
Abstract
Keywords
With the population aging, utilization of critical care services is expected to increase (Carson, Cox, Holmes, Howard, & Carey, 2006; Needham, Bronskill, et al., 2005) while intensive care unit (ICU) mortality decreases (Lilly, Zuckerman, Badawi, & Riker, 2011). Hence, there is a growing pool of survivors of critical illness who frequently have long-term ICU-related neuromuscular problems, including muscle weakness, joint contractures, and impairment in activities of daily living (ADLs; Burtin et al., 2009; Clavet, Hébert, Fergusson, Doucette, & Trudel, 2008; De Jonghe et al., 2002; Latronico, Shehu, & Seghelini, 2005; Vest, Murphy, Araujo, & Pisani, 2011; Zanni et al., 2010). These impairments are particularly common and severe for survivors of severe critical illness, including patients with acute respiratory failure or acute lung injury (ALI) and acute respiratory distress syndrome (Barnato, Albert, Angus, Lave, & Degenholtz, 2011; Bienvenu et al., 2012; Desai, Law, & Needham, 2011; Herridge et al., 2003, 2011; Wunsch et al., 2010).
As a consequence of these important issues, the focus on introducing early rehabilitation interventions in the ICU to improve patients’ long-term outcomes is increasing (Herridge, 2009; Needham, 2008; Needham et al., 2012; Rubenfeld, 2007). Studies of early rehabilitation interventions in the ICU have demonstrated safety, feasibility, and improved patient outcomes (Adler & Malone, 2012; Bailey et al., 2007; Burtin et al., 2009; Morris et al., 2008; Pohlman et al., 2010). In particular, in a randomized controlled trial of early (vs. later) occupational and physical therapy, initiated at a median of 1.5 (vs. 7.4) days after the start of mechanical ventilation, patients demonstrated significantly improved physical function at hospital discharge (Schweickert et al., 2009). Despite this evidence, early rehabilitation has not yet been widely adopted in many ICUs (Bahadur, Jones, & Ntoumenopoulos, 2008; Gosselink et al., 2008; O’Connor & Walsham, 2009).
Understanding factors associated with the timing of rehabilitation therapy in the ICU can help in understanding barriers to earlier therapy. As such, our objective was to evaluate the association of patient, ICU, and hospital factors with the time to first occupational therapy intervention in the ICU in a prospective cohort of mechanically ventilated patients with ALI.
Method
Research Design
This research was conducted as part of a prospective cohort study of patients with ALI (Needham, Dennison, et al., 2005). This study was approved by the institutional review boards (IRBs) of all participating institutions. All IRBs approved a waiver of consent permitting collection of observational data without informed consent.
Participants
We enrolled consecutive mechanically ventilated patients meeting standard ALI diagnostic criteria (Bernard et al., 1994). Exclusion criteria included (1) limitations in care at the time of study enrollment (such as no vasopressors), (2) >5 days of mechanical ventilation before study eligibility, (3) baseline language or communication barrier, (4) preexisting cognitive impairment, and (5) preexisting illness with a life expectancy of <6 mo.
Outcome Variable
The outcome variable for this analysis was the time from ALI onset (i.e., study enrollment) to first occupational therapy intervention during the ICU admission for ALI. We collected dates of occupational therapy interventions from medical records based on standardized documentation procedures used at each study site hospital. Occupational therapy interventions were defined specifically as excluding interventions that exclusively involved only splinting, bracing, or passive positioning to evaluate factors associated with interventions typically considered part of early rehabilitation activities in the ICU (Korupolu, Gifford, & Needham, 2009).
Exposure Variables
Exposures evaluated for association with time to first occupational therapy intervention in the ICU were grouped into patient, ICU, and hospital factors. Patient factors, abstracted from the medical record, included the following: demographics (age, sex, and race), body mass index, ICU admission diagnosis, and prehospitalization comorbidity status using the Functional Comorbidity Index (Groll, To, Bombardier, & Wright, 2005). We used the Acute Physiology and Chronic Health Evaluation II (APACHE II) score to assess the severity of illness within the first 24 hr of ICU admission (Knaus, Draper, Wagner, & Zimmerman, 1985). Time-varying patient factors, measured daily in the ICU, included the following: organ failure status (using Sequential Organ Failure Assessment [SOFA] score; Vincent et al., 1996), use of continuous hemodialysis, delirium status (not delirious, delirious, or comatose) using the validated Confusion Assessment Method for the Intensive Care Unit (Ely et al., 2001), and mechanical ventilation status and fraction of inspired oxygen (FiO2). ICU-related factors evaluated included type of ICU (medical, surgical, trauma) and daily interruption of sedation medication infusions (Kress, Pohlman, O’Connor, & Hall, 2000). We evaluated hospital study site as a hospital-related factor.
