency toward reduced mortality and permanent transfer to HD resulted in a considerable and significantly better technique survival rate in the UMCU (90.0% vs 69.4% per episode in the VUmc). These outcomes were also considerably better than those reported in the literature on EM peritonitis episodes, which show a high catheter removal rate (∼35%) (1,3,5,17,18), permanent transfer to HD (∼25%) (1,3,16), and mortality (> 40% in older studies, ∼8% in more recent studies) (1–4,6,16,19–22), as well as a reduced technique survival (∼70%) (1,3,17).
The beneficial effect of the Mero-PerRest protocol on the outcome of EM peritonitis was largely due to its favorable effect in polymicrobial episodes, as the outcome in single-organism EM peritonitis was very good and not different between the 2 treatment protocols (Figure 2). This suggests that multiple-and single-organism EM peritonitis are different entities. It is tempting to speculate that the polymicrobial form of EM peritonitis, with its poor prognosis when managed using traditional IP treatment protocols, is caused by underlying abdominal pathology. In contrast, the single-organism variant could more often result from trans- or periluminal migration of EM derived from the perineal area. This is supported by the finding that exit-site treatment with gentamicin cream for prevention of S. aureus infections also induced a one-third reduction in the incidence of gram-negative peritonitis (23). However, the distinction between polymicrobial and single-organism EM peritonitis may not be absolute, as single-organism EM peritonitis has also been reported in cases of proven severe intra-abdominal pathology (6).
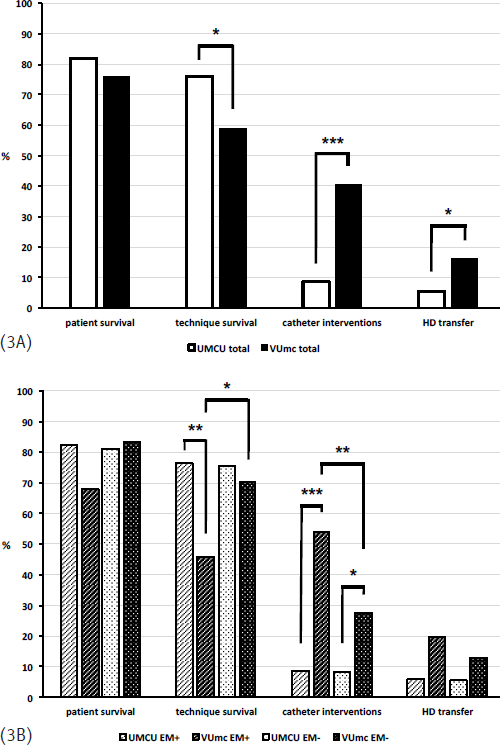
Patient outcomes. Patient survival, technique survival, catheter interventions, and HD transfer in all patients (3A) from UMCU and VUmc and in patients who have experienced at least 1 peritonitis episode with enteric microorganisms (EM+) and in patients who have never experienced peritonitis with enteric microorganisms (EM-) (3B). Analysis on intention-to-treat basis.
Half of the study population was prone to developing EM peritonitis. The intention-to-treat analysis of patient outcomes showed a tendency toward reduced patient mortality and permanent HD transfer, resulting in a statistically significant increased technique survival in EM peritonitis-prone patients (76.5% vs 46.0% of patients treated with a traditional protocol). In fact, the treatment outcome in patients prone to EM peritonitis in the UMCU became entirely comparable with that in non-EM peritonitis. It is of note that the rate of catheter interventions in EM peritonitis was considerably lower with the Mero-PerRest protocol (8.8% of patients) than with the gentamicin-rifampicin protocol (54.0% of patients). This suggests that the development of refractory cases that prompt catheter interventions are to a large extent prevented by the Mero-PerRest protocol. This is relevant, because permanent transfer to HD and mortality were > 80% after a catheter intervention in the VUmc.
Interestingly, both primary cure rate and technique survival of non-EM peritonitis episodes using the Mero-PerRest protocol was also significantly better than with the gentamicin-rifampicin protocol, although to a lesser extent (95.6% vs 84.7% of episodes and 95.6% vs 85.6% of episodes, respectively). On the one hand, this may be due to the possible favorable effect of temporary interruption of PD, also in non-EM peritonitis (24,25). On the other hand, the increased technique survival in the UMCU in episodes of non-EM peritonitis appeared to be largely due to a markedly reduced incidence of catheter interventions (1.8% vs 9.9% per episode). This was also found in patients not prone to EM peritonitis in the UMCU, in whom the catheter intervention rate was only 30% of that in the VUmc.
The design of the Mero-PerRest protocol was based on 3 assumptions. The first is that EM peritonitis cannot be diagnosed at presentation using clinical and laboratory parameters (2,4). This delays antibiotic treatment adequately covering the intestinal flora until EM peritonitis is identified by culture. This may lead to refractory cases with a protracted course, triggering frequent adaptations of antibiotic therapy. For instance, Jarvis et al. reported that a conversion to a second regime of antibiotics was needed in 64% of cases and change to a third schedule in another 21%, with an average delay of 3 and 6 days, respectively (1). In the study by Szeto et al., a second antibiotic had to be added to the original therapy in 39% of cases (2).
The second assumption is that age is associated with EM peritonitis. In the study of Jarvis et al., the OR for the occurrence of peritonitis with gram-negative microorganisms was 1.68 for patients in the highest age tertile compared with the lowest tertile (1). We postulate that this is predominantly related to the increasing incidence of diverticular disease of the colon with age (8,9). Indeed, the risk of EM peritonitis in PD patients is associated with the presence and severity of diverticular disease of the colon (21,26,27). In line with this, a review of abdominal catastrophes in PD patients showed that diverticular disease of the colon was by far the most frequent underlying pathology (28). The age cut-off of 50 years of the Mero-PerRest protocol was based on the paper by Wu et al. (26).