Missing Data
Delirium assessments were not always available for reasons such as the patient being unavailable and a weekend or holiday period without research staff coverage to perform the prospective assessments. To address these missing data and maintain the study sample size for statistical analyses, we used multiple imputation methods (Rubin, 1987) that allowed us to impute (i.e., predict) missing delirium status on days on which data were not collected. The imputed values were based on a logistic regression model for delirium status as a function of clinically relevant predictors of delirium. As per standard methods for multiple imputation, these imputed values were calculated to create five datasets with no missing data.
Data Collection
We collected patient demographic data, prehospitalization comorbidities, ICU admission diagnosis and severity of illness, and daily ICU data from the medical record after study enrollment (Needham et al., 2007). Delirium assessments were conducted daily by trained research staff. All data collectors underwent didactic training on the data collection forms and procedures documented in study operation manuals (Needham, Dennison, et al., 2005). Collectors were required to pass initial quality assurance reviews by the lead study investigator or coordinator before they collected data independently. Routine quality assurance reviews were conducted throughout the data collection period of the study.
Data Analysis
Descriptive statistics were calculated with comparisons performed using χ2, Fisher’s exact, and Wilcoxon rank-sum tests, as appropriate. We used χ2 and Fisher’s exact tests to compare the proportion of participants who received occupational therapy across levels of categorical exposure. The Wilcoxon rank-sum test compared the distribution of continuous exposures for participants who did and did not receive occupational therapy. Exposures were continually assessed up to the earliest study endpoint, defined as the day the patient received the first occupational therapy intervention, died, or was discharged from the ICU (censoring).
Fine and Gray (1999) proportional subdistribution hazards regression was used for analysis of the primary outcome. This methodology appropriately accounts for the competing risk of death in analyzing the time until first occupational therapy intervention because patients with greater severity of illness are both less likely to receive occupational therapy and more likely to die (Varadhan et al., 2010). This statistical regression model estimates the association of exposures with the time until a first occupational therapy intervention and provides a statistical measure known as a hazard ratio (HR). For a specific exposure, an HR >1 indicates that a first occupational therapy intervention in the ICU is more likely to occur and an HR <1 indicates that a first occupational therapy intervention is less likely to occur. The daily patient exposures (SOFA score, delirium status, sedation interruption, mechanical ventilation status, and FiO2) were appropriately treated in the regression analysis as time-varying variables.
Bivariate models were fit, and the results were averaged over the imputed datasets using Rubin’s (1987) method. The final regression model included all exposures that had a bivariate association with time to occupational therapy at p ≤ .15. Cumulative incidence function curves were created by first fitting this final regression model to each of the five imputed delirium datasets and obtaining the average cumulative incidence. The proportional hazard assumption for each exposure was evaluated by visually inspecting the plot of Schoenfeld (1982) residuals versus time. After inspection of the plots, interaction terms were created for exposures that have potential nonproportional hazards over time. However, these interaction terms were nonsignificant (p > .05) and, hence, not included in the final multivariate model. The absence of multicollinearity was confirmed using variance inflation factors (Hamilton, 2009). Statistical significance was defined as two-sided p < .05. Statistical analyses were performed using STATA 12.0 software (Stata Corporation, College Station, TX) and R (R Development Core Team, 2011).
Results
The analysis included data for 514 consecutive eligible patients enrolled from 11 ICUs at three academic hospitals in Baltimore, MD, from October 2004 to October 2007. Of these 514 patients, 154 (30%) received occupational therapy during the ICU stay for ALI. Table 1 presents patients’ characteristics and compares those who ever versus never received any occupational therapy intervention during their ICU stay for ALI. The two groups had significant differences in the distribution of ICU diagnoses, with 86% of those ever and 96% of those never receiving occupational therapy having medical diagnoses. Those who never received occupational therapy had significantly worse severity of illness at ICU admission, with a median APACHE II score of 28 (interquartile range [IQR] = 21–35) vs. 23 (IQR = 18–29; p < .001). Additionally, those who never received occupational therapy had worse SOFA scores, greater utilization of continuous hemodialysis, higher mean oxygen requirements, and greater proportion of days with coma (Table 1).
Baseline Characteristics, by ICU Occupational Therapy Status
Note. APACHE II = Acute Physiology and Chronic Health Evaluation II; BMI = body mass index; FiO2 = fraction of inspired oxygen; ICU = intensive care unit; IQR = interquartile range; SOFA = Sequential Organ Failure Assessment.
Comparing “ever occupational therapy” and “never occupational therapy” and calculated using Pearson χ2, Fisher’s exact, and Wilcoxon rank-sum tests, as appropriate. bCalculated using available (i.e., not imputed) data.
The 154 patients who received occupational therapy interventions during their ICU stay had 551 days with at least one occupational therapy intervention, representing 16% of all their ICU days. The median number of occupational therapy visits per patient was 2 (IQR = 1–4) and the median duration of treatment was 30 min (IQR = 25–45). Patients could have more than one type of treatment coded during an occupational therapy visit, with the most common treatments being upper-extremity exercise (43%), range of motion (passive, passive–assistive, or active; 32%), ADL training (31%), and functional mobility (15%).
The number of days to the first occupational therapy intervention, death, or discharge from the ICU was not significantly different between those who ever (median = 8.5 days, range = 6–13) versus never (median = 8 days, range = 4–13) received occupational therapy. Table 2 shows the results of the multivariate regression analysis demonstrating several patient, ICU, and hospital factors independently associated with time to first occupational therapy intervention. Worse organ failure, as indicated by a higher SOFA score or ever receiving continuous hemodialysis, was associated with a longer time until occupational therapy intervention, with relative HRs of 0.91 (95% confidence interval [CI] [0.87, 0.94]) and 0.53 (95% CI [0.31, 0.92]) for those ever versus never receiving occupational therapy, respectively.
Factors Associated With Time to Initiating Occupational Therapy in the ICU
Note. Hazard ratios >1 indicate an association with earlier initiation of occupation therapy in the ICU. Hazard ratios calculated using Fine and Gray proportional subdistribution hazards regression models (Fine & Gray, 1999) with time-varying exposures for daily SOFA score, delirium, mechanical ventilation status, FiO2, and sedation interruption. APACHE II = Acute Physiology and Chronic Health Evaluation II; BMI = body mass index; FiO2 = fraction of inspired oxygen; ICU = intensive care unit; Ref. = reference category; SOFA = Sequential Organ Failure Assessment.
Missing data imputed using multiple imputation (Rubin, 1987).
Among ICU factors, admission to a trauma ICU (vs. a medical ICU) was associated with shorter time to an initial occupational therapy intervention (HR = 3.82, 95% CI [1.54, 9.49]). Figure 1 shows the adjusted cumulative incidence of initial occupational therapy intervention by type of ICU. In addition, compared with receiving no sedative infusions, uninterrupted sedation infusions were associated with a longer time to first occupational therapy treatment, particularly when sedation infusions were not interrupted daily (HR = 0.44, 95% CI [0.29, 0.67]). Independent of these patient and ICU factors, hospital site was also associated with time to first occupational therapy intervention. Compared with hospital Site 1, admission to Site 2 was associated with delayed occupational therapy with a relative HR of 0.44 (95% CI [0.27, 0.72]), whereas admission to Site 3 was associated with earlier time to occupational therapy (HR = 1.90, 95% CI [1.24, 2.92]). Figure 2 illustrates the differing adjusted cumulative incidence of occupational therapy in the ICU among the three hospital sites.