The third assumption is that it is not the removal of the PD catheter per se that causes resolution of refractory EM peritonitis, but that the resulting peritoneal rest has this effect. This suggests that PD itself affects the natural history of abdominal pathology by interfering with local defense mechanisms. In this respect, the non-physiological composition of the dialysate, the prevention of sealing of perforations by the presence of PD fluid or the interference with peritoneal humoral and cellular defense mechanisms by intermittent draining of the abdomen could all play a role. This notion is supported by the observations of Harwell et al., who showed that the incidence of abdominal catastrophes is increased 20- to 60-fold in PD patients compared with those on HD or after renal transplantation (6). In line with this idea, Spital successfully applied peritoneal rest with IV antibiotics without removing the catheter in a case of refractory EM peritonitis caused by diverticular disease of the colon (29). A similar case was reported by Nebel (30). Later reports confirmed the value of temporary discontinuation of PD without catheter removal in treating refractory EM peritonitis (31,32), even in a case of perforated appendicitis (33).
Based on these assumptions, we considered elderly patients to be at risk of EM peritonitis and decided to treat them by peritoneal rest and IV therapy with meropenem. This drug has excellent activity against the majority of gram-negative, gram-positive, and anaerobic pathogens, making it well suited as an empirical treatment of intra-abdominal infections (34). In non-dialysis patients, several randomized trials indeed favored treating intra-abdominal infections with meropenem (35).
Meropenem was also applied as catheter lock because EM peritonitis relapsed frequently after resuming PD in the early developmental phase of the protocol. This was attributed to leaving the inside of the catheter untreated during IV antibiotic therapy. Reports on catheter locks in the treatment of PD-related peritonitis are scarce. Lee et al. described the successful use of a ceftazidime-heparin lock in the treatment of 2 cases of refractory gram-negative peritonitis without the necessity of catheter removal (36). Usberti et al. successfully applied a sulbactam-ampicillin catheter lock in combination with oral ciprofloxacin and temporary interruption of PD in patients with uncomplicated predominant staphylococcal peritonitis (25). The potential importance of intracatheter treatment is illustrated by the favorable effect of an amphotericin lock in the treatment of fungal peritonitis in PD patients, allowing a cure without catheter removal in this form of peritonitis that is often refractory to treatment (11).
The present study has several limitations. One is that the data sets were obtained in 2 different hospitals, and it can therefore not be excluded that the observed differences were due to center effects, such as differences in prevalence of ESBL-producing Enterobacteriaceae and MRSA. However, no episode in our study was caused by one of them. Because of study design (1 treatment strategy per hospital), additional correction at center level with a multilevel model is not possible. Several questions remain specifically with respect to the Mero-PerRest protocol. First, it is unknown whether the protocol is also effective if started after confirmation of EM peritonitis by culture or even when conventional treatment of such an episode is failing. Second, the optimal duration of the interruption of PD has not been assessed, as the period of 1 week has been chosen on very limited literature data (29,30). Third, the optimal age criterion, balancing the unnecessary application of the protocol and missed EM peritonitis episodes, has not been determined. Fourth, the necessity of a catheter lock, the most suitable antibiotic for this, and its optimal intracatheter concentration have not been studied. Fifth, we did not formally test the hypothesis that diverticular disease of the colon was the predominant cause of EM peritonitis in our cohort by radiological imaging or colonoscopy. Other causes of translocation of microorganisms into the peritoneal cavity, such as ischemic bowel disease, appendicitis, or cholecystitis may have played a role in some patients (4,6). In addition, as mentioned above, part of the single-organism EM peritonitis episodes may have had an exogenous origin. However, in view of the high incidence of diverticulosis in patients in the age range of our cohorts, at least 50% are expected to have colonic diverticula with a predicted rate of complications such as diverticulitis of up to 25% (9). In accordance with this, a colonic origin dominates in many reports of polymicrobial EM peritonitis or surgical abdominal catastrophes in PD patients (20,28), and diverticular disease of the colon is considered to be an important cause of EM peritonitis (21,26,27). Finally, the relative contributions of the broad initial antibiotic coverage, the specific type of antibiotic, and the interruption of PD have not been determined. To study this, a trial involving at least 4 groups of patients would be needed: (1) standard empirical antibiotics, continuing PD; (2) standard empirical antibiotics, interrupting PD; (3) meropenem, continuing PD; (4) meropenem, interrupting PD. However, extensive use of meropenem may lead to carbapenem-resistance (37), of which the prevalence in the Netherlands is fortunately still low (38). Therefore, it would also be relevant to compare an alternative antibiotic treatment protocol that covers most of the intestinal flora with meropenem in this trial. All in all, this proposed trial would be large and difficult to perform, especially in the light of the current and ongoing decline in the number of PD patients in many countries.
Conclusions
We have shown that the dismal outcome of EM peritonitis in PD patients 50 years old and above could be improved markedly by a protocol involving discontinuation of PD without catheter removal and broad initial IV and intracatheter antibiotic treatment that covers most of the intestinal flora. This favorable effect was most distinct in patients with polymicrobial EM peritonitis. Due to the type of data available, the relative contribution of the broad initial antibiotic coverage and the temporary interruption of PD to the improved outcome remain to be determined.
Footnotes
ACA has received speaker fees from Baxter Healthcare and Fresenius Medical Care. PMW has received consulting fees from AMGEN, Eli Lilly and Sanofi and speaker fees from Fresenius Medical Care. WHB has received speaker fees from Baxter Healthcare. WR and FJI declared no competing interests.