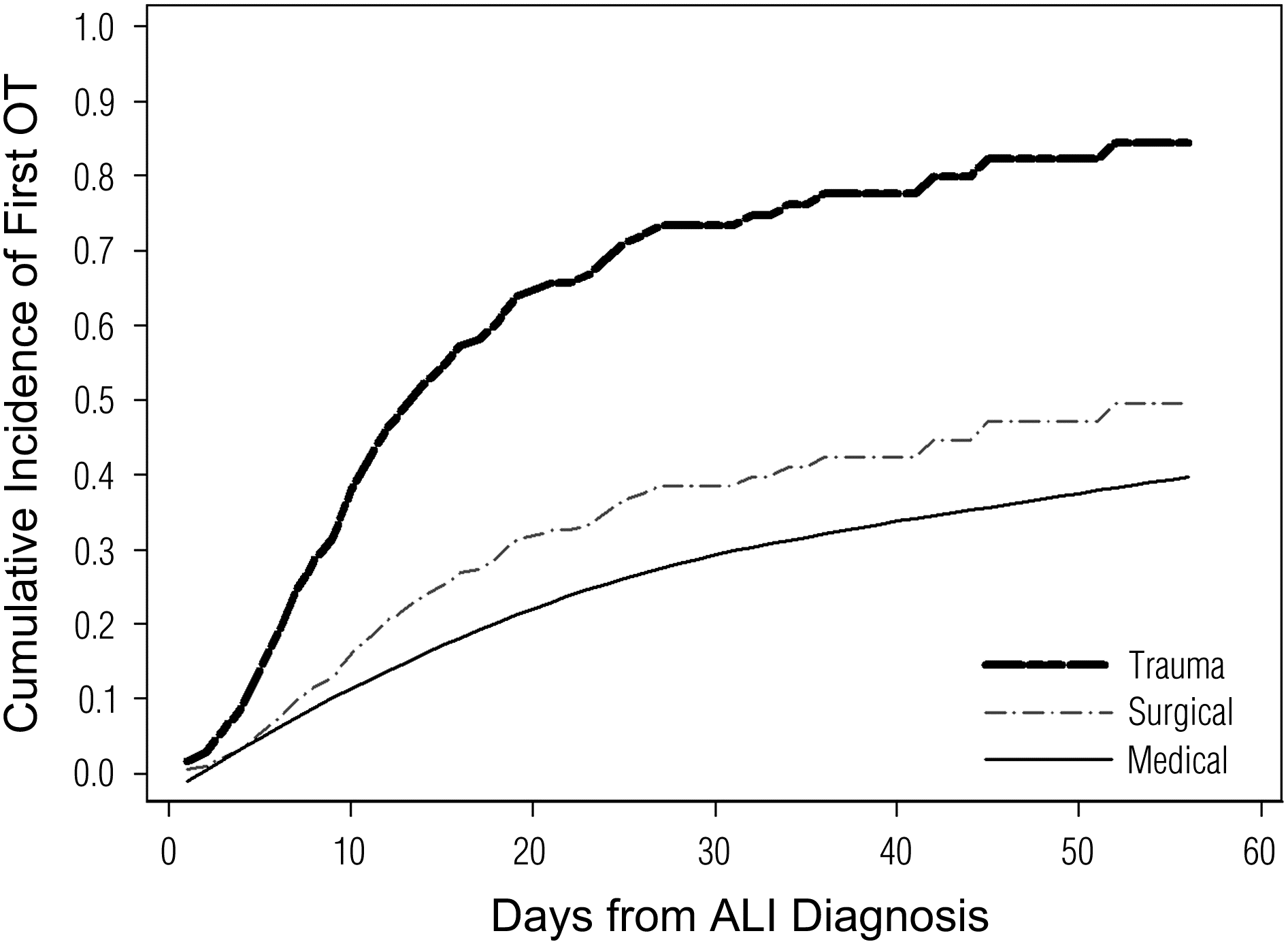
Estimated adjusted cumulative incidence of initiating occupational therapy (OT) intervention in the intensive care unit, by intensive care unit admission type.
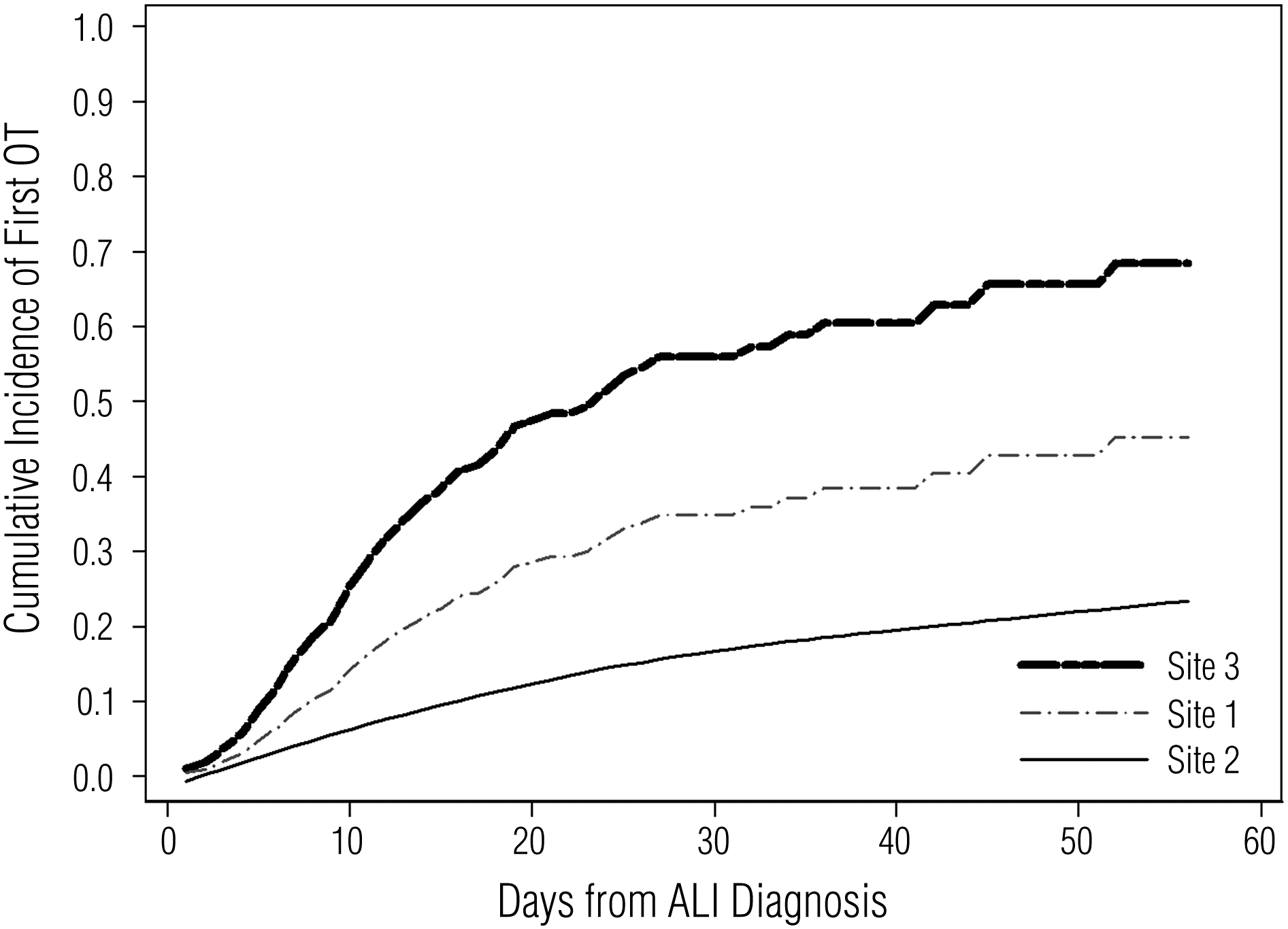
Estimated adjusted cumulative incidence of initiating occupational therapy (OT) intervention in the intensive care unit, by hospital.
Discussion
In this prospective cohort of 514 consecutive patients with ALI from 11 ICUs in three academic hospitals, only 30% ever received any occupational therapy intervention during their ICU stay. Severity of patients’ critical illness, including increased organ failure and receiving continuous hemodialysis, was associated with delayed initiation of occupational therapy. Independent of these factors, ICU sedation practice, ICU type, and hospital site were also associated with timing of occupational therapy initiation.
In this study of patients with ALI, severity of illness was associated with delayed initiation of occupational therapy in the ICU. For example, use of continuous hemodialysis was associated with delayed occupational therapy initiation. However, others have shown that some ICU patients receiving continuous hemodialysis can receive rehabilitation (Hopkins & Spuhler, 2009). Recent studies of mechanically ventilated ICU patients have consistently demonstrated the safety of early rehabilitation in the ICU (Bailey et al., 2007; Burtin et al., 2009; Morris et al., 2008; Needham & Korupolu, 2010; Needham et al., 2010; Pohlman et al., 2010; Schweickert et al., 2009). Training and education may help overcome perceived barriers of critical illness in initiating earlier occupational therapy interventions in the ICU.
Sedation practices often vary between ICUs with variable uptake in the implementation of evidence-based daily interruption of sedative infusions (Kress et al., 2000). Deep sedation and use of sedatives are recognized as important barriers associated with delayed rehabilitation in the ICU (Thomsen, Snow, Rodriguez, & Hopkins, 2008; Zanni et al., 2010). Minimizing sedation is an important step in optimizing patients’ eligibility for early rehabilitation (Desai et al., 2011; Hopkins & Spuhler, 2009; Needham, 2008; Needham et al., 2010; Schweickert et al., 2009).
Despite accounting for these significant patient factors and ICU sedation factors, ICU type and hospital site were each significantly associated with time to first occupational therapy intervention in the ICU. These findings suggest that culture or attitude toward rehabilitation might be different among types of ICU. Changing ICU culture to embrace and prioritize early rehabilitation is a critical step to successful adoption of early rehabilitation programs in the ICU (Bailey, Miller, & Clemmer, 2009; Hopkins & Spuhler, 2009; Needham & Korupolu, 2010). Results may also be affected by differences in occupational staffing in specific ICUs. Occupational therapists may draw on results of this study to help effect evidence-based communication and promotion of occupational therapy’s role (Ciro, 2011), especially in creating multidisciplinary early rehabilitation teams in the ICU (Needham et al., 2010; Schweickert et al., 2009).
Limitations and Future Research
This study has some potential limitations. First, because the study was observational, causality cannot be established between these patients and institutional factors with time to first occupational therapy intervention. However, certain factors (e.g., severity of illness) are not amenable to randomization to more clearly determine causality using a controlled trial. Moreover, our observed associations appear credible given their consistency with previously postulated barriers from other studies (Bailey et al., 2009; Garnacho-Montero et al., 2001; Hopkins & Spuhler, 2009). Our study is unique in providing empirical evaluation of these barriers to early occupational therapy intervention.
Second, results from this study might not be generalizable because all participating ICUs were in academic hospitals within a single city. Additionally, only patients with ALI were enrolled in this study, and they are not representative of a general ICU cohort because of their high severity of illness. However, we enrolled a total of 514 consecutive patients over a 3-yr period from 11 ICUs at three hospitals, which provides some strength for external validity over smaller single-site evaluations and allowed for some heterogeneity in terms of patient factors and different cultures in the participating hospitals and ICUs. Evaluation in other settings should be undertaken to further evaluate the generalizability of these findings.
Third, the study did not include any data on occupational therapist staffing or ICU culture regarding early rehabilitation in each hospital or ICU. However, no participating ICU or hospital had an early rehabilitation program at the time this study was conducted. More research is needed to further explore the role of ICU staffing and culture in facilitating early occupational therapy rehabilitation. Despite these potential limitations, this study contributes further evidence regarding factors that could affect early occupational therapy intervention in the ICU setting.
Implications for Occupational Therapy Practice
In this multisite study of patients with ALI, we found that only a small proportion of patients had any occupational therapy intervention during their ICU stay.
Severity of patients’ critical illness was a barrier to initiating occupational therapy interventions in the ICU.
Even after adjusting for severity of illness, ICU and hospital factors were associated with timing of occupational therapy initiation, suggesting that the ICU and hospital environment may be modifiable factors to successfully introduce early rehabilitation in the ICU.
Conclusion
In our multisite cohort of patients with ALI, only 30% ever received any occupational therapy intervention during their ICU stay. Patient severity of illness was independently associated with delayed occupational therapy. In addition, ICU sedation practices, type of ICU, and hospital study site also were independently associated with timing of occupational therapy. ICU and hospital practices and culture are potentially modifiable factors to promote earlier rehabilitation in the ICU.
Footnotes
Acknowledgments
This research was supported by National Institutes of Health Acute Lung Injury Specialized Centers of Clinically Oriented Research Grant P050 HL 73994. The funding bodies had no role in the study design, writing of the article, or decision to submit the article for publication. The authors have not disclosed any potential conflicts of interest.
We thank all patients who participated in the study. We acknowledge Benjamin Althouse and Jonathan Gellar, who assisted with statistical analyses for multiple imputation of missing data, and David M. Shade, who critically reviewed a draft of the article